Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
128 Cards in this Set
- Front
- Back
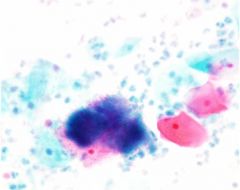
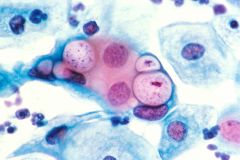
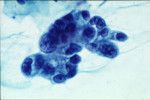
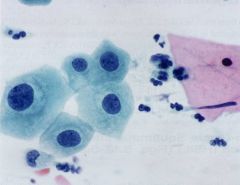
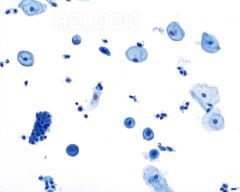
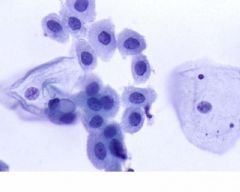
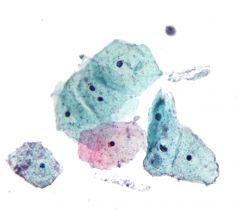
pap smear
|
actinomyces, associated with IUD - IUD cells can mimic HSIL but have smooth nuclear membranes, washed out chromatin
|
|
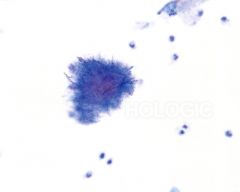
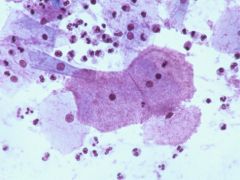
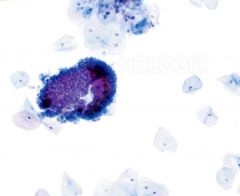
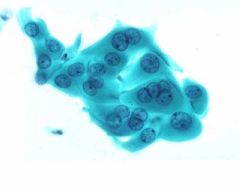
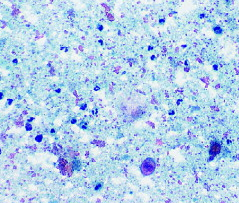
pap smear
|
actinomyces IUD assoc- IUD cells can mimic HSIL but have smooth nuclear membranes, washed out chromatin
|
|
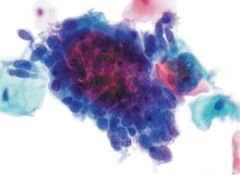
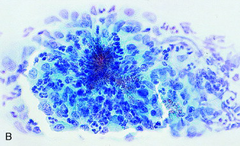
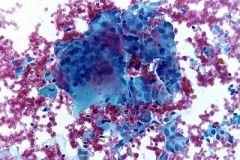
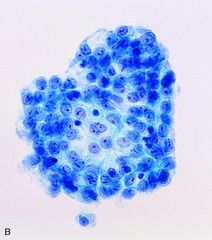
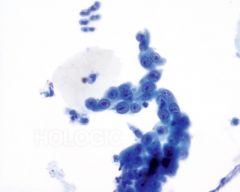
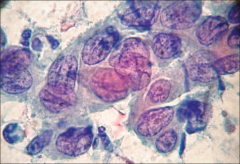
pap smear
|
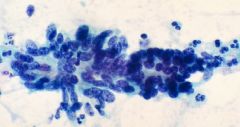
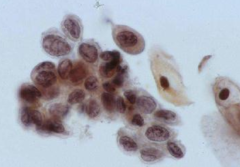
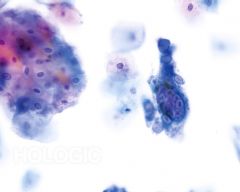
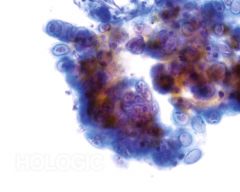
AIS - feathering, rosettes, gland like
|
|
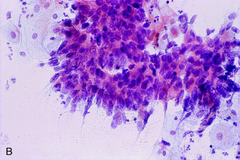
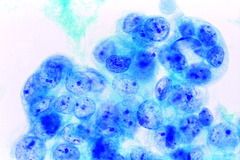
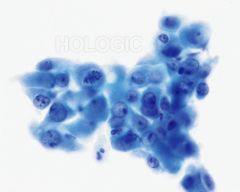
pap smear
|
AIS - feathering, rosettes, gland like
|
|
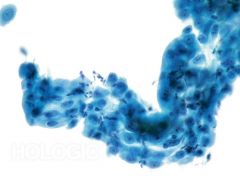
pap smear
|
AIS - feathering, rosettes, gland like
|
|
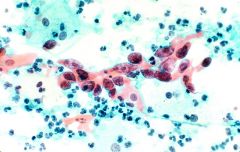
pap smear
|
ariasstella, pregnancy
|
|
pap smear
|
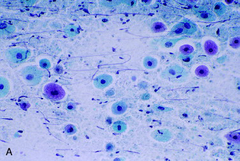
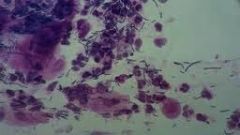
atrophy - dark blue blobs, degenerated parabasals, granular background
|
|
pap smear
|
atrophy - dark blue blobs, degenerated parabasals, granular background
|
|
pap smear
|
atrophy - dark blue blobs, degenerated parabasals, granular background
|
|
pap smear
|
atypical parakeratosis - in regular parakeratosis - pyknotic nuclei and hypereosinophilic cytoplasm
|
|

pap smear
|
benign keratin pearl
|
|
pap smear
|
candida - skewered
|
|
pap smear
|
chronic follicular cervicitis
|
|
pap smear
|
chylamydia
|
|
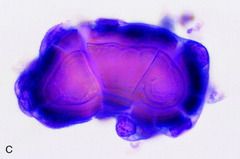
pap smear
|
cockleburr crystals - no clinical significance, found with pregnancy
|
|

pap smear
|
cockleburrs - no clinical significance, found with pregnancy
|
|
pap smear
|
endometrial cells - occasional kidney bean shaped nuclei
|
|
pap smear
|
endometrial cells- occasional kidney bean shaped nuclei
|
|
pap smear
|
endometrial ca - usu no tumor diathesis on Pap, single cells, vacuoles, prominent nucleoli
|
|

pap smear
|
endometrial ca- usu no tumor diathesis on Pap, single cells, vacuoles, prominent nucleoli
|
|
pap smear
|
endometrial ca- usu no tumor diathesis on Pap, single cells, vacuoles, prominent nucleoli
|
|

pap smear
|
endometrial cells - occasional kidney bean shaped nuclei
|
|
pap smear
|
clue cells - usu relatively clean backgroun, treatment is metronidazole
|
|
pap smear
|
granuloma
|
|
pap smear
|
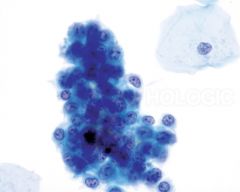
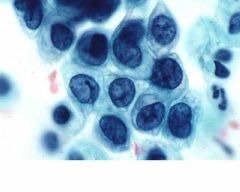
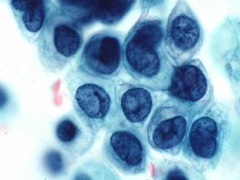
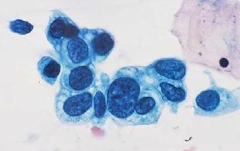
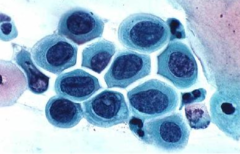
HSIL - 3x nuclei of intermediate cell, 1 nuclei fits into cytoplasm
|
|
pap smear
|
HSIL- 3x nuclei of intermediate cell, 1 nuclei fits into cytoplasm
|
|
pap smear
|
HSIL- 3x nuclei of intermediate cell, 1 nuclei fits into cytoplasm
|
|
pap smear
|
HSIL- 3x nuclei of intermediate cell, 1 nuclei fits into cytoplasm
|
|
pap smear
|
HSIL- 3x nuclei of intermediate cell, 1 nuclei fits into cytoplasm
|
|
pap smear
|
HSIL- 3x nuclei of intermediate cell, 1 nuclei fits into cytoplasm
|
|
pap smear
|
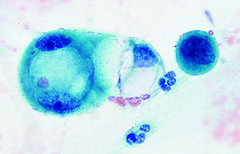
HSV
|
|
pap smear
|
HSV
|
|
pap smear
|
HSV
|
|
pap smear
|
IUD effect - mimics HSIL, but round nuclear membranes, fine chromatin pattern
|
|
pap smear
|
lactobacilli - often bare nuclei
|
|
pap smear
|
leptothrix- often found with trich
|
|
pap smear
|
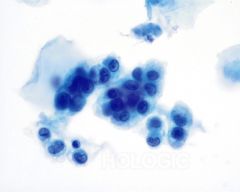
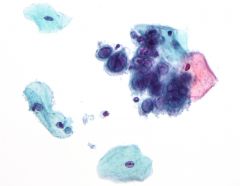
LSIL - 3 x nuclei of intermediate cell with 2 or more nuclei fitting into cytoplasm, perinuclear cavity, rolled up thick cytoplasm
|
|
pap smear
|
LUS
|
|

pap smear
|
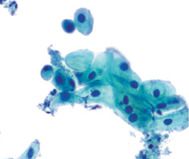
endocervical cells
|
|
ovarian
|
ovarian serous borderline
|
|
ovarian
|
ovarian serous ca
|
|
pap smear
|
postpartum - can be yellow staining glycogen or single parabasals
|
|
pap smear
|
psammoma
|
|
pap smear
|
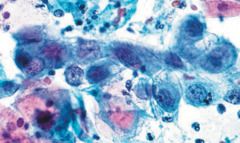
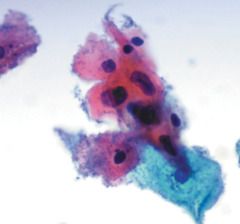
radiation - two tone cytoplasm, increase cellular size, increase nuclei but also cytoplasm, multinucleation, vacuolization of cytoplasm and increased pmns (last two go away with time)
|
|
pap smear
|
radiation- two tone cytoplasm, increase cellular size, increase nuclei but also cytoplasm, multinucleation, vacuolization of cytoplasm and increased pmns (last two go away with time)
|
|
pap smear
|
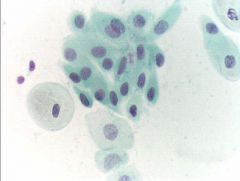
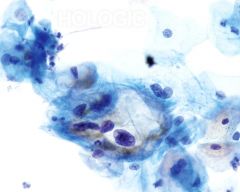
repair - no hyperchromasia persay but increase nuclear size, school of fish, not really single cells
|
|
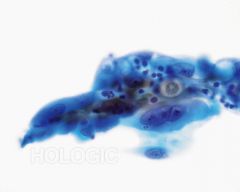
pap smear
|
repair no hyperchromasia persay but increase nuclear size, school of fish, not really single cells
|
|
pap smear
|
repair - no hyperchromasia persay but increase nuclear size, school of fish, not really single cells
|
|
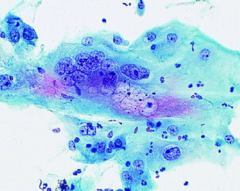
pap smear
|
invasive scca - tadpoles, single cells, tumor diathesis, prominent nucleoli
|
|
pap smear
|
squamous metaplasia - dense cytoplasm, fine chromatin, interlocking parabasals, active nuclei (chromocenters present),streaming but cookie cutter
|
|
pap smear
|
squamous metaplasia - dense cytoplasm, fine chromatin, interlocking parabasals, active nuclei (chromocenters present),streaming but cookie cutter
|
|
pap smear
|
squamous metaplasia - dense cytoplasm, fine chromatin, interlocking parabasals, active nuclei (chromocenters present),streaming but cookie cutter
|
|

pap smear
|
surepath, sedimentation
|
|

pap smear
|
thinprep liquid based smear
|
|
pap smear
|
transitional metaplasia
|
|
pap smear
|
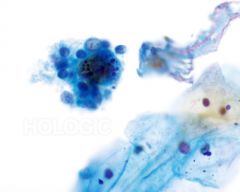
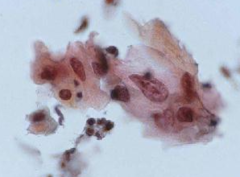
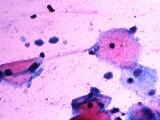
trich- reactive type haloes, associated with leptothrix, treated with metronidazole, fuzzy pear shapes
|
|
pap smear
|
tumor diathesis
|
|
|
sufficient number of cells for liquid based Pap smear
|
5000
|
|
|
sufficient number of cells for conventional Pap smear
|
10,000
|
|
|
where is the HPV virus in invasive SCCa
|
integrated into genome
|
|
|
what is the nuclear size of LSIL cells compared to intermediate cell
|
3x
|
|
|
how many nuclei fit into the cytplasm in a LSIL cell
|
two or more
|
|
|
how many nuclei fit into the cytoplasm in an HSIL cell
|
1
|
|
|
what is the nuclear size of an HSIL cell compared to an intermediate cell
|
3x
|
|
|
learn the cyto stains
|
diffiquik, etc and their artifacts
|
|
|
describe the Digene II process
|
RNA probe targets vDNA with an antibody to these together with an associated light emission probe
|
|
|
learn the recommendations for screening
|
for Pap vs. HPV
|
|
|
when to report endometrial cells
|
>40 years, >12 days past LMP
|
|
|
what is the frequency of progression to invasive ca for LSIL
|
<1%
|
|
|
what is the frequency of progression to invasive SCCa from HSIL
|
CIN II - 5%
CIN 3 - 12% |
|
|
when is the earliest one should colpo postpartum
|
>6 weeks
|
|
|
what are the daughters of DES use at risk for
|
vaginal adenosis, clear cell carcinoma
|
|
|
of HPV early genes, what binds what
|
E6 binds p53
E7 binds rb |
|
|
low risk HPV types
|
6, 11, 42-44, 53,54, 57, 66
|
|
|
high risk HPV types
|
16, 18, 31-35, etc
|
|
|
how to distinguish on Pap between mets to cx vs. direct extension to cx
|
mets to cx - no tumor diathesis
direct extension to cx - tumor diathesis can be seen |
|
|
one useful identifier of mesothelial cells in pelvic washing
|
mesothelial cells have a prominent nucleoli
|
|
|
what is the mesothelial skirt made of
|
made of ectoplasm and endoplasm (perinuclear organelles)
|
|
|
how does HMBE-1 compare to calretinin in staining mesothelial cells
|
HMBE1 is less specific but as sensitive as calretinin
|
|
|
learn more about thin prep/sure path
|
- process
- differences |
|
|
what affect does alcohol fixation in a Pap smear have on cells
|
smaller cellular size
|
|
|
compare histologic fx of HSIL vs. invasive SCCa on Pap smear
|
in HSIL you really shouldn't see prominent nucleoli and definitely not tumor diathesis
|
|
|
what is the specificity and sensitivity of a Pap
|
sensitivity - 47%
specificity 95% |
|
|
where might you see a reallly granular/dirty background
|
atrophic vaginitis
|
|
|
what percent of cases should be ASCUS coming out of an individual lab
|
5%
|
|
|
what should the ASCUS/SIL ratio be coming out of a lab
|
less than or equal to 3:1
|
|
|
three indications for colpo
|
LSIL, HSIL, ASC-H
|
|
|
compare histologic fx of repair vs. invasive SCCa
|
repair - fine chromatin, flat sheets but cohesive cells
invasive SCCa - coarse chromatin, marked crowding, single cells |
|
|
How often does ASCUS lead to HSIL on biopsy
|
10-20%
|
|
|
what percent of Paps are nl
|
91%
|
|
|
compare exfoliated EM cells vs. HSIL
|
HSIL cells are larger and in flatter sheets
|
|
|
what % of LSIL cells will regress
|
50%
|
|
|
what is the most common cause of small cell ca of the cx
|
HPV 18
|
|
|
maturation indices for 1 hour old child
|
95-5 - Intermediate and superficial
|
|
|
maturation indices for child
|
80- parabasals
20- intermediates |
|
|
maturation indices for menstruating females
|
40-60 intermediate-superficial if premenses
70-30 intermediate-superficial if in menses |
|
|
maturation indices for OCP use
|
95-5 intermediate-superficial
|
|
|
maturation indices for postmenopausal
|
100 -0-0 parabasal/intermediate vs. superficial
|
|
|
what's a normal vaginal pH
|
4.5
|
|
|
what do anucleated squames mean
|
contamination from vulva or leukoplakia in vagina
|
|
|
describe nuclei and cytoplasm of endocervical cells
|
definite chromatin detail is seen and nucleoli are evident; cytoplasm is more delicate and foamy but size of endocervical nuclei are slightly larger than seen for squames (2n intermediate cell)
|
|
|
most accurate e2 indices come from where
|
lateral wall of vagina
|
|
|
what is leptothrix
|
filamentous bacteria - strings of spaghetti
|
|
|
fx you might find in a histological picture with trich
|
- associated inflammation
- reactive haloes - shot gun pmns - grey background |
|
|
if you hear a clinical story of a pregnant woman in her 3rd trimester and see radiation-like changes in her Pap smear, what should you think of
|
folate deficiency
|
|
|
if you've had radiation, how long should you wait before a pap smear
|
~2 months
|
|
|
what histo fx should you think of with OCP
|
parakeratosis
|
|
|
if you see parakeratosis, what should you think of clinically
|
OCP use
|
|
|
what histologic fx do you see with Chylamydia
|
- intracytoplasmic bugs
- lymphocytic cervicitis (+ tingible body macs) |
|
|
where do you find alternaria
|
water contaminant
|
|
|
what is the depth of invasion required to call an invasive scca microinvasive
|
less than or equal to 3 mm
|
|
|
appearance of air-dried artifact
|
hazy, grey
|
|
|
compare repair vs endocervical adenocarcinoma
|
repair - macronucleoli; endocervical adenoca - micronucleoli
repair fine granular chromatin; endocervical adenoca - coarse repair cellular aggregates; endocervical adenoca - isolated or syncytial repair - inflammation, endocervical adenoa - more clean background repiar - often well-defined cell borders, endocervical adenoca - overlapping of cells with little cytoplasm |
|
|
compare repair to large cell in situ
|
repair - aggregates, fine chromatin, macronucleoli, cell borders
large cell in situ - isolated, coarse chromatin, less common macronucleoli, less distinct cell border |
|
|
criteria for ASCUS
|
1. nucleus 2-3 x cross diameter of intermediate cel
2. chromatin: increased, even, no granularity 3. number of affected cells 3-5 |
|
|
specimen adequacy
satis for evaluation |
1. appropriate labeling, clinical data
2. adequate # cells (covers >10% slide) 3. adequate t zone (2 clusters of 5 or more cells) 4. endocervicals or lots of metaplasitics |
|
|
specimen adequacy:
satis but limited by can include |
- lack of pertinent info.
- partially obscuring blood, inflammation, thick area (precluding interpretation of 50-75% of slide) - no endocervical cells |
|
|
if see a psammoma, what should you do
|
look further - may see papillary clusters s/o ovarian
|
|
|
tricky slide: melanoma
|
may hide pigment, grey background
|
|
|
when to start screening
|
21 years, 3 years post first intercourse
|
|
|
how often to screen - age dependent
|
21-30: conventional/q year, LBP every 2
30-70: if nl 3x/q 3yrs (if HPV), q 2yrs if not HPV 70: can stop if negative for 10 years can stop if no uterus if DES/iC must do every year |
|
|
when testing HR or LR HPV types
|
HR only
|
|
|
in whom do you do HPV genotyping?
|
30+
|
|
|
what are the two relevant parameters for reporting endometrial cells
|
>12 days post LMP
>40 years |
|
|
if see clue cells, what do you treat with
|
metronidazole
|
|
|
if see trich, what treat with
|
metronidazole (+sexual partner) - remember,with trich can see small halo
|
|
|
what buys an adolescent a colpo
|
HSIL (arguable with ASC-H)
|
|
|
when do you colpo a pregnant person
|
ONLY if invasive cancer; no colpo until 6 wks postpartum
|