![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
80 Cards in this Set
- Front
- Back
|
Normal series of events in cough mechanism |
-Deep inhalation, closure of glottis, active contraction of expiratory muscles, and glottis opening -Deep inhalation increases the lung volume and airway diameter, allowing air to pass thru partially obst' mucus plugs or other foreign matter -Cont' of expiratory muscles against the closed glottis causes a high intrathoracic pressure to develop -When the glottis opens, large flow of air is expelled at a high speed, providing momentum for mucus to move to the upper airways to be expectorated or swallowed |
|
|
Diaphragmatic/ belly breathing |
Technique that encourages deep breathing to increase air to the lower lungs. -Belly moves out when inhaling and sinks when exhaling * Opens the pores of Kohn btw alveoli to allow sharing of Oxygen between alveoli -This is important if alveoli are plugged with mucus. |
|
|
Evaluating effectiveness of coughing by: |
-Sputum expectoration -Pt's report of swallowed sputum -Clearing of adventitious sounds by auscultation Encourage pt w/ chronic pulmonary diseases, URT infections, LRT infections to deep breathe and cough q2h while awake Pt w/ excessive sputum to cough q1h and wake to cough q2-3h during night PostOP directed cough q 2-4h while pt awake to prevent accumulation of secretions (use splint) |
|
|
Cascade cough |
Pt takes a slow, deep breath and holds it for 2 seconds while contracting expiratory muscles Then opens the mouth and performs a series of coughs throughout exhalation, coughs at progressively lowered lung volumes * Promotes airway clearance and a patent airway in pt's with large volume of sputum |
|
|
huff cough |
Simulates a natural cough reflex and is generally effective only for clearing central airways -While exhaling, pt opens glottis by saying the word huff (w/ practice pt able to progress to cascade cough) |
|
|
Quad cough |
For pt without abdominal muscle control (SCI) While pt breathes out with a maximal expiratory effort, the patient or nurse pushes inward and upward on the abdominal muscles toward the diaphragm, causing the cough |
|
|
Chest physiotherapy (CPT) |
-Group of therapies for mobilizing pulmonary secretions Postural drainage, chest percussion, vibration -Followed by productive coughing or suctioning of a pt who has decreased ability to cough --Recommended for pt who produces greater than 30 mL of sputum per day, atelectasis, pneumonia |
|
|
Contraindications for CPT |
-Diuretics, antihypertensives decrease pt's tolerance to postural changes and postural drainage -Long term use of steroid increases risk for rib fractures and contra to vibration -Increased ICP, SCI, abd aneurysm resection contra to positional changes of postural drainage -Thoracic trauma or surgery contra percussion + vibration -Congenital / acquired cog limitations alter pt ability to learn and follow controlled coughing techniques - Be aware of exercise tolerance since CPT is fatiguing |
|
|
Assessment before CPT |
- Respiratory assessment to confirm need for CPT ( sputum production, effectiveness of cough, hx of pulmonary probs successfully tx w/ CPT) -abnormal lung sounds, documented conditions such as atelectasis, pneumonia, changes in o2 status |
|
|
Postural drainage |
Use of positioning techniques that drain secretions from specific segments of the lungs and bronchi into the trachea
Purpose of various positions in postural drainage is to drain each segment toward the larger airways - Position maintained for about 5 minutes during p+v - Schedule procedure to be completed 1 hour before meals or 3 hours after meals |
|
|
Contraindications for positions for postural drainage (trendelenburg) |
chest trauma hemoptysis heart disease pulmonary embolus head injury Other conditions where pt's condition is not stable |
|
|
Percussion |
Rhythmically clapping on the chest wall over the area being drained to force secretions into larger airways for expectoration - Position hand w/ fingers and thumb touching and hands cupped (cupping makes hand conform to chest wall while trapping air cushion to soften intensity of clapping) - Procedure should sound hallow and not be painful -Perform over single layer of clothing |
|
|
Contraindications for percussion |
Bleeding disorders osteoporosis fractured ribs Avoid over burns, open wounds, infected skin of thorax - Caution to percuss lung fields under the ribs and NOT over spine, breastbone, stomach, lower back b/c trauma to spleen, liver, and kidneys |
|
|
Vibration |
Shakes secretions to larger airways --> Place flattened hand or 2 hands firmly on chest wall over the appropriate segment and tense muscles of the arm and provide a shaking motion. (have pt exhale slowly during vibration) - increases velocity and turbulence of exhaled air, helps remove secretions, increases exhalation of trapped air, shakes mucous loose, and induces a cough - Tolerated better than percussion and can be used in sitch where percussion is contraindicated |
|
|
Cuff inflation pressure |
16 - 20 mmHg or < 25 cm H20 Should not exceed to allow adequate tracheal capillary perfusion (add or remove air to the pilot tubing using a syringe and stopcock.) -Verify cuff pressure with manometer - High pressure predisposes to tracheal necrosis - Cuff can be deflated when pt no longer at risk for aspiration -Suction trach tube then mouth before deflating to prevent aspiration during deflation - Deflate during exhalation, inflate during inhalation |
|
|
Obturator |
-Used when inserting the tube - When inserting place obturator inside the outer cannula with rounded tip protruding from the end of the tube to ease insertion -TAKE OUT IMMEDIATELY so air can flow through the tube -Keep at bedside for use in case of accidental decantation |
|
|
Non disposable inner cannula ? |
Clean every 8 hours |
|
|
Suction catheter size |
- no more than half the size of the lumen of the tracheostomy tube |
|
|
Suction pressure set at |
-120 to -150 mmHg |
|
|
Preoxygenate for |
minimum of 30 seconds by: 1) adjusting ventilator to deliver 100% oxygen 2) using MRB connected to 100% oxygen 3) asking pt to take 5-6 deep breaths while administering oxygen |
|
|
Insert suction catheter |
WITHOUT SUCTION to minimize amount of O2 removed from lungs To point where pt coughs or resistance is met OR 0.5- 1.0 cm beyond length of artificial airway then, withdraw catheter 0.5 - 1.0 cm before applying suction to prevent trauma to carina |
|
|
Limit suction time to |
10 seconds |
|
|
D/C suctioning if : |
HR decreases from baseline by 20 beats/min HR increases from baseline by 40 beats/min A dysrhythmia occurs SpO2 decreases to less than 90% |
|
|
After each suction pass: |
Oxygenate for at least 30 seconds with 5-6 breaths by MRB |
|
|
Tracheostomy care provided |
every 8 hours |
|
|
Oropharyngeal and nasopharyngeal suctioning |
- Used when pt is able to cough effectively but unable to clear secretions by expectorating -Apply suction after pt has coughed -Once the pulmonary secretions decrease and a patient is less fatigued, he is then able to expectorate or swallow mucus, and suctioning no longer necessary |
|
|
orotracheal and nasotracheal suctioning |
Necessary when pt w/ pulmonary secretions is unable to manage secretions by coughing and doesn't have artificial airway -Pass sterile catheter the mouth or nose into the trachea (nose preferred to reduce gag reflex) -Advance catheter tip farther into the pt's trachea -Allow pt to rest bwt passes of the catheter |
|
|
Tracheal suctioning |
Performed thru an artificial airway such as an endotracheal or tracheotomy tube -Catheter size should be as small as possible, but large enough to remove secretions - Half the internal diameter of the ET tube is size recommendation -never apply suction pressure while inserting the catheter to avoid traumatizing the lung mucosa -Once insert catheter to necessary distance, maintain pressure bwt 120 and 150 mmHG as you withdraw Apply suction intermittently ONLY while withdrawing the catheter |
|
|
Open VS closed suctioning |
Open suctioning involves using a new sterile catheter for each suction session Closed suctioning involves using a reusable sterile suction catheter that is encased in a plastic sheet to protect it btw suction sessions (used most often on pt who require mechanical ventilation to support resp status b/c it permits continuous delivery of 02 while suction is performed & reduces risk of o2 desaturation Sterile gloves not required |
|
|
Oral airway |
-Prevents obstruction of the trachea by displacement of the tongue into the oropharynx -Extends from the teeth to the oropharynx, maintaining the tongue in the normal position Use correct size airway: measure the distance from the corner of the mouth to the angle of the jaw just below the ear to the distance from the flange of the airway to the tip (airway too small, tongue doesn't stay in place) (airway too large, forces tongue toward the epiglottis and obstructs the airway) -Insert airway by turning the cure of airway toward the cheek and placing it over the tongue -When airway is in oropharynx, turn it so the opening points downward Correct placement: airway moves the tongue forward away from the oropharynx, and the flange (flat portion of the airway) rests agains pt's teeth |
|
|
Endotracheal and tracheal airway |
ET is a short term artificial airway to admin mechanical ventilation, relieve upper airway obst, protect against aspiration, clear secretions -Tube is passed thru the pt's mouth passed the pharynx, and into the trachea -Usually removed w/n 14 days, can be used longer |
|
|
Tracheostomy |
Long term assistance artificial airway (incision made into trachea, a short artificial airway the tracheostomy tube is inserted) MC complication is partial or total airway obstruction caused by buildup of respiratory secretions -Humidification from air humidifiers or humidified oxygen tracheostomy collars can help prevent drying secretions that cause occlusion |
|
|
Nursing interventions to maintain or promote lung expansion |
Noninvasive: ambulation, positioning, incentive spirometry, noninvasive ventilation Invasive: chest tube insertion and management assist in restoring lung expansion |
|
|
Noninvasive positive pressure ventilation |
-Used to prevent using invasive artificial airways in pt w/ acute respiratory failure, cariogenic pulmonary edema, or exacerbation of COPD, after ET tube extubation -Purpose: maintain positive airway pressure and improve alveolar ventilation -Prevents/ treats atelectasis by inflating the alveoli, reducing pulmonary edema by forcing fluid out of lungs back into circulation TypesL CPAP, BiPAP (bilevel) |
|
|
Chest tubes |
-A catheter inserted thru the thorax to remove air and fluids from the pleural space or to reestablish normal intrapleural and intrapulmonic pressures Common after chest surgery and chest trauma and used for tx of hemothorax, pneumothorax to promote lung reexpansion |
|
|
Chest tube sizes |
small bore chest tube (12-20 Fr) used to remove a small amount of air Large bore chest tube to remove large amounts of fluid or blood and large amounts of air |
|
|
S/S of upper and lower airway obstruction (requiring suctioning) |
- abnormal RR -adventitious sounds on inspiration + expiration -nasal secretions -Gurgling -drooling -restlessness -gastric secretions/ vomit in mouth -Coughing without clearing secretions from airway |
|
|
s/s associated w/ hypoxia and hypercapnia |
-Decreased Sp02 -Increased pulse and BP -Increased RR -apprehension -anxiety -decreased ability to concentrate -lethargy -Decreased LOC -fatigue, dizziness, irritability -dysrhythmias, pallor, cyanosis |
|
|
RF for upper or lower airway obstruction |
COPD Pulmonary infection Fluid imbalance Lack of humidity Impaired mobility Decreased LOC Decreased gag or cough reflex Dysphagia Presence of feeding tube |
|
|
Contraindications to nasotracheal suctioning |
occluded nasal passages nasal bleeding epiglottitis croup acute head, facial, neck injury Coagulopathy or bleeding disorder Irritable airway laryngospasm / bronchospasm gastric surgery w/ high anastomosis MI |
|
|
Tracheostomy tube with an inflated cuff |
-Used if pt is at risk for aspiration or needs mechanical ventilation -Cuff exerts pressure on tracheal mucosa -Cuff inflation pressure should not exceed 20 mmHg or 25 cm H2o (higher pressures may compress tracheal capillaries, limit blood flow, predispose pt to tracheal necrosis -MLT (minimal leak technique) and MOV (minimal occlusion volume) methods used to inflate cuff |
|
|
Deflating cuff |
-Done when pt no loner risk for aspiration -Before deflation, have pt cough up secretions and suction the tracheostomy tube then the mouth (prevents aspiration of secretions) -Deflated during exhalation to help propel secretions to mouth - Deflating cuff asap reduces swallowing dysfunction that the cuff causes |
|
|
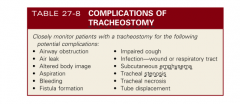
Complications of tracheostomy |
|
|
|
Fenestrated tube |
- Has openings on the surface of the outer cannula that permit air from the lungs to flow over the vocal cords -Allows pt to breath spontaneously thru larynx, speak, cough up secretions while tracheostomy tube remains in place -Only pt who can swallow without risk of aspiration can use this tube -Also used when pt needs to be mechanically ventilated |
|
|
If there is no aspiration |
1) remove inner cannula (if nonfenenstrated) 2) deflated the cuff 3) place the decantation cap in the tube Severe respiratory distress may result if tube is capped before removing the inner cannula and deflating the cuff |
|
|
Disadvantage of fenestrated tube |
Potential for developing tracheal polyps from tracheal tissue granulating into the fenestrated openings |
|
|
Speaking tracheostomy tube |
- Has 2 pigtail tubings (one connects to the cuff and is for cuff inflation, second connects to an opening just above the cuff) -When the second tubing is connected to a low flow (4-6 L/minute) air source allows air to move up over vocal cords and permit speech -Allows pt w at risk for aspiration to speak w/ cuff inflated |
|
|
Decannulation |
- Tracheostomy tube can be removed when the patient can adequately exchange air and expectorate secretions - Close stoma with tape strips and cover it with occlusive dressing - Epithelial tissue begins to form in 24 - 48 hrs - Opening closes within 4 -5 days - Splint stoma when coughing, swallowing, speak -SURGICAL INTERVENTION NOT REQUIRED |
|
|
Pneumothorax |
Air in pleural space -Dyspnea, decreased mvmc of chest wall, diminished or absent breath sounds on affected side, hyperresonance to percussion Intervention: chest tube insertion with flutter valve or chest drainage system |
|
|
Hemothorax |
Blood in the pleural space, may/may nit occur in conjunction with pneumothorax - Dyspnea, diminished or absent breath sounds, dullness to percussion, decreased hgb, shock depending on blood volume lost Intervention: chest tube insertion w/ chest drainage system. Autotransfusion of collected blood, tx of hypovolemia as necessary |
|
|
Tension pneumothorax |
Air in pleural space that doesn't escape. Increased air in pleural space shifts organs and increases intrathoracic pressure - Cyanosis, air hunger, violent agitation, tracheal dev away from affected side, subcutaneous emphysema, neck vein distention, hyperresonance to percussion Intervention: needle decompression followed by chest tube insertion w/ chest drainage system |
|
|
Flail chest |
Fracture of two or more adjacent ribs in two or more places with loss of chest wall stability - paradoxic mvmt of chest wall, respiratory distress. May be associated with hemothorax, pneumothorax, pulmonary contusion Intervention: O2 as needed to maintain o2 sat, analgesia, CPAP, BiPAP (positive pressure ventilation), mechanical ventilation |
|
|
Cardiac tamponade |
Blood rapidly collects in pericardial sac, compresses myocardium because the pericardium doesn't stretch and prevents ventricles from filling - Muffled, distant heart sounds, hypotension, neck vein distention, increased central venous pressure Intervention: Surgery, medical emergency, pericardiocentesis |
|
|
Spontaneous pneumothorax |
Occurs due to the rupture of small blebs on apex of lungs
Primary: bleb occurs in healthy young individual Secondary: as result of lung disease (COPD, asthma, CF, pneumonia) - Smoking increases risk for bleb formation - RF: being tall and thin, male gender, family hx, previous spontaneous pneumothorax |
|
|
Iatrogenic pneumothorax |
Due to laceration or puncture of lung during medical procedures -Transthoracic needle aspiration is leading cause Others: subclavian catheter insertion, thoracentisis, pleural biopsy, transbronchial lung biopsy -Barotrauma from excessive ventilatory pressure during manual or mechanical ventilation |
|
|
Traumatic pneumothorax |
Can occur from penetrating (open) or non penetrating (closed) chest trauma -Penetrating trauma allows air to enter pleural space thru an opening in chest wall Ex: stab or gunshot wounds, surgical thoracotomy Emergency tx is covering wound with an occlusive dressing secured on three sides (vent dressing) |
|
|
Tension pneumothorax |
Air enters pleural space but cannot escape - Accumulation of air in pleural space causes increased intrapleural pressures = compression of lung on affected side and pressure of the heart and great vessels, pushing them away from affected side Mediastinum shift towards unaffected side (compressing good lung), which further compromises oxygenation As pressure increases, venous return is decreased and CO falls --> Results from open or closed pneumothorax, mechanical ventilation, resuscitative efforts, chest tubes are clamped or become blocked |
|
|
Tension pneumothorax manifestations |
Dyspnea, tachycardia, tracheal deviation, decreaed or absent breath sounds on affected side, neck vein distension, cyanosis, diaphoresis MEDICAL EMERGENCY: if tension in pleural space isn't relieved, pt likely to die from inadequate CO or severe hypoxemia |
|
|
Hemothorax |
Accumulation of blood in pleural space resulting from injury to chest wall, diaphragm, lung, blood vessels, or mediastinum. - Occurs w/ pneumothorax is called a hemopneumothorax - Pt requires immediate insertion of a chest tube for evacuation of the blood, which can ne recovered and reinserted for a short time after injury |
|
|
Chylothorax |
- Lymph fluid in pleural space - Thoracic duct is disrupted traumatically or from a malignancy - Normal lymph flow thru thoracic duct is 1500- 2500 mL/day. This amount can increase up to tenfold after ingestion of fats - 50% of cases heal w/ conservative tx ( chest drainage, bowel rest, parenteral nutrition) - Octreotide used to reduce the flow of lymph fluid - Pleurodesis is artificial production of adhesions between the parietal and visceral pleura, usually done with chem sclerosing agent (talc or doxycycline) |
|
|
Fractured Ribs |
Most common type of chest injury resulting from blunt trauma - Ribs 5-9 most frequently fractured because they are least protected by chest muscles -Fractured rib is splintered or displaced, it may damage the pleura and lungs -> pain at site of injury during inspiration and coughing, patient splints area and takes shallow breaths to decrease the pain - Ateletasis and pneumonia develop because of decreased ventilation and retained secretions - NSAID, opioids, nerve blocks, deep breathing, coughing, incentive spirometry |
|
|
Flail chest |
- Fracture of several consecutive ribs, in 2 or more separate places, causing an unstable segment. - Instability of chest wall causes paradoxic mvmt during breathing - Paradoxic chest mvmt prevents adequate ventilation aof lung in the injured area and increases the work of breathing |
|
|
Flail chest manifestations |
- rapid, shallow respirations and tachycardia Diagnosed by ABGs, chest xray, palpitation of abnormal respiratory mvmt, evaluation for crepitus near rib fractures |
|
|
flutter of heimlich valve |
Used to evacuate air from the pleural space. (prevents reentry of air into pleural space) -Consists of a one way rubber valve within a rigid plastic tube. It's attached to the external end of chest tube - Valve opens when pressure in chest is greater than atmospheric pressure (during expiration) and closes when intrathoracic pressure is less than atmospheric pressure (during inspiration) -Used in place of a chest drainage unit for small uncomplicated pneumothorax w/ little or no drainage and no need for suction |
|
|
Oropharyngeal (oral) airways (OPAs) |
Inserted into the mouth and used only on unconscious, unresponsive victims with no gag reflex
Contra: victim suffered oral trauma, such as broken teeth, recently undergone oral surgery |
|
|
Nasopharyngea (nasal) airways |
Inserted into the nose and may be used on a conscious, responsive victim or an unconscious victim -Doesn't cause gag reflex Contra: victims w/ suspected head trauma or skull fracture |
|
|
Inserting OPA |
1) measure OPA from earlobe to corner of the mouth 2) Use cross finger technique to open the victim's mouth 3) Grasp lower jaw and tongue and lift upward 4) Insert OPA w/ curved end along roof of mouth 5) as tip approaches back of mouth, rotate it 180 degrees 6) slide OPA into back of throat --> Flange should rest on victim's lips |
|
|
Inserting NPA |
1) Measure from earlobe to tip of nostril. Ensure diameter of NPA is not larger than nostril 2) Use water soluble lubricant on NPA prior to insertion 3) With bevel toward septum (center of the nose), advance NPA gently, straight in, following the floor of the nose 4) Flange should rest on victim's nostril |
|
|
Take care not to dislodge tracheostomy during first 5-7 days when stoma is not mature Precautions to prevent early tube replacement |
- Keep a replacement tube both smaller or bigger and equal size at bedside -Do not change tracheostomy tapes for at least 24 hours after insertion procedure - Physician performs first tube change no sooner than 7 days after tracheostomy |
|
|
What do you do in an accidental tube dislodgment? |
- Immediately attempt to replace it - Grab retention sutures or use a hemostat to spread the opening to facilitate replacing tube -Insert obturator in the replacement tube (lube with saline poured over tip) -Insert tube into stoma at a 45 degree angle to the neck (remove obturator) |
|
|
what do you do if the tube cannot be replaced? |
-Assess level of respiratory distress -Cover stoma with a sterile dressing and ventilate pt with bag mask ventilation over the nose and mouth until help arrives |
|
|
Flutter / heimich valve |
Used to evacuate air from the pleural space - Consists of a one way rubber valve within a rigid plastic tube attached to external end of CT - Valve opens when pressure in chest is greater than atmospheric pressure (during expiration) and closes when intrathoracic pressure is less than atmospheric pressure (inhalation) -Used for small to moderate sized pneumothorax, blebs |
|
|
Collection chamber |
Receives fluid (drainage) and air from the pleural or mediastinal space. The drained fluid stays in this chamber while the air vents to the water seal chamber |
|
|
Water seal chamber |
contains 2 cm of water, which acts as a one way valve. -Incoming air enters from the collection chamber and bubbles up through the water -Water prevents back flow of air into the patient from the system -Intermittent bubbling as long as their is air in pleural space -Normal fluctuation (tidaling) movement of water with respiration reflects intrapleural pressure changes during inspiration and expiration -Sudden cessation of tidaling = occluded tube |
|
|
Suction control chamber |
Applies suction to the chest drainage system (wet and dry suction control) - Water: uses column of water with top end vented to the atmosphere to control the amount of suction from the wall regulator -The amount of suction is regulated by the amount of water in the chamber -Filled with 20 cm of water - Suction pressure usually -20 cm H20 -Should see gentle bubbling |
|
|
If a chest tube becomes disconnected |
- Immediately reestablish the water seal system and attach a new drainage system asap -immerse in sterile water (2 cm) until system can be reestablished |
|
|
Appearance of a new air leak |
-Assess drainage system to id where leak is coming from (patient or system) - Chest tube may be momentarily clamped to change drainage apparatus or check for air leaks |
|
|
Complications associated w/ chest tube placement and drainage |
-Volumes of 1 - 1.5 L of pleural fluid are removed rapidly, reexpansion pulmonary edema or a vasovagal response with symptomatic hypotension may occur - SubQ emphysema can occur from air leaking into the tissue surrounding the chest tube insertion site -Severe subQ emphysema can cause drastic swelling of the head and neck with potential airway compromise |
|
|
Minimal occluding volume technique |
1) for the mechanically ventilated pt, place stethescope over trachea and inflate the cuff to MOV by adding air until no air leak is heard at peal inspiratory pressure (end of ventilator inspiration) 2) Spontaneously breathing: inflate until no sound is heard after a deep breath or after inhalation w/ a BVM 3) use a manometer to verify cuff pressure is between 20 -25 cm H20 (if cuff pressure cannot be maintained or larger volumes of air are needed to keep it inflated, could be a leak or tracheal dilation at the cuff site) Notify MD to reposition or change ET tube |
|
|
Minimal leak technique |
Procedure is same as MOV - Remove a small amount of air from he cuff winter a slight air leak is auscultated at peak inflation |