Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
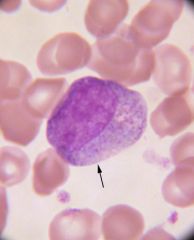
What is the large cell?
|
A myeloblast is a large cell, 12-20 microns in diameter, with a nucleus that takes up most of the cell.
Nuclear chromatin is fine, with little condensation and fairly homogenous in appearance. Nucleoli may vary in number and are apt to be large. The scanty cytoplasm is blue without granules. |
|
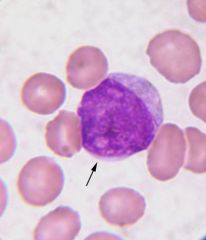
What is this cell?
|
A promyelocyte may be the same size as the myeloblast or even larger. Unlike the myeloblast, the promyelocyte's cytoplasm contains large black or purple granules. Nucleoli may be present.
|
|

What is this cell?
|
The myelocyte is smaller than the myeloblast or the promyelocyte. Unlike the myeloblast and promyelocyte, the myelocyte's cytoplasm contains specific granules, i.e. brick-red (eosinophils), large, blue-black granules (basophils), and lilac granules (neutrophils).
The nucleus still has a round or oval shape and no nucleoli are present. Myelocytes are not seen on a normal peripheral blood smear. |
|
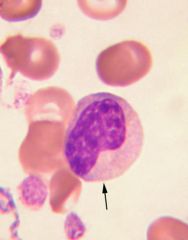
What is this cell?
|
Metamyelocytes (Juvenile) are smaller than the myelocytes. There is more marked clumping of the nuclear chromatin so that the nucleus becomes much denser, takes up less than half the cell volume, and is indented (kidney-shaped).
|
|
|
What is this cell?
|
The band (stab) is similar to the metamyelocyte but the band is smaller and has a horseshoe-shaped nucleus.
The cytoplasm may contain fine lilac granules (neutrophilic), brick-red granules (eosinophilic) or large blue-black granules (basophilic). Bands normally account for 0-5% of the total leukocyte count in circulating blood of the adult. |
|
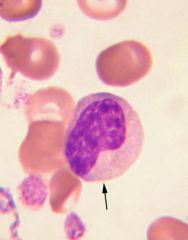
What is this cell?
|
Metamyelocytes (Juvenile) are smaller than the myelocytes. There is more marked clumping of the nuclear chromatin so that the nucleus becomes much denser, takes up less than half the cell volume, and is indented (kidney-shaped).
|
|
What is this cell?
|
The band (stab) is similar to the metamyelocyte but the band is smaller and has a horseshoe-shaped nucleus.
The cytoplasm may contain fine lilac granules (neutrophilic), brick-red granules (eosinophilic) or large blue-black granules (basophilic). Bands normally account for 0-5% of the total leukocyte count in circulating blood of the adult. |
|
What is this cell?
|
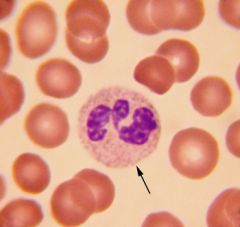
A segmented neutrophil (poly) is approximately 12-14 microns in diameter. This is the final stage of granulocytic development. Normal polys generally have two to five lobes.
Hypersegmented polys, containing six or more lobes, are characteristically seen in megaloblastic anemias. Polys normally account for 45-75% of a normal differential in an adult. |
|
What is this cell?
|
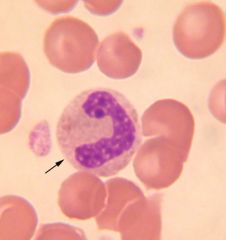
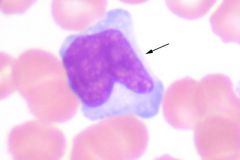
A monocyte has blue-gray cytoplasm and a lobulated nucleus. It's distinguished from other leukocytes by the folding-over of the nuclear lobe (fetal-shaped). 4-11% in a normal blood differential.
|
|
What is this cell?
|
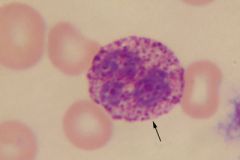
Basophils are present in small numbers (0-3%) in a normal blood smear. Dark coarse granules and indistinct nucleus are characteristic. The basophil is a source of histamine and involved with allergic and inflammatory/immune responses. Increased numbers are seen in myeloproliferative disorders, e.g. chronic myelogenous leukemia and polycythemia vera.
|
|
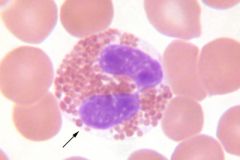
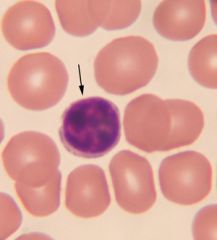
What is this cell?
|
Eosinophils are characterized by the presence of numerous large red-orange granules which will fill the cytoplasm and sometimes cover the nucleus.
0-8% in normal blood, increased in parasitic infections, asthma, hay fever, and many other diseases. |
|
|
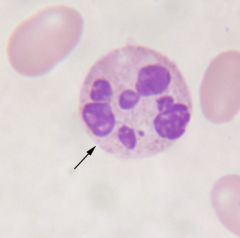
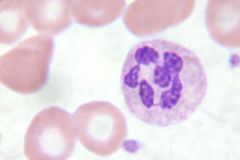
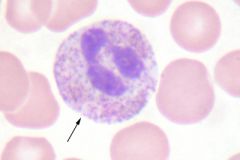
What is this cell? When is it seen?
|
Oil immersion view shows a hypersegmented neutrophil, which has at least six nuclear lobes (the normal neutrophil generally has 2-5 lobes), consistently seen in megaloblastic anemias.
Oval macrocytes and distorted RBC's (poikilocytosis) may also be seen. |
|
What is this cell and when is it seen?
|
Oil immersion view shows a hypersegmented neutrophil, which has at least six nuclear lobes (the normal neutrophil generally has 2-5 lobes), consistently seen in megaloblastic anemias.
Oval macrocytes and distorted RBC's (poikilocytosis) may also be seen. |
|
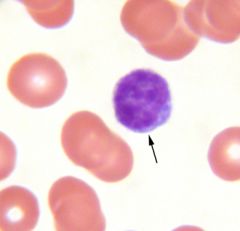
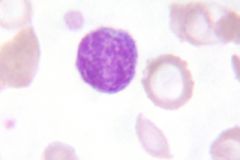
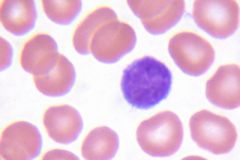
What is this cell?
|
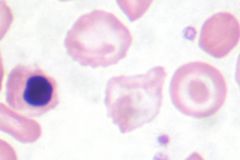
Normal small lymphocyte with its pale blue cytoplasm and dense, dark-staining nucleus.
Note: the size of the nucleus is approximately the same size of normal red blood cells (approximately 7 microns). 16-46% in a normal adult blood smear, increased in infectious mononucleosis, lymphocytic leukemia, and many other diseases. |
|
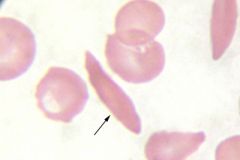
What is this cell?
What causes its distortion? |
Marked distortion of red cell shape is seen in this patient with sickle cell anemia. The sickled form, seen in this image, reflects polymerization of Hgb S molecules and distortion of erythrocyte shape. The patient's hemolysis and increased red blood cell production may also result in the presence of nucleated red blood cells.
|
|
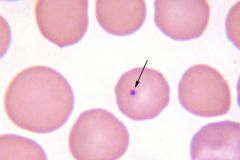
What is this inclusion and when is it seen?
|
Howell-Jolly bodies: Spherical blue bodies (Wright Stain) within or on erythrocytes: nuclear (DNA) debris.
Associated with hyposplenism and pernicious anemia. |
|
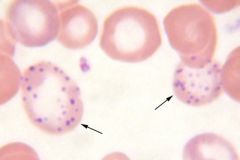
What is this called?
What is the inclusion composed of? What diseases is this associated with? |
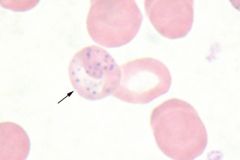
Cells indicated by arrows demonstrate
basophilic stippling. Basophilic stippling represents aggregates of ribonucleoprotein (RNA) and is seen in lead poisoning, thalassemias, and other anemias. |
|
What is this disease process?
What causes this type of anemia? What would you expect MCV to be? What should reticulocyte count be? What shoud platelet count be? Describe expected bone marrow changes. What should serum LDH be? |
Megaloblastic anemias, whether due to vitamin B12 deficiency or folic acid deficiency, present with almost identical morphologic blood and bone marrow changes. Anemia is normochromic and macrocytic - MCV sometimes reaching as high as 150 cubic microns (μ3). Presence of macro-ovalocytes is considered quite characteristic of megaloblastic anemia. The reticulocyte count is usually decreased despite marked anemia.
The so-called right shift of neutrophils (hypersegmented - six or more lobes) typify megaloblastic anemia. Thrombocytopenia is also not uncommon. The bone marrow is hyper-cellular, reflecting predominately the megaloblastic hyperplasia. The megaloblastic changes are noted in all three lines, i.e. red cells, white cells, and platelet precursors within the marrow. Serum B12 and/or folic acid levels and the red cell folate concentration are decreased. Serum lactic dehydrogenase concentration is high. |
|
What type of anemia is depicted here? What are some common causes?
|
A microcytic, hypochromic anemia characterized by decreased hemoglobin, decreased hematocrit, and decreased red cell indices (MCV, MCH and MCHC) is the hallmark of iron deficiency anemia. A moderate degree of anisocytosis (variation in size), moderate to marked poikilocytosis (variation in shape) and significant elliptocytosis frequently accompany moderate and severe degrees of iron deficiency anemia. The leukocyte count is generally normal, whereas the platelet count is frequently increased. The reticulocyte count may be normal or slightly decreased - rarely if ever increased. The bone marrow is normoblastic and depleted of stainable iron. Additional features of diagnostic importance are low serum ferritin, low serum iron, and increased total iron binding capacity (TIBC).
|
|
How would you describe this peripheral smear?
|
Normal red cell morphology.
Note the relative uniformity of size (7-8 microns; approximately the same size as the nucleus of a small lymphocyte) and shape of the red cells and the normal hemoglobin content as evidenced by the central area occupying approximately 1/3 of the cell. |
|
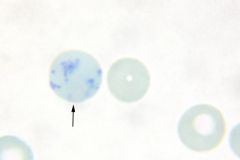
What type of cell is this?
|
Reticulocytes are newly formed erythrocytes.
When stained supravitally with new methylene blue, they contain a blue reticular (RNA) network. These cells appear as macrocytes with diffuse cytoplasmic basophilia (polychromasia) when stained with Wright stain (next image). The normal reticulocyte count: 0.5-2.5%. |
|
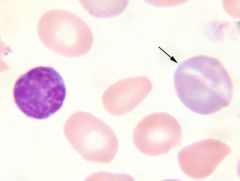
What type of cell is this? When might you see it? Explain its appearance.
|
Polychromatic red cells are somewhat larger than normal and have a faint bluish or grayish-pink color. The color is due to a small amount of RNA.
Significantly higher percentage reflects increased production - same significance as reticulocytes. |
|
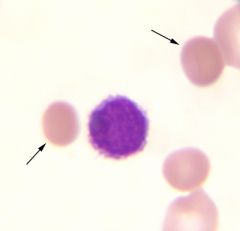
What are the cells indicated by the arrows?
|
This peripheral blood smear shows a number of spherocytes. These cells have a small diameter, and are darker staining than normal. The normal erythrocyte's pale center is absent.
Because of their spherical shape, which is due at least in part to loss of membrane area, they are more susceptible to osmotic stress as measured by the osmotic fragility test. |
|

What is this cell? When do you see it?
|
When the cytoplasm is virtually the same color as a mature non-nucleated red cell, and the nucleus has become very pyknotic or shrunken, the cell is referred to as an orthochromatic normoblast.
Nucleated red cells do not normally appear in the peripheral blood. If they are seen, one must consider a marked increase in marrow erythroid production, i.e. with acute hemorrhage or hemolysis; or a marrow infiltrative process, e.g. with tumor cells or fibrosis. |
|
What is this cell? When would you see it?
|
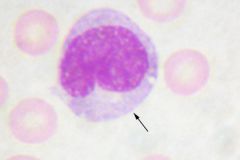
The cells are large with abundant cytoplasm; the nuclei show fine blast-like chromatin pattern. In some cells the cytoplasm may be vacuolated or "muddy". The edges of the lymphocytes are often indented by adjacent red cells.
There is an increased number of atypical lymphocytes in infectious mononucleosis - along with a positive heterophil test and the presence of EB-virus specific antibody. At the beginning of your blood morphology studies, you will probably have difficulties differentiating blast cells from atypical lymphs; and atypical lymphs from monocytes and metamyelocytes. |
|
This blood smear is from a 13 year-old girl who has a hemoglobin of 7.9 gm/dl; MCV, 55.9 µ3; MCH, 20.1 µµg; MCHC of 24%. Her serum iron is 230 µg/dl, total iron binding capacity (TIBC) of 240 µg/dl, and she has increased marrow iron stores.
What disease are these findings consistent with? |
Thalassemia Major
|
|
Your patient's peripheral blood smear is shown above. Based on the cell inclusions, what test might be appropriate?
|
Lead levels in the patient's blood.
|
|
What is this cell?
Infiltration of this cell into bone marrow would indicate what disease? What would a typical clinical presentation include? |
Plasma cell.
Multiple myeloma Older male patient with chronic infections presents with severe back pain. Imaging studies reveal multiple lytic lesions. Urinalysis is positive for Bence-Jones proteins. Patient shows signs of acute renal failure. |
|
What is this cell? What pathologic process does it indicate?
|
This is a neutrophil with toxic granulation: Part of leukocytosis of infection.
|
|
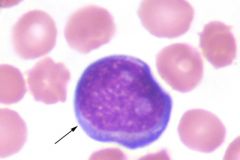
What is this cell?
Excess amounts of this cell in peripheral smear of a child indicates what disease? |
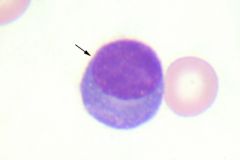
Lymphoblast
ALL - Acute lymphoblastic leukemia |
|
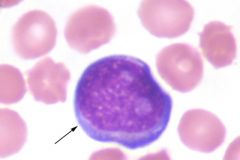
What is this cell? Its presence in excess in an older male's peripheral blood indicates what disease?
|
Mature lymphocyte
CLL - chronic lymphocytic leukemia (most common WBC malignancy) |
|
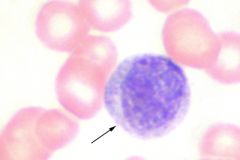
What is this cell?
Excess amounts of this cell in peripheral smear of a child indicates what disease? |
Lymphoblast
ALL - Acute lymphoblastic leukemia |
|
What is this cell?
This 36 year-old patient has a WBC of 85,000/mm3. His differential: 58 neutrophils, 15 bands, 9 metamyelocytes, 10 cells resembling the cell indicated by the arrow, 5 eosinophils, 2 lymphocytes, and 1 monocyte. His leukocyte alkaline phosphatase is low and he has a Ph chromosome. What disease does he have? That translocation does he have? |
Myelocyte
CML t(9;22) |
|
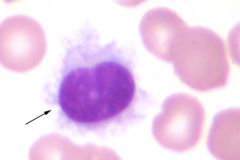
What is this?
|
Hairy cell.
Hairy cell leukemia presentation: This peripheral blood smear is from a 60 year-old patient who has recently had a tendency to bleed easily. On physical examination, a few petechiae were found on his legs. His hemoglobin was 10 gm/dl, hematocrit of 30%, WBC was 7,000/mm3, platelet count of 20,000/mm3, and 40% of his white cells resemble the cell indicated by the arrow. Histochemical studies reveal that these cells contain acid phosphatase resistant to tartrate. |