![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
119 Cards in this Set
- Front
- Back
|
Upper outer quadrant -breast |
Tail of spence |
|
|
Lymphnodes of breast |
Anterior (pectoral) Posterior (subscapular) Lateral (brachial) Central (midaxillary) |
|
|
Breast cancer risks |
Gender Age Early menstruation Genetics 5-10% hereditary Brac Ethnicity Caucasians Early menstruation before 12 Later menopause Dense breast |
|
|
Client education breast cancer risk |
Preventative mammogram age 50 American cancer society recommends yearly mammograms at 40 Having no kids or after 30 Working night shift Second hand smoke Monthly exams |
|
|
Breast self exam |
3 finger pads with left hand for bumps Overlapping some sized circular motion Up down pattern from mid axillary line toward sternum Hands on hips.look for changes in size shape contour dumpling redness of nipple |
|
|
Palpation of breast |
Tumors are usually unilateral with irregular birders hard and non tender Finrocystic breasts feel ropy lumpy and bumpy Nipple discharge Enlarged lumpy more greater than 1 cm may indicate infection |
|
|
Pagets disease |
Rate form of breast cancer in nipple (dry flaky skin around nipple) |
|
|
Gynocamastia |
Smooth firm movable disc of glandular tissue may be seen in one breast in male's during puberty hormonal imbalance |
|
|
Peau d'orange |
Dimpled appearance of skin (skin of orange) seen with inflammatory cancer |
|
|
Retracted nipple or breast tissue |
Suggests malignancy |
|
|
Heart and great vessels review |
Located in mediastinum Size of clenched fist 9oz women 10.9 oz men Anterior chest that overlies heart called precordium Heart is one way system |
|
|
Arteries |
Carry blood away from the heart |
|
|
Veins |
Carry blood to the heart |
|
|
Septum |
Partition that separates left and right side of heart |
|
|
Heart structures |
Right-- pumps blood to lungs for has exchange (pulmonary circulation) pumps unoxygentaed blood (blue side) Left- pumps blood to body (systemic circulation) pumps oxygenated blood (red side) |
|
|
Vena cava & pulmonary arteries and veins |
Superior vena cava-returns blood to rt atrium to upper torso
Inferior vena cava- returns blood to th atrium from lower torso
Pulmonary artery- exits right ventricle bifurcated carries blood to lungs
Pulmonary veins- two from each ling returns oxygenated blood back into left atrium |
|
|
Heart valves |
Tricuspid located between right atrium and right ventricle Mitral located between atrium and left ventricle Pulmonic valve: entrance of pulmonary artery Aortic valve- entrance of aorta |
|
|
Heart regurgitation |
Valve does not close all the way so blood leaks backward toward heart |
|
|
Stenosis |
Valve does not open all the way |
|
|
Automaticity |
Cardiac muscle cells have ability to generate electrical impulse |
|
|
Cardiac cycle |
Process of emptying and filling of the cardiac chambers Two phases: diastole and systole |
|
|
Electrical conduction of the heart |
SA node located on posterior wall of atrium (pacemaker) Generates impulses (60-100) Conduction occurs simultaneously across both atriumss of the heart causing contraction Impulse continues to AV mode Continue to bundle of his Continue to rt and left bundle branches Down perkinje fibers Causes ventricular contraction
If SA node damaged electrical activity shifts to AV node to orignate and rate is 40-60 beats per minute. |
|
|
P wave |
Atrial depolarization conduction of impulse through atria |
|
|
PR interval |
Time from beginning of atrial secularization to beginning of ventricular depolarization ( beginning of P wave to beginning of QRS) |
|
|
QRS complex |
Ventricular secularization (also eatrial depolarization) conduction of impulse through the ventricles causing contraction of ventricles |
|
|
ST segment |
Period between ventricular depolarization and beginning of ventricular repolarization. |
|
|
T wave |
Ventricular repolarization the ventricles return to a resting state |
|
|
QT interval |
Total time for ventricular depolarization and repolarization from beginning of Q wave to T wave do QT varied with heart rate. |
|
|
U wave |
May or may not be present it follows t wave and represents the final phase of ventricular repolarization. |
|
|
PWRST |

P- activation of atria two upper chambers of heart QRS complex is Activation of ventricles Lower chambers T wave is recovery phase |
|
|
Diastole |
Relaxation of ventricles (filling) AV valves open (higher pressure on atria than ventricles) Blood rushes through the atria into ventricles |
|
|
Systole (pumping) |
Contraction of ventricles (emptying) Pressure higher in ventricles than atria AV valves close (S1 sound lub) All four valves close causing aortic and pulmonix valve to open When ventricles empty semilunar valves close causing second heart sound (S2 dub) |
|
|
Heart sounds |
Produced by valves closing S1 result from closure of AV valves (heard best at apex of heart) S2 sound closure of semilunar valves (aortic and pulmonic) heart at base of heart |
|
|
S3 sound |
Ventricular gallop (ventricular diastole) Associated with volume overlad CHF children and young adults Kentucky |
|
|
S4 (atrial gallop) |
Late diastolic atrial filling Uncontrolled hypertension Tenessee |
|
|
Cardiac output |
Amount of blood pumped by the ventricles during a given time (1 minute) Determined by stroke volume wich is the amount of blood pumped from the heart with each contraction SV × HR = CO Normal cardiac output is 5-6L/min |
|
|
Neck vessels |
Carotid- take oxygenated blood to brain Jugular: return blood to heart from neck via superior vena cava Level of jugular vein pressure reflects pressure of RT atrium |
|
|
Coronary artery disease (CAD) |
Build up of day and cholesterol= plaque in coronary arteries Atherosclerosis Areas of heart damaged or dead due to lack of oxygenation and blood flow Leading cause of death in U.S. |
|
|
Neck vessel data collection |
COPD- will have elevated venous pressure during exhalation Jvd= right sided heart failure Acute care- invasive cardiac monitoring used to measure pressures |
|
|
Point of maximal impulse |
Apical impulse Two fingers palpate mitral area Norma- size of nickel 1-2cm small amplitude gentle tap Abnormal- larger than 2cm more forceful longer duration suspect cardiac enlargement Thrill or pulsation associated with grade 4 or higher murmur |
|
|
Pulse rate deficit |
Palpate radial pulse while auscultsting apical pulse Count for full minute If difference detected may indicate atrial fibrillatio. Atrial flutter pvc heart block |
|
|
Coronary arteries |
Right coronary arteries- feeds right side of heart (pumps blood to lungs) Left anterior coronary artery: feeds left side of heart Circumflex coronary artery: feeds left side of heart Left side larger more muscular feeds rest of body |
|
|
Immediate treatment of an MI |
Ischemia of heart Oxygen Nitrates Aspirin Morphine |
|
|
Pericarditis |
Inflammation of perocardioum sticky membranes producing friction rubTreatment: NSAIDs Treatment: NSAIDs |
|
|
Pericardial effussion |
Abnormal accumulation of fluid around the heart sac Cardiac trauma, surgery, vital or bacterial infections Treatment NSAIDs pericarsiocentesis surgery to remove pericardium |
|
|
Cardiac tamponade |
Compression of heart by accumulation of fluid in Pericardial sac Heart surgery trauma heart attack end stage lung cancer Pericarsiocentesis surgery surgery |
|
|
Right sided heart failure |
Most common Right ventricular MI, PE, Pulmonary hypertension Forces blood back into veins Symptoms Dependent edema (pitting) JVD Abnormal distention or ascites Enlarged abdominal organs Hepatomegaly splenomegaly Weight gain from edema Anorexia Extra heart sounds |
|
|
Left sided heart failure |
Fluid backs up to lungs (in air sacs) CAD, MI, systemic hypertension, mitral aortic valve disease
Symptoms SOB Crackles Cyanosis Diaphoresis Fatigue Tacgypnea Blood tinged sputum Nocturia due to renal profusion
|
|
|
Paroxysmal nocturnal dyspnea |
Breathlessness wich wakes patient from sleep Caused by accumulation of alveolar fluid from sleep Open Windows sit on edge of bed |
|
|
Surge |
Arterial pulse felt via palpation of superficial arteries |
|
|
Major arteries |
Brachial Radial Ulnar Femoral Popliteal Posterior tibial Dorsalis pedis |
|
|
Veins |
Deep veins (90% of all blood volume) Superficial (saphenous longest) Communicator veins |
|
|
Venous stasis |
If vein mechanisms impeded (One way valves, muscular contraction, pressure gradients of lungs and abdomen) pooling in legs occur |
|
|
Lymphatic system |
Drains excess fluid and plasma proteins from tissues and returns them to venous system |
|
|
Lymphatic drainage |
Superficial inguinal-legs Epitrochlear-upper arm just behind elbow drains hand and fingers Axillary bodes- under arm |
|
|
Peripheral artery disease |
Reduced blood flow of limbs from atherosclerosis Symptoms: Intermittent claudication= pain when walking improved when activity stops |
|
|
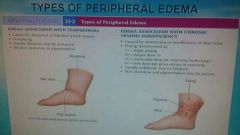
Arterial insufficiency |

Pain, arterial claudication, diminished or absent pulses, cool to touch, hairless shins and feet, dry, shiny skin, ulcers on tips of toes, heels or pressure areas, deep wounds, circular, minimal edema |
|
|
Venous insufficiency |
Pain, aching and cramping minimal. Pulses present, dark pigmentation on lower calf and foot area, reddish blue Brown skin color, ulcers on medial mallous (groove between ankle and Achilles) or tibial area, superficial sound, irregular border, moderate to sever or leg edema, granulation ulcer tissue . |
|
|
Lymphedema |
Blocked lumpy circulation non pitting edema |
|
|
Raynauds |
Vasoconstriction or vasospasm of fingers and toes |
|
|
Allen test |
Patency of radial and ulnar arteries Hands palm side up make fist Use thumbs to occlude arteries Release fist while occluded Release pressure on one artery Repeat on other side Normal coloration returns to palm within 5-15 seconds |
|
|
Superficial thrombophlebitis |
Increased warmth in leg |
|
|
Warning signs of PE |
SOB Rapid breathing Chest pain Rapid heart rate Light headed |
|
|
Homans sign |
Not reliable Tests for dvt Positive if or has extreme pain with dorsiflexion of foot D diner to dx dvt |
|
|
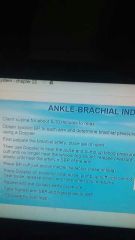
Position change test for arterial or venous insufficiency |
Supine, one forearm under both knees and one forearms under ankles Raise legs 12 inches (above level of heart) Instruct client to pump feet up and down for 1 minute until all venous blood drained Ask client sit up at end of bed legs off side Note color and time it takes to refill Abnornal= marked pallid with legs elevated return of pink color that takes longer than 10 seconds. Persistent rigor (dusky redness) of toes feet and legs dependent |
|
|
Ankle brachial index (ABI) |
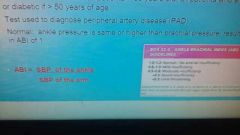
Known as ankle brachial pressure index Greater than 60 years or 50 years and smoke Tests for peripheral artery disease Normal: ankle pressure is same or higher than brachial pressure resulting of ABI of 1 |
|

|
|
|
|
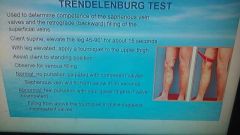
Manual compression test |

|
|
|
Trendelenburg test |
|
|
|
Types of peripheral edema |
|
|
|
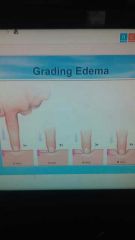
Grading edema |
|
|
|
Solid vicera organs |
Maintain shape consistently Liver pancreas spleen adrenal glands kidneys ovaries |
|
|
Hollow vicera organs |
Structures that change shape depending on their contents Stomach gallbladder small intestine colon bladder |
|
|
Vascular structures of the abdomen |
Abdominal aorta Renal arteries Iliac arteries |
|
|
Peptic ulcer disease |
Open sores that form in the lining of the esophagus stomach or small intestine Can be trasmitted from person to person or food and water
Occurs when acid eats away at the protective mucous covering and erodes the underlying lining
Bacterium heliocopter h pylori usually causes ulcer formation Painful and bleeding, internal bleeding, infection, abdominal pain, burning sensation, fullness, chest pain and black tarry stools fatigue and weight loss |
|
|
Risk for peptic ulcers |
Presence of h pylori Excessive alcohol intake Regular use of ndaids Smoking Radiation Uncontrolled stress |
|
|
Visceral pain |
Hollow abdominal organs contract forcefully or become distended Poorly defined or localized Characterized by full burning colicky or cramping pain |
|
|
Parietal pain |
Parital peritoneum becomes inflamed Appendicitis or peritonitis Localized intense severe pain |
|
|
Referred pain |
Pain perceived at location other than that of original stimulus |
|
|
Cullens sign |
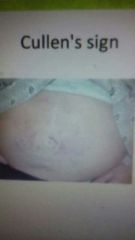
Bluish or purple discoloration around umbilicus indicates intra abdominal bleeding |
|
|
Grey-Turners sign |

Bluish or purple discoloration of the abdominal flanks |
|
|
Umbilicus |
Inverted or protruding no more than 0.5 cm |
|
|
6 Fs causes of abdominal distention |
Fat Feces Fetus Fibroids Flatulence Fluid |
|
|
Peristaltic waves |
Not normally seen. If seen can mean obstruction. |
|
|
Fluid wave test |
Test for secures as client is supine Fluid shift from wall to wall using palms of hands |
|
|
Rebound tenderness |
Palpate at 90° away from tender area and release. If realease hurt more. |
|
|
Blumbergs sign |
Indicates peritonitis (inflammation of peritoneum) of release hurt the most |
|
|
Rovsings sign |
Pain in RLQ when palpating LLQ |
|
|
Obturator sign |
Test for appendicitis Rt knew and ankle held and rotate leg internally and externally Pain in RLQ indicates irritation of obturator muscle due to appendicitis or perforated appendix |
|
|
Cholecystitis |
Inflammation of gall bladder |
|
|
Murphy's sign |
press your fingertips under lives border at rt codtal border and ask client to instigate if accentuated sharp pain that causes patient to hold breath than positive Murphy's sign for cholecystitis |
|
|
Types of muscle |
Skeletal smooth and cardiac |
|
|
Probation and supination |
Pronation- downward Supination- outward |
|
|
Protraction and retraction |
Jaw |
|
|
Internal and external rotation |
Leg bent at knee in or out |
|
|
Gout |
Too much uric acid in blood form crystals on joints especially big tie swelling tenderness and sharp pain on lower extremities Treatment Nsaids and corticosteroids |
|
|
Osteoarthritis |
Occurs when protective cartilage over bones wears down over time Most common Hands knees and spine |
|
|
Temporomamdibular joint (TMJ) |
Clicking or popping is abnormal |
|
|
Kyphosis lumbar lordosis and scoliosis |
Concave Convex Curvature |
|
|
Straight leg test |
Client supine raise leg at point of pain dorsiflex foot |
|
|
Ganglion |
Non tender round enlarged fluid filled cyst |
|
|
Anatomic snuffbox |
Hollow area on back of wrist at base of fully extended thumb Tenderness may indicate scaphoid fracture. |
|
|
Carpal tunnel syndrome CTS |
Medial nerve damage |
|
|
Phalens test |
Rest elbows on table and place back of hands together for 60 seconds of tingling or pain present possible carpal tunnel |
|
|
Tinels test |
Percuss over median nerve if shocking sensation medial nerve entrapped possible carpal tunnel |
|
|
Flick signal |
Vigorously shake hands for 30 seconds Numbness or tingling after 30 seconds abnormal |
|
|
Thumb opposition test |
Carpal tunnel syndrome |
|
|
Swan neck deformity |
Seen with long term rheumatoid arthritis |
|
|
Bouttonieres deformity |
Long term rheumatoid arthritis "button swelling in joints" |
|
|
Osteoarthritis |
Hard painless nodules on joints |
|
|
Heberdens nodes |
Over distal joints |
|
|
Bouchards nodes |
Over proximal joints |
|
|
Ballotement test |
Assess fluid in patella Squeeze top and push on bottom of knee |
|
|
McMurrays test |
If client complains of giving in or locking of knees Rotate lower leg and foot laterally while holding knee slowly extend noting clicking or pain |
|
|
Corns |
Painful thickening of bony prominence on feet |
|
|
Callussess |
Non painful thickened skin that occur at pressure points |
|
|
Plantar wart |
Painful wart |
|
|
Hammer toe |
Hyperextension at metatarsophalangeal joint 28th flexion at the proximal interphalangeal joint |
|
|
Hallux valgus |

Abnormality in wich the great tie is deviated laterally and may overlap the second toe |