Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
|
How did they originally diagnose Sickle Cell Disease?
|
Putting a rubber band around a finger will cause hypoxia, causes cells to sickle, go from 15% → 90% sickled
|
|
|
What are the steps of the pathophysiology for Sickle Cell Disease?
|
1) Endothelial activation by SS-RBCs and other inflammatory mediators
2) Recruitment of adherent leukocytes 3) Activation of recruited neutrophils and other leukocytes (monocytes or iNKT cells) 4) Interactions of sickled RBCs w/ adherent neutrophils 5) Vascular clogging by heterotypic cell-cell aggregates composed of SS-RBCs, adherent leukocytes, and possibly platelets 6) Increased transit time to greater than the delay time for deoxygenation-induced hemoglobin polymerization, propagating retrograde vaso-occlusion 7) Ischemia as a result of the obstruction creates a feedback loop of worsening endothelial activation |
|
|
What happens during the first step of Sickle Cell Disease?
|
1) Endothelial activation by SS-RBCs and other inflammatory mediators
|
|
|
What happens during the second step of Sickle Cell Disease after the endothelium is activated?
|
2) Recruitment of adherent leukocytes
|
|
|
What happens during the third step of Sickle Cell Disease after adherent leukocytes are recruited?
|
3) Activation of recruited neutrophils and other leukocytes (monocytes or iNKT cells)
|
|
|
What happens during the fourth step of Sickle Cell Disease after activation of recruited neutrophils and leukocytes?
|
4) Interactions of sickled RBCs w/ adherent neutrophils
|
|
|
What happens during the fifth step of Sickle Cell Disease after the endothelium is activated?
|
5) Vascular clogging by heterotypic cell-cell aggregates composed of SS-RBCs, adherent leukocytes, and possibly platelets
|
|
|
What happens during the sixth step of Sickle Cell Disease after the vascular clogging?
|
6) Transit time becomes greater than the delay time for deoxygenation-induced hemoglobin polymerization, propagating retrograde vaso-occlusion
|
|
|
What happens during the seventh step of Sickle Cell Disease after the retro-grade vaso-occlusion?
|
7) Ischemia as a result of the obstruction creates a feedback loop of worsening endothelial activation
|
|
|
What happens to the vessel wall during Sickle Cell Disease?
|

- Oxidative endothelial cell damage (ROS)
- Increased inflammation - Increased cell adhesion and tissue factor expression - Loss of vasoregulation - Intimal hyperplasia - Platelet and leukocyte adhesion - Propagation of fibrin clot - Entrapment of rigid sickle RBCs - Dysregulation of NO pathway |
|
|
What happens to the RBCs during Sickle Cell Disease?
|

- Sickle-RBC adhesion
- Abnormal shear - Entrapment of rigid sickle RBCs |
|
|
What happens to the plasma during Sickle Cell Disease?
|

- ↑ Serum free hemoglobin
- Propagation of fibrin clot |
|
|
Case: 8 month-old girl w/ SCD was admitted to ED w/ pallor noted by mother. She has not been ill other than a slight cold. She has been a little less active.
On physical examination, where do you look for pallor? |
- Conjunctiva
- Mucous membranes - Palms - Soles |
|
|
Case: 8 month-old girl w/ SCD was admitted to ED w/ pallor noted by mother. She has not been ill other than a slight cold. She has been a little less active.
Her spleen on exam appears to be somewhat enlarged. What questions might you ask of the family? |
- History of enlarged spleen? If they've had it before it is more likely to do it again
- Splenic sequestration? - Is it new? |
|
|
Case: 8 month-old girl w/ SCD was admitted to ED w/ pallor noted by mother. She has not been ill other than a slight cold. She has been a little less active.
What lab studies may be helpful? What's the first thing to order from the lab? |
- Type + Cross-match for blood transfusion
- CBC - Reticulocyte count |
|
|
How do you treat Sickle Cell Disease?
|
Hypoxia, dehydration, and fever increase sickling, so:
- Treat hypoxia with O2 - Give fluids, oral or IV, to prevent dehydration in the cells (enhances sickling) and in the patient - Antipyretics for fever (causes enzymatic reactions to speed up) |
|
|
What should kids with Sickle Cell Disease avoid?
|
- Avoid cold swimming pools and Lake Michigan
- Avoid cold temperatures |
|
|
If you make a diagnosis of splenic sequestration, what therapy is indicated?
|
O2 even if their SaO2 is 99%
|
|
|
Case: 8 month-old girl w/ SCD was admitted to ED w/ pallor noted by mother. She has not been ill other than a slight cold. She has been a little less active.
If you can't palpate the spleen because she was uncooperative, which of the lab studies help you differentiate sequestration from RBC aplasia? |
Reticulocyte count
|
|
|
What is a common life-threatening complication of Sickle Cell Disease? How common / who is most likely to get it?
|
Splenic Sequestration
- Up to 1% of children w/ SCD - SS > SC - Usually infants (as early as 5 weeks) |
|
|
What are the features of Splenic Sequestration in Sickle Cell Disease?
|
- Greater than 2g drop in hemoglobin d/t splenic RBC pooling
- Rapidly enlarging spleen - Can progress to shock and death if untreated - Often recurs |
|
|
What happens to the hemoglobin in Sickle Cell Disease patient with Splenic Sequestration?
|
- Greater than 2g drop
- Caused by splenic RBC pooling |
|
|
How do you treat Splenic Sequestration in a patient with Sickle Cell Disease?
|
- Short term: fluids, oxygen, RBCs / blood transfusion
- Long term: splenectomy (after one or two sequestration events) |
|
|
What are the effects of doing a blood transfusion on a Sickle Cell Disease patient with Splenic Sequestration?
|
- Transfusion reverses process in hours
- Transfuse w/ aim to raise Hemoglobin 3g, may result in rapid shrinkage of spleen - Final Hemoglobin value 2-3g higher than target (d/t RBC/Hb released from spleen |
|
|
How do you prevent / detect early a Splenic Sequestration event in patients with Sickle Cell Disease?
|
- Newborn screening for SCD (all 50 states)
- Teach mom and dad how to feel for spleen at first visit |
|
|
What does Parvovirus B19 infection cause in a Sickle Cell Disease patient?
|
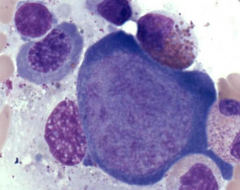
Aplastic Crisis
- Infects erythroblasts in the BM - They will require a blood transfusion to live |
|
|
What is the most likely etiologic agent for a Sickle Cell Disease patient with an aplastic crisis?
|
Parvovirus B19
|
|
|
How do you cure Sickle Cell Disease?
|
Bone marrow transplant
- HLA identical sibling w/ HbAA or HbAS |
|
|
How do you treat Sickle Cell Disease?
|
Transfusion increases HbA and reduces HbS
- HbS <30% prevents stroke recurrence Hydroxyurea (only approved drug) Bone Marrow Transplant to cure from HLA identical sibling who is AA or AS |
|
|
What are the effects of Hydroxyurea?
|
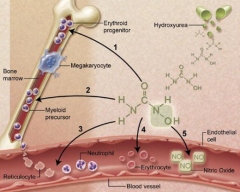
- Decreases sickled cells
- Reduces number of vaso-occlusive incidents - Reduces acute chest incidents - Induction of HbF - ↓ Neutrophil and reticulocyte counts - ↓ Adhesiveness of circulating neutrophils and reticulocytes - ↓ Hemolysis - Nitric Oxide (NO) release w/ local vasodilation and improved vascular response (A→B→C and D→E→F) |
|
|
Case: 3yo Hmong girl presents with microcytic anemia. She has been treated w/ iron with no effect. Her mother also has a history of anemia. The child's screen was positive for Bart hemoglobin consistent w/ a 2 gene deletion.
Why is it important that we order molecular studies to define the alpha gene deletions? |
- There is no clinical difference if genes are deleted in cis or in trans
- But the genetic counseling implications are huge - If deleted in cis and mother or daughter have children with a man who also has similar α-thalassemia trait, potential for HbH disease (if his deletions are trans) or embryonic lethal 4 gene deletion if cis |
|
|
If a patient has cis α-thalassemia trait (2 deletions on same gene), then what are the implications depending on if they mate with someone who also has α-thalassemia trait?
|
- If man has trans deletions: potential for HbH disease
- If man has cis deletions: potential for embryonic lethal 4 gene deletion |