![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back

Ovarian mass. What should you be concerned about? |
endometrial hyperplasia or carcinoma due to unopposed estrogen production
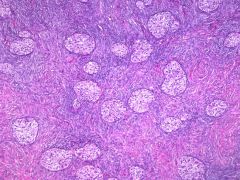
Fibrothecoma |
|
Ovarian lesion
|
Struma ovarii in a teratoma
|
|
|
What distinguishes benign from malignant smooth muscle tumor of the uterus?
|
Coagulative necrosis
|
|
|
Melanoma is measured how?
|
From the surface of the epithelium (discounting acellular keratin layer) to the deepest portion of the tumor.
|
|
|
SCC depth of invasion is measured how?
|
Measured from adjacent basement membrane of the closest dermal papillae.
|
|
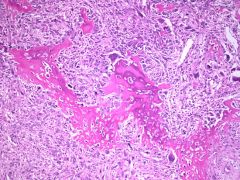
The uterine lesion illustrated is:
|
Malignant mixed mullerian tumor, heterologous
sarcomatous component heterologous: muscle, cartilage, osteoid, fat homologous: endometrial stromal sarcoma, leiomyosarcoma |
|
|
Hydatidiform mole is txed by?
|
Evacuation of uterus and serial beta-hCG titers
|
|
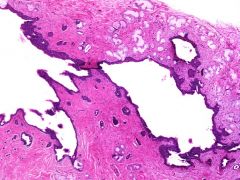
Ovarian lesion
|
Mucinous cystadenoma
|
|
Ovarian lesion
|
Serous cystadenoma
|
|
Vulvar lesion showed the following IHC profile: CK7+, CK20-, CEA+, GCDFP-15+, HMB-45-, Uroplakin III-,
Most likely dx? |
Paget's disease
|
|
This endometrial lesion is ?
|
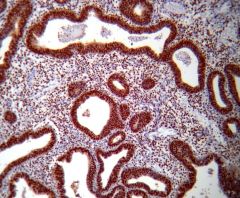
Simple hyperplasia w/out atypia
PTEN strong and diffuse staining |
|
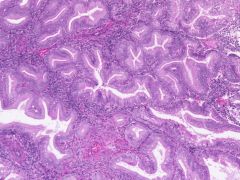
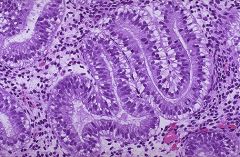
This endometrial lesion is?
|
Complex hyperplasia w/out atypia
|
|
This ovarian lesion was excised. The patient can be best followed up with which of the following serum markers?
|
AFP
yolk sac carcinoma/endodermal sinus tumor |
|
|
Most common malignancy arising out of a benign teratoma?
|
Squamous cell carcinoma
|
|
|
FIGO grade 1
FIGO grade 2 FIGO grade 3 |
FIGO grade 1 Well-differentiated: 0-5% solid tumor
FIGO grade 2 Moderately differentiated: 6%-50% of nonsquamous tumor is solid FIGO grade 3 Poorly differentiated: >50% of nonsquamous tumor is solid |
|
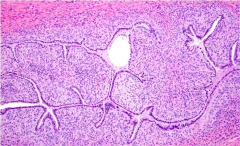
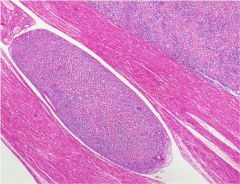
What is this lesion in the ovary?
What other tumor may develop? What chromosome do patients carry? |
gonadoblastoma
dysgerminoma (seminoma) Y chromosome Does not metastasize |
|
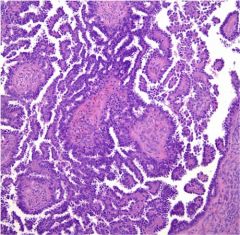
What are the distinctive structures shown?
Dx? Associated w/? Tumor cells + for what stains? |
Call-Exner bodies
granulosa cell tumor 75% associated w/ hyperestrinism which may cause endometrial hyperplasia. Calretinin+, EMA- Usually presents Stage 1 |
|
What is the most reliable diagnostic feature distinguishing this lesion from the more aggressive neoplasm arising from this tissue type?
|
Serous borderline tumor
Lack of stromal invasion |
|

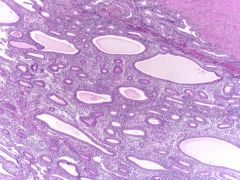
Vaginal bx
|
Adenosis
•Adenosis present in 35% to 90% after in utero exposure to DES, taken by pregnant women until 1971 in USA. |
|
Endometrial curettage from a 26-yo woman. What is this?
|
Arias-Stella reaction
|
|
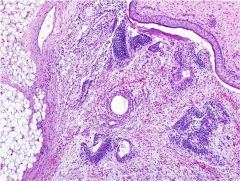
Vulvar cyst at 4 o'clock position at the introitus. Most likely dx?
|
Bartholin duct cyst
Located at 4 and 8 o'clock position at introitus |
|
Ovarian lesion
|
Brenner tumor
urothelial markers + |
|
Endometrial bx shows ?
|
Day 16-17 secretory endometrium
|
|

Most common origin of ovarian lesion w/ these features?
|
GI tract
Metastatic signet ring cell adenocarcinoma of ovary |
|
|
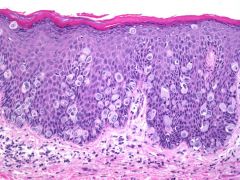
Differentiated VIN
|
Occurs in older patients.
Not HPV related. Greater risk of progression to invasion than common basaloid/warty HPV-related VIN lesion. |
|
|
Paget's disease of the vulva frequently recurs after excision. Why?
|
Microscopic lesion often extends beyond grossly visible lesion.
|
|
|
Sarcoma botyroides of the vagina occurs in predominantly what age group?
Sarcoma boytroides of the cervix occurs in what age group? |
Children <5 yrs
teens - young adults |
|
|
Most CIN lesions arise from ?
|
Transformation zone of cervix
|
|
|
FIGO definition of microinvasive SCC of cervix
|
Stage IA1: tumor <3 mm deep and <7 mm wide.
Stage IA2: tumor 3-5 mm deep and <7 mm wide |
|
|
Histologically benign glands in malignant stroma.
|
Mullerian adenosarcoma
|
|
|
Tumor of the uterus that is not related to unopposed estrogen.
|
Uterine serous carcinoma
|
|
|
17-yo pt w/ large ovarian mass. Origin of tumor is most likely?
|
Germ cell
|
|
|
Conditions associated w/ tubal ectopic pregnancy.
|
Salpingitis isthmica nodosa
Chlamydial infection Follicular salpingitis IUD |
|
How are immature teratomas of the ovary graded?
|
Grade 1: Immature neuroepithelium occupying <1 LPF (4x obj) on the worst slide.
Grade 2: Immature neuroepithelium occupying no more than 3 LPFs on the worst slide. Grade 3: immature neuroepithelium occupying >3 LPFs on any slide. |
|
|
Least common type of twin placenta
|
Monoamniotic monochorionic
|
|
|
Partial mole vs. complete mole
|
Partial triploid, complete diploid (paternal only)
Partial mole has lower risk of progression to gestational trophoblastic neoplasia. Partial mole has less pronounced trophoblast proliferation. Partial mole may be inadvertently dxed as missed abortion by both clinician and pathologist. |
|
|
What stain can distinguish complete from partial hydatidiform moles?
|
p57^kip is expressed from maternal allele in most tissues. Therefore, it is underexpressed in complete moles. Syncytiotrophoblastic cells are nonreactive and maternal decidualized stromal cells are strongly reactive in all types of gestations.
|
|
|
What stain can distinguish inflammatory atypia of the cervix from CIN?
|
Ki-67 stains upper layers of epithelium in CIN and condyloma accuminatum and is confined to basal layer in normal squamous.
|
|
|
What stain can distinguish differentiated VIN from squamous cell hyperplasia of vulva
|
VIN is likely to show nuclear p53+ while squamous hyperplasia does not.
|
|
|
What stain can distinguish smooth muscle neoplasm of uterus from endometrial stromal lesion?
|
Smooth muscle neoplasms typically h-caldesmon+. Endometrial stromal lesion CD10+, h-caldesmon-.
|
|
|
What stain can distinguish endometrial carcinoma from endocervical carcinoma?
|
HPV+ (&/or p16) and ER-, vimentin- favors endocervical.
ER+, vimentin+ and HPV- favors endometrial. |
|
Mass removed from the cervix.
|
Glassy cell carcinoma
younger age group, mean age 40 yrs Associated w/ pregnancy, HPV 16 &18 Peripheral blood eosinophilia Prominent eosinophilic inflammatory infiltrate |
|
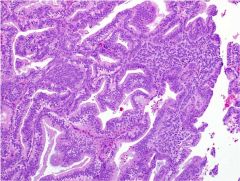
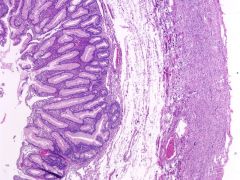
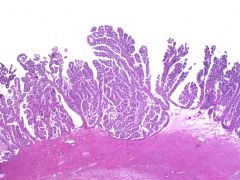
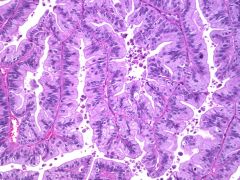
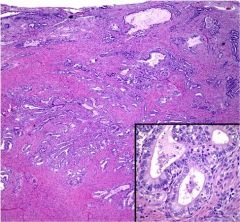
exophytic mass in the endometrial cavity of a 55-year-old woman who underwent a total abdominal hysterectomy and BSO
|
Endometrioid adenocarcinoma
|
|
an incidentally found 1.3-cm myometrial nodule in a hysterectomy specimen obtained from a 47-year-old woman
|
Adenomatoid tumor
|
|
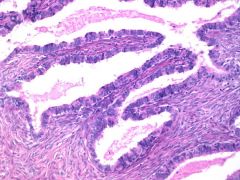
endometrial polyp fragment obtained during an endometrial curettage
|
The image depicts well-spaced glands in a myomatous stroma. Squamous morular metaplasia is conspicuous. In the setting of a polyp, these findings are most consistent with an atypical polypoid adenomyoma.
|
|
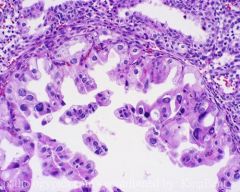
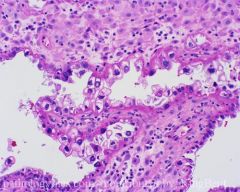
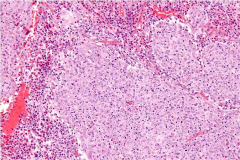
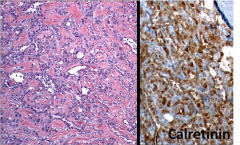
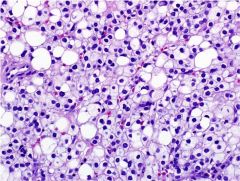
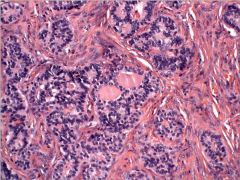
ovarian mass. The tumor cells are immunoreactive for calretinin and negative for EMA.
|
The nuclei are round and nuclear grooves (a prominent feature in adult granulosa cell tumors) are not seen. The calretinin(+)/EMA(-) is consistent with a sex cord-stromal tumor, specifically, a juvenile granulosa cell tumor.
|
|
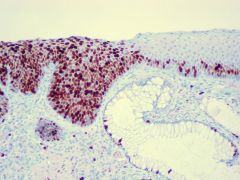
The image provided represents a section of a cold-knife cone biopsy obtained from a 29-year-old woman with a history of glandular dysplasia on Papanicolaou smear. What HPV subtypes are associated w/ this entity?
|
At least 90% of cervical adenocarcinomas contain human papillomavirus and types 16 and 18 account for approximately 80-90% of cases.
|
|
|
What is the most common histologic subtype of Müllerian malignancy observed in women with known BRCA mutations?
|
high-grade serous carcinomas
|
|
The image depicts a section of an infiltrative uterine mass resected from a 74-year-old woman who initially presented with postmenopausal bleeding. Molecular analysis revealed evidence for the presence of a t(11;22)(q24;q12) translocation. What is the usual presentation of this tumor?
|
Extrauterine involvement by the tumor at presentation is common.
Post menopausal women, poor prx |
|
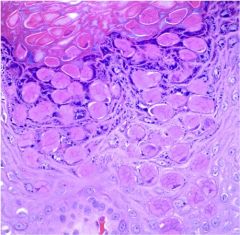
What is this disease and how is it transmitted?
|
Molluscum contagiosum
Direct contact, often sexually transmitted. DNA poxvirus (Molluscipoxvirus genus) These lesions typically present as painless, dome-shaped papules with or without central umbilication and can present in both immunocompetent and immunocompromised individuals. |
|
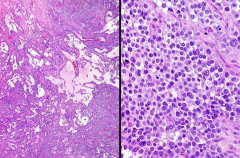
The image depicts a representative section of a polypoid uterine mass removed from a 68-year-old woman. What histologic feature portends a poor prognosis?
|
Adenosarcoma
Myometrial invasion and especially sarcomatous overgrowth in adenosarcoma is associated with a poor prognosis. |
|
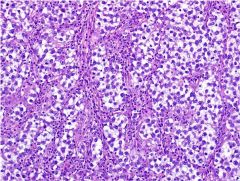
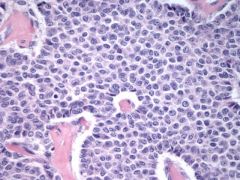
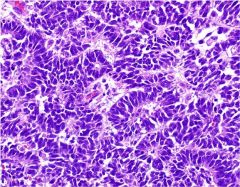
The image depicts a representative section of a 14.2-cm ovarian mass removed from a 19-year-old woman. These tumors are bilateral in what % of cases? What serum levels are elevated?
|
Dysgerminoma bilateral 15% of cases.
LDH increased |
|
The image depicts a representative section of a cystic right ovarian mass obtained from a 67-year-old woman. What feature is most likely to be associated with a worse clinical outcome?
|
Presence of invasive implants in the peritoneum
Serous borderline tumor with micropapillary architecture |
|
The photomicrograph is representative of a uterine mass removed from a 55-year-old woman who presented with post-menopausal bleeding. Immunohistochemistry reveals that the tumor cells are + for SMA & HMB45 while negative for S100, desmin, and CK7. What is the most likely diagnosis?
|
Perivascular epithelioid cell tumor
PEComa |
|
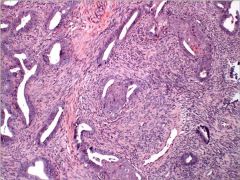
The image depicts a representative section from a hysterectomy specimen removed for uterine fibroids from a 49-year-old woman. What is this?
|
This is a cytologically bland smooth muscle proliferation that extends into intravascular spaces, c/w INTRAVASCULAR LEIOMYOMATOSIS (IVL). Tumor can extend into the veins of the broad ligament and can even extend into the IVC resulting in sxs such as dyspnea & syncope. Cytogenetically, similar karyotypic abnormalities are observed in IVL as in uterine leiomyomas; specifically, der(14)t(12;14)(q15;24). Hence, IVL is considered to be related to uterine leiomyomata of the usual type.
|
|
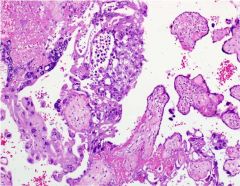
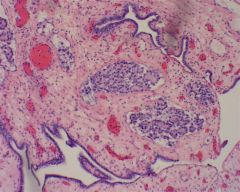
The image depicts an incidentally found intraplacental nodule from a term placenta associated with a normal pregnancy that resulted in the birth of a healthy baby boy. What is this entity?
|
intraplacental choriocarcinoma
This is rare in placentas & when discovered grossly often described as infarcts. Beta-hCG levels should be monitored in the mother & infant to determine whether further metastatic evaluation is indicated. Maternal metastases can be encountered but metastases in the infant are rare; hence, infants fare well. Choriocarcinoma is typically managed by chemotx w/ an overall disease-free survival approaching 90%. |
|
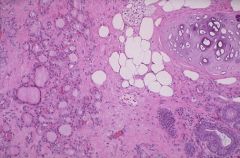
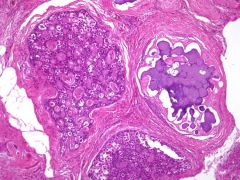
The photomicrograph depicts the only finding in the right ovary of a total abdominal hysterectomy and bilateral salpingo-oophorectomy specimen obtained from a 41-year-old woman. What is this associated w/?
|
Keratin granulomas seen in association with endometrioid adenocarcinomas of the uterus that exhibit squamous differentiation
|
|
|
Gynandroblastomas are defined as a combination of which two tumor elements?
|
Granulosa cell and Sertoli cell
|
|
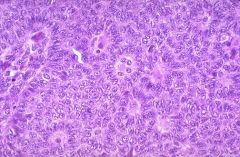
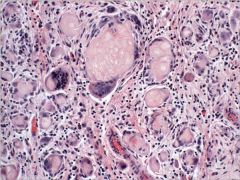
The image depicts a representative section of an ovarian tumor removed from a 41-year-old woman. |
This is a trabecular carcinoid tumor admixed with thyroid follicles, c/w a dx of strumal carcinoid. 60% of cases, there is a coexisting mature cystic teratoma and bilateral ovarian disease is seen in approx 10% of cases. These tumors are almost always benign & are associated with carcinoid sxs in rare instances.
|
|
|
On Pap test screening superficial cells predominate in what setting? |
Preovulation (estrogen) Estrogen-secreting tumors hormone replacement Cirrhosis (lack of estrogen metabolism) |
|
|
On Pap test screening intermediate cells predominate in what setting? |
Progesterone-rich Pregnancy Post-ovulation Newborn girls |
|
|
On Pap test screening parabasal cells predominate in what setting? |
Postmenopausal Premenarche Postpartum especially lactation |
|
|
Cytopathologists and cytotechs can perform primary screening of how many slides in what time period? |
100 pap tests in an 8-hour period is the limit (12.5 tests/hour) Number of 2ndary reviews is not regulated. |
|
|
According to ClIA '88 random rescreen of what %age of all negative Pap tests is required? What happens for all Pap tests for HSIL or worse? |
10% Review of histologic biopsy correlation for HSIL or worse and review of all prior negative Pap tests in the 5 years prior to the 1st interpretation of HSIL or worse. |