![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
197 Cards in this Set
- Front
- Back
|
When should you not delegate vital signs? |
orthostatic hypotension When evaluating a medication On admission |
|
|
What is body temperature? |
Heat produced - heat lost |
|
|
What is the acceptable temperature range? |
96.8 - 100.4 F 36 - 38 C |
|
|
Temperature sites |
Oral, rectal, axillary, temporal artery, tympanic membrane, esophageal catheter, pulmonary artery, urinary bladder |
|
|
What is the average core temperature ranges for the elderly population? |
35 - 36.1 C 95 - 97 F |
|
|
What time of day is the temperature the lowest? |
6 AM |
|
|
What time of day is the temperature the highest in healthy people? |
4 PM |
|
|
What is a core temperature? |
A temperature of the deep tissues humans keep body core temperature relatively constant despite environmental conditions and physical activity |
|
|
Surface temperatures |
Unlike core temperature, surface temperatures vary depending on blood flow to the skin and the amount of heat lost to the external environment. |
|
|
Differences in degrees between oral, rectal, and axillary temperatures |
Rectal one degree higher than oral Axillary one degree lower than oral |
|
|
Advantages of taking oral temperature |
Accurate surface temperature reading Reflects rapid change in core temp Reliable route to measure temperature in patients who are intubated |
|
|
Disadvantages of taking oral temp |
Causes delay in measurement if patient recently ingested hot/cold fluids or foods, smoked, or is receiving oxygen by mask/cannula Not for patients who had oral surgery, trauma, history of epilepsy, seizures, or confused, uncooperative, unconscious |
|
|
Advantages of taking tympanic membrane temp |
most accurate method in critically ill Used for patients with tachypnea without affecting breathing Sensitive to core temp changes Not influenced by environment |
|
|
Disadvantages of tympanic membrane temp |
Otitis media and cerumen impaction distorts reading surgery of the ear Does not accurately measure core temp changes during and after exercise Affected by ambient temp devices such as incubators, radiant warmers, and facial fans
|
|
|
Disadvantages or rectal temp |
Lags behind core temp during rapid temp changes Not for patients with diarrhea, rectal disorders, or bleeding tendencies or those who had rectal surgery Readings influenced by impacted stool |
|
|
Advantages of Temporal artery temp |
Reflects rapid change in core temp |
|
|
What two things regulate the balance between heat lost and heat produced, or thermoregulation? |
Physiological and behavioral mechanisms |
|
|
The hypothalamus |
senses minor changes in body temp. Anterior hypothalamus controls heat loss Posterior controls heat production |
|
|
Where is the hypothalamus located? |
Between the cerebral hemispheres |
|
|
How does the anterior hypothalamus control heat loss? |
When nerve cells in the anterior hypothalamus become heated beyond the set point, impulses are sent out to reduce body temp. The body redistributes blood to surface vessels to promote heat loss Mechanisms of heat loss: sweating, vasodilation (widening) of blood vessels, and inhibition of heat production |
|
|
How does the posterior hypothalamus control body temp? |
If posterior hypothalamus senses body temp is lower than set point the body initiates heat-conservation mechanisms. Mechanisms of heat conservation: vasoconstriction of blood vessels, voluntary muscle contraction, muscle shivering. |
|
|
How does heat production plays a role in body temperature regulation? |
Heat produced by the body is a by-product of metabolism. Activities requiring additional chemical reactions increase the metabolic rate. metabolism increases, additional heat is produced. metabolism decreases, less heat is produced. |
|
|
When does heat production occur? |
during rest, voluntary movements, involuntary shivering, and nonshivering thermogenesis |
|
|
Basal metabolic rate |
Basal metabolism accounts for the heat produced by the body at absolute rest |
|
|
Shivering |
The skeletal muscle movement during shivering requires significant energy The heat produced helps equalize body temp and the shivering ceases In vulnerable patients shivering seriously drains energy sources, resulting in further physiological deterioration |
|
|
Heat loss and heat production occur ___________. |
Simultaneously |
|
|
Heat loss |
The structure of the skin and exposure to the environment result in constant, normal heat loss through radiation, conduction, convection, and evaporation. |
|
|
Heat loss through radiation |
The transfer of heat from the surface of one object to the surface of another without direct contact between the two. Position enhances radiation heat loss (standing exposes a greater radiating surface area, and lying in a fetal position minimizes heat radiation) Promote heat loss thru radiation by removing clothing or blankets Or to decrease heat loss from radiation cover the body with dark, closely woven clothing |
|
|
Heat loss through conduction |
The transfer of heat from one object to another thru direct contact When warm skin touches a cooler object, heat is lost Applying an ice pack or bathing a patient with a cool cloth increases conductive heat loss Applying several layers of clothing reduces conductive loss heat loss t |
|
|
Intermittent fever |
Fever spikes interspersed with usual temperature levels (temperature returns to acceptable value at least once in 24h) |
|
|
Remittent fever |
Fever spikes and falls without a return to acceptable temperature levels |
|
|
Relapsing fever |
Periods of febrile episodes and periods with acceptable temperature values (febrile episodes and periods of normothermia are often longer than 24h) |
|
|
Pyrexia |
A fever. Elevated body temperature due to a change in the hypothetical set point |
|
|
What temperature is generally considered a fever of an adult or child? |
100.4 F or 38 C depending on the type of thermometer used |
|
|
Normothermia |
Normal body temperature between 36.5 and 37.2 C |
|
|
What temperature is considered Hypothermia ? |
Below 36.2 C |
|
|
What temperature is considered hyperthermia? |
Above 37.6 C |
|
|
What temperature is considered hyperpyrexia? |
Extremely high temp above 41.5 C |
|
|
Hypoxia |
Inadequate oxygen |
|
|
Heat loss thru convection |
The transfer of heat away by air movement. A fan promotes heat loss thru convection The rate of heat loss increases when moistened skin comes into contact with slightly moving air. |
|
|
Fever of unknown origin (FUO) |
A fever with an undetermined cause |
|
|
What is hyperthermia? |
An elevated body temperature related to the inability of the body to promote heat loss or reduce heat production. |
|
|
What causes hyperthermia? |
An overload of the thermoregulatory mechanisms. Any disease or trauma to the hypothalamus impairs heat-loss mechanisms. |
|
|
What is malignant hyperthermia? |
Hereditary condition of uncontrolled heat production that occurs when susceptible people receive certain anesthetic drugs. |
|
|
What is heatstroke? |
A body temperature of 40 C (104 F) or more accompanied by hot, dry skin and CNS abnormalities, such as delirium, convulsions, or coma. *dangerous heat emergency with a high mortality rate* |
|
|
Signs and symptoms of a heat stroke |
Giddiness, confusion, delirium, excessive thirst, nausea, muscle cramps, visual disturbances, incontinence, increased HR, low BP. Most important sign is hot, dry skin. There will be no sweat bc of severe electrolyte loss and hypothalamic malfunction. If progresses patient becomes unconscious, with fixed, non reactive pupils. Permanent neurological damage can occur unless cooling measures are rapidly started. |
|
|
What are the two types of heatstroke? |
Exertional and nonexertional |
|
|
Exertional heatstroke |
Develops in able-bodied individuals, such as athletes, shoulders, or laborers who are performing rigorous physical activities |
|
|
Nonexertional heatstroke |
Can develop during low-level physical activities among elderly, ambulatory individuals with comorbidities (diabetes, CV disease) |
|
|
Besides exertional and nonexertional heatstroke patients who else is at risk for developing heatstroke? |
Those who take medications that decrease the ability of the body to lose heat Anticholinergics Amphetamines Beta-adrenergic receptor antagonists Phenothiazides
Diuretics |
|
|
Heat loss thru evaporation |
The transfer of heat energy when a liquid is changed to a gas. The body continuously losses heat by evaporation. Approx. 600 to 900 mL a day evaporated from the skin and lungs, resulting in water and heat loss. |
|
|
Heat exhaustion |
Occurs when profuse diaphoresis results in excess water and electrolyte loss. Caused by environmental heat exposure, a patient exhibits s/s of deficient fluid volume |
|
|
What is Hypothermia? |
Heat loss during prolonged exposure to cold overwhelms the ability of the body to produce heat. Assessment of core temperature is critical when you suspect hypothermia. A special low reading thermometer is required because standard devices do not register below 35 C (95 F) |
|
|
S/S of hypothermia |
Uncontrolled shivering, loss of memory, depression, poor judgement, HR, RR, BP fall as temp falls, skin becomes cyanotic, cardiac dysrhythmias, loss of LOC, unresponsive to painful stimuli In severe cases a person demonstrates clinical signs similar to death (lack of response to stimuli, extremely low RR and pulse) |
|
|
Frostbite |
Ice crystals form inside the cells, and permanent circulatory and tissue damage occurs. Most susceptible earlobes, tip of nose, fingers, toes The injured area becomes white, waxy, and firm to the touch. The patient looses sensation in the area. Interventions: gradual warming, analgesia, protection of the injured tissue |
|
|
Interventions for patient with a fever |
Obtain cultures of body fluids before being antibiotic if ordered Minimize heat production (reduce frequency of activities) Maximize heat loss (reduce external coverings w/o causing shivering) Satisfy requirements for increased metabolic rate (supplemental oxygen as ordered, provide measures to stimulate appetite & provide 8-10 8oz glasses fluids) Encourage oral hygiene from dehydration, damp cloth to forehead Identify onset and duration of febrile episodes Control environmental temp to 21 C to 27 C (70 F to 80 F) |
|
|
Interventions for hyperthermia |
Remove excess clothing and blankets Provide external cool packs or cooling blanket (better option) Hydrate with cool liquids (oral or IV) Lavage with cool fluids Administer antipyretic drug therapy |
|
|
Interventions for hypothermia |
Remove the person from the cold Provide external warming measures Provide internal warning measures *core rewarming must be done slowly to minimize the risk for dysrhythmias. Cardiac monitoring is required when the patient is recovering from severe hypothermia)* |
|
|
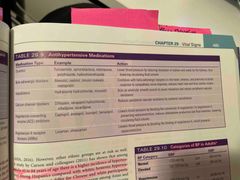
Antipyretics |
Medications to reduce fever Acetaminophen & NSAIDS such as ibuprofen, salicylates, and indomethacin reduce fever by increasing heat loss. |
|
|
How do Corticosteroids effect body temperature and infection? |
Although not used to treat fever, they reduce heat production by interfering with the hypothalamic response. Steroids mask S/S of infection so patients prescribed steroids need to be monitored closely, especially if they’re at risk for infection. |
|
|
Nonpharmacological therapies for reducing fever |
Blankets cooled by circulating water delivered by motorized units increase conductive heat loss. Make sure that nursing measures to enhance body cooling do not stimulate shivering. Shivering is counterproductive & increases energy expenditure up to 400%. Avoid tepid baths, Bathing w alcohol-water solutions, Applying ice packs to groin and axillae areas, And cooling fans Medications to reduce shivering are meperidine and butorphanol |
|
|
Diaphoresis |
Visible perspiration primarily occurring on the forehead and upper thorax. For each hour of exercise in hot conditions up to 2 L of body fluid can be lost in sweat. Excessive evaporation causes skin scaling and itching and drying of the nares and pharynx. |
|
|
Interventions for patient with a fever |
Obtain cultures of body fluids before being antibiotic if ordered Minimize heat production (reduce frequency of activities) Maximize heat loss (reduce external coverings w/o causing shivering) Satisfy requirements for increased metabolic rate (supplemental oxygen as ordered, provide measures to stimulate appetite & provide 8-10 8oz glasses fluids) Encourage oral hygiene from dehydration, damp cloth to forehead Identify onset and duration of febrile episodes Control environmental temp to 21 C to 27 C (70 F to 80 F) |
|
|
What is THE indicator of circulatory response? |
Pulse |
|
|
What regulates the strength of ventricular contraction and the stroke volume? |
Mechanical, neural, and chemical factors |
|
|
The volume of blood pumped by the heart in one minute is the ___________________. |
Cardiac output, the product of HR, and the ventricular stroke volume. |
|
|
In an adult the heart normally pumps ______ of blood per minute. |
5000 mL |
|
|
Ulnar pulse |
Used to perform an Allen’s test |
|
|
Character of the pulse include: |
Rate, rhythm, strength, equality When auscultating apical assess rate and rhythm only |
|
|
If you detect an abnormal rate while palpating a peripheral pulse, the next step is to _____________. |
Assess the apical rate |
|
|
Pulse deficit |
An inefficient contraction of the heart that fails to transmit a pulse wave to the peripheral pulse site. To assess: assess radial and apical rates simultaneously and then compare rates. The difference between the apical and radial pulse rates is the pulse deficit. |
|
|
Pulse rhythm |
Is either regular or irregular |
|
|
People who have a congenital absence of sweat glands or a serious skin disease that impairs sweating are ___________. |
Unable to tolerate warm temps because they cannot cool themselves adequately. |
|
|
Dysrhythmia |
An interval interrupted by an early or late beat or a missed beat indicates an abnormal rhythm. Described as regularly irregular or irregularly irregular |
|
|
Strength of the pulse |
Reflects the volume of blood ejected against the arterial wall with each heart contraction and the condition of the arterial vascular system leading to the pulse site Bounding (4) Full or strong (3) Normal and expected (2) Diminished or barely palpable (1) Absent (0) |
|
|
Pulse equality |
Assess pulses on both sides comparing the two. A pulse in one extremity is sometimes unequal in strength or absent in many disease states (ex. thrombus formation) |
|
|
Factors influencing HR INCREASING pulse rate |
Exercise (short term exercise) Temperature (fever and heat) Acute pain Emotions (anxiety) Medications (positive chronotropic drugs such as epinephrine) Hemorrhage (sympathetic stimulation increased by loss of blood) Postural changes (standing or sitting) Pulmonary conditions (asthma, COPD) |
|
|
Factors influencing HR DECREASING pulse rate |
Heart conditioned by long term exercise Hypothermia Chronic pain Negative chronotropic drugs such as digitalis, beta adrenergic and calcium blockers Lying down |
|
|
Nursing diagnoses for pulse |
Activity intolerance Anxiety Acute pain Decreased cardiac output Deficient/excess fluid volume Impaired gas exchange Ineffective peripheral tissue perfusion |
|
|
Respiration |
The mechanism the body uses to exchange gases between the atmosphere and the blood and the blood and the cells. It involves ventilation, diffusion, and perfusion. |
|
|
Ventilation |
The movement of gases in and out of the lungs |
|
|
Diffusion |
The movement of oxygen and carbon dioxide between the alveoli and the red blood cells |
|
|
Perfusion |
The distribution of red blood cells to and from the pulmonary capillaries |
|
|
Skin in temperature regulation |
The skin regulates temp thru insulation of the body, vasoconstriction, and temperature sensation. The skin, subcutaneous tissue, and fat keep heat inside the body. People with more fat have more natural insulation than do slim or muscular people. |
|
|
Analyzing respiratory efficiency requires: |
Assessing ventilation by determining respiratory rate, depth, rhythm, and end-tidal carbon dioxide (EtCO2) value. And assessing diffusion and perfusion by determining oxygen saturation (SpO2) |
|
|
Hypoxemia |
Low levels of arterial O2 |
|
|
During a normal, relaxed breath, a person inhales ______ of air. |
500 mL (the tidal volume) |
|
|
Eupnea |
Normal respiration |
|
|
Respiratory depth |
Described as deep, normal, or shallow |
|
|
Respiratory rhythm |
Regular or irregular |
|
|
Alterations in breathing patterns |
Back (Definition) |
|
|
Factors influencing respirations |
Back (Definition) |
|
|
Factors affecting oxygen saturation |
Back (Definition) |
|
|
Blood pressure |
The force exerted on the walls of an artery by the pulsing blood under pressure from the heart. |
|
|
Alterations in breathing patterns |

Back (Definition) |
|
|
Factors influencing respirations |

Back (Definition) |
|
|
Factors affecting oxygen saturation |

Back (Definition) |
|
|
Pulse pressure |
The difference between systolic and diastolic pressure |
|
|
Blood pressure reflects the interrelationships of: |
Cardiac output Peripheral resistance Blood volume Viscosity Vessel elasticity |
|
|
Factors affecting body temp |
Age(temp reg unstable till puberty, usual temp range drops as individuals approach older adulthood) Exercise (any form increases metabolism & heat production and thus body temp) Hormone level (hormonal variations during the menstrual cycle cause body temp fluctuations, menopause) Circadian rhythm (normally changes 0.5-1 C during 24h period, usually lowest 1-4 AM & highest at 4 PM. Does not change with age but does with Occupation) Stress (physical and emotional stress increase body temp) Environment (affect infants and older adults more often bc their temperature-regulating mechanisms are less efficient) Temperature alterations (fever, hyperthermia, heatstroke, heat exhaustion, hypothermia) |
|
|
Patterns of fever |
Sustained Intermittent Remittent Relapsing |
|
|
Sustained fever |
A constant body temperature continuously above 38 C (100.4 F) that has little fluctuation |
|
|
Heat loss through conduction |
The transfer of heat from one object to another thru direct contact When warm skin touches a cooler object, heat is lost Applying an ice pack or bathing a patient with a cool cloth increases conductive heat loss Applying several layers of clothing reduces conductive loss heat loss |
|
|
Intermittent fever |
Fever spikes interspersed with usual temperature levels (temperature returns to acceptable value at least once in 24h) |
|
|
Remittent fever |
Fever spikes and falls without a return to acceptable temperature levels |
|
|
Relapsing fever |
Periods of febrile episodes and periods with acceptable temperature values (febrile episodes and periods of normothermia are often longer than 24h) |
|
|
Pyrexia |
A fever. Elevated body temperature due to a change in the hypothetical set point |
|
|
The skins role in temperature regulation |
insulating the body, vasoconstriction, and temperature sensation. |
|
|
Normothermia |
Normal body temperature between 36.5 and 37.2 C |
|
|
What temperature is considered Hypothermia ? |
Below 36.2 C |
|
|
What temperature is considered hyperthermia? |
Above 37.6 C |
|
|
What temperature is considered hyperpyrexia? |
Extremely high temp above 41.5 C |
|
|
Hypoxia |
Inadequate oxygen |
|
|
Heat loss thru convection |
The transfer of heat away by air movement. A fan promotes heat loss thru convection The rate of heat loss increases when moistened skin comes into contact with slightly moving air. |
|
|
Fever of unknown origin (FUO) |
A fever with an undetermined cause |
|
|
What is hyperthermia? |
An elevated body temperature related to the inability of the body to promote heat loss or reduce heat production. |
|
|
What causes hyperthermia? |
An overload of the thermoregulatory mechanisms. Any disease or trauma to the hypothalamus impairs heat-loss mechanisms. |
|
|
What is malignant hyperthermia? |
Hereditary condition of uncontrolled heat production that occurs when susceptible people receive certain anesthetic drugs. |
|
|
What is heatstroke? |
A body temperature of 40 C (104 F) or more accompanied by hot, dry skin and CNS abnormalities, such as delirium, convulsions, or coma. *dangerous heat emergency with a high mortality rate* |
|
|
Signs and symptoms of a heat stroke |
Giddiness, confusion, delirium, excessive thirst, nausea, muscle cramps, visual disturbances, incontinence, increased HR, low BP. Most important sign is hot, dry skin. There will be no sweat bc of severe electrolyte loss and hypothalamic malfunction. If progresses patient becomes unconscious, with fixed, non reactive pupils. Permanent neurological damage can occur unless cooling measures are rapidly started. |
|
|
What are the two types of heatstroke? |
Exertional and nonexertional |
|
|
Exertional heatstroke |
Develops in able-bodied individuals, such as athletes, shoulders, or laborers who are performing rigorous physical activities |
|
|
Nonexertional heatstroke |
Can develop during low-level physical activities among elderly, ambulatory individuals with comorbidities (diabetes, CV disease) |
|
|
Besides exertional and nonexertional heatstroke patients who else is at risk for developing heatstroke? |
Those who take medications that decrease the ability of the body to lose heat Anticholinergics Amphetamines Beta-adrenergic receptor antagonists Phenothiazides
Diuretics |
|
|
Heat loss thru evaporation |
The transfer of heat energy when a liquid is changed to a gas. The body continuously losses heat by evaporation. Approx. 600 to 900 mL a day evaporated from the skin and lungs, resulting in water and heat loss. |
|
|
Heat exhaustion |
Occurs when profuse diaphoresis results in excess water and electrolyte loss. Caused by environmental heat exposure, a patient exhibits s/s of deficient fluid volume |
|
|
What is heatstroke? |
body temperature of 40 C (104 F) , hot, dry skin, delirium, convulsions, or coma. *dangerous heat emergency with a high mortality rate* |
|
|
Signs and symptoms of a heat stroke |
delirium, excessive thirst, visual disturbances, increased HR, low BP. Most important sign is hot, dry skin. There will be no sweat bc of severe electrolyte loss and hypothalamic malfunction. If progresses patient becomes unconscious, with fixed, non reactive pupils. Permanent neurological damage can occur unless cooling measures are rapidly started. |
|
|
Frostbite |
Ice crystals form inside the cells, and permanent circulatory and tissue damage occurs. Most susceptible earlobes, tip of nose, fingers, toes The injured area becomes white, waxy, and firm to the touch. The patient looses sensation in the area. Interventions: gradual warming, analgesia, protection of the injured tissue |
|
|
Exertional heatstroke |
athletes, soldiers, or laborers who are performing rigorous physical activities |
|
|
Interventions for hyperthermia |
Remove excess clothing and blankets Provide external cool packs or cooling blanket (better option) Hydrate with cool liquids (oral or IV) Lavage with cool fluids Administer antipyretic drug therapy |
|
|
Besides exertional and nonexertional heatstroke patients who else is at risk for developing heatstroke? |
Those who take medications that decrease the ability of the body to lose heat Anticholinergics Amphetamines Beta-adrenergic receptor antagonists Phenothiazides Diuretics |
|
|
Antipyretics |
Medications to reduce fever Acetaminophen & NSAIDS such as ibuprofen, salicylates, and indomethacin reduce fever by increasing heat loss. |
|
|
How do Corticosteroids effect body temperature and infection? |
Although not used to treat fever, they reduce heat production by interfering with the hypothalamic response. Steroids mask S/S of infection so patients prescribed steroids need to be monitored closely, especially if they’re at risk for infection. |
|
|
S/S of hypothermia |
Uncontrolled shivering, HR, RR, BP fall as temp falls, cyanotic, cardiac dysrhythmias, loss of LOC In severe cases a person demonstrates clinical signs similar to death (lack of response to stimuli, extremely low RR and pulse) |
|
|
Diaphoresis |
Visible perspiration primarily occurring on the forehead and upper thorax. For each hour of exercise in hot conditions up to 2 L of body fluid can be lost in sweat. Excessive evaporation causes skin scaling and itching and drying of the nares and pharynx. |
|
|
Interventions for patient with a fever |
Obtain cultures of body fluids before starting antibiotic if ordered Minimize heat production (reduce frequency of activities) Maximize heat loss (reduce external coverings w/o causing shivering) Satisfy requirements for increased metabolic rate (supplemental oxygen as ordered, provide measures to stimulate appetite & provide 8-10 8oz glasses fluids) Encourage oral hygiene from dehydration, damp cloth to forehead Identify onset and duration of febrile episodes Control environmental temp to 21 C to 27 C (70 F to 80 F) |
|
|
What is THE indicator of circulatory response? |
Pulse |
|
|
What regulates the strength of ventricular contraction and the stroke volume? |
Mechanical, neural, and chemical factors |
|
|
The volume of blood pumped by the heart in one minute is the ___________________. |
Cardiac output, the product of HR, and the ventricular stroke volume. |
|
|
In an adult the heart normally pumps ______ of blood per minute. |
5000 mL |
|
|
Nonpharmacological therapies for reducing fever |
Blankets cooled by circulating water delivered by motorized units increase conductive heat loss. Make sure that nursing measures to enhance body cooling do not stimulate shivering. Avoid tepid baths, Bathing w alcohol-water solutions, Applying ice packs to groin and axillae areas, And cooling fans Medications to reduce shivering are meperidine and butorphanol |
|
|
Fever related to drug therapy |
hypersensitivity response to a drug. With other allergy symptoms such as rash or pruritus (itching) Treatment: withdrawing Med, treating any skin integrity impairment, educating the patient and family about the allergy |
|
|
If you detect an abnormal rate while palpating a peripheral pulse, the next step is to _____________. |
Assess the apical rate |
|
|
Pulse deficit |
An inefficient contraction of the heart that fails to transmit a pulse wave to the peripheral pulse site. To assess: assess radial and apical rates simultaneously and then compare rates. The difference between the apical and radial pulse rates is the pulse deficit. |
|
|
Pulse rhythm |
Is either regular or irregular |
|
|
People who have a congenital absence of sweat glands or a serious skin disease that impairs sweating are ___________. |
Unable to tolerate warm temps because they cannot cool themselves adequately. |
|
|
Dysrhythmia |
An interval interrupted by an early or late beat or a missed beat indicates an abnormal rhythm. Described as regularly irregular or irregularly irregular |
|
|
Character of the pulse include: |
Rate, rhythm, strength, equality apical rate and rhythm only |
|
|
Pulse equality |
Assess pulses on both sides comparing the two. A pulse in one extremity is sometimes unequal in strength or absent in many disease states (ex. thrombus formation) |
|
|
Factors influencing HR INCREASING pulse rate |
Exercise (short term exercise) Temperature (fever and heat) Acute pain Emotions (anxiety) Medications (positive chronotropic drugs such as epinephrine) Hemorrhage (sympathetic stimulation increased by loss of blood) Postural changes (standing or sitting) Pulmonary conditions (asthma, COPD) |
|
|
Factors influencing HR DECREASING pulse rate |
Heart conditioned by long term exercise Hypothermia Chronic pain Negative chronotropic drugs such as digitalis, beta adrenergic and calcium blockers Lying down |
|
|
Nursing diagnoses for pulse |
Activity intolerance Anxiety Acute pain Decreased cardiac output Deficient/excess fluid volume Impaired gas exchange Ineffective peripheral tissue perfusion |
|
|
Respiration |
The mechanism the body uses to exchange gases between the atmosphere and the blood and the blood and the cells. It involves ventilation, diffusion, and perfusion. |
|
|
Ventilation |
The movement of gases in and out of the lungs |
|
|
Diffusion |
The movement of oxygen and carbon dioxide between the alveoli and the red blood cells |
|
|
Perfusion |
The distribution of red blood cells to and from the pulmonary capillaries |
|
|
Skin in temperature regulation |
The skin regulates temp thru insulation of the body, vasoconstriction, and temperature sensation. The skin, subcutaneous tissue, and fat keep heat inside the body. People with more fat have more natural insulation than do slim or muscular people. |
|
|
Analyzing respiratory efficiency requires: |
Assessing ventilation by determining respiratory rate, depth, rhythm, and end-tidal carbon dioxide (EtCO2) value. And assessing diffusion and perfusion by determining oxygen saturation (SpO2) |
|
|
Hypoxemia |
Low levels of arterial O2 |
|
|
During a normal, relaxed breath, a person inhales ______ of air. |
500 mL (the tidal volume) |
|
|
Eupnea |
Normal respiration |
|
|
Respiratory depth |
Described as deep, normal, or shallow |
|
|
Respiratory rhythm |
Regular or irregular |
|
|
Alterations in breathing patterns |
Back (Definition) |
|
|
Factors influencing respirations |
Back (Definition) |
|
|
Factors affecting oxygen saturation |
Back (Definition) |
|
|
Blood pressure |
The force exerted on the walls of an artery by the pulsing blood under pressure from the heart. |
|
|
Alterations in breathing patterns |

Back (Definition) |
|
|
Factors influencing respirations |

Back (Definition) |
|
|
Factors affecting oxygen saturation |

Back (Definition) |
|
|
Pulse pressure |
The difference between systolic and diastolic pressure |
|
|
Blood pressure reflects the interrelationships of: |
Cardiac output Peripheral resistance Blood volume Viscosity Vessel elasticity |
|
|
Factors affecting body temp |
Age(temp reg unstable till puberty, usual temp range drops as individuals approach older adulthood) Exercise (any form increases metabolism & heat production and thus body temp) Hormone level (hormonal variations during the menstrual cycle cause body temp fluctuations, menopause) Circadian rhythm (normally changes 0.5-1 C during 24h period, usually lowest 1-4 AM & highest at 4 PM. Does not change with age but does with Occupation) Stress (physical and emotional stress increase body temp) Environment (affect infants and older adults more often bc their temperature-regulating mechanisms are less efficient) Temperature alterations (fever, hyperthermia, heatstroke, heat exhaustion, hypothermia) |
|
|
Patterns of fever |
Sustained Intermittent Remittent Relapsing |
|
|
Sustained fever |
A constant body temperature continuously above 38 C (100.4 F) that has little fluctuation |
|
|
Cardiac output |
BP depends on cardiac output As cardiac output increases, more blood is pumped against arterial walls, causing the BP to rise. |
|
|
False high diastolic |
Deflating cuff to slowly Inflating to slowly |
|
|
Factors affecting BP |
Age (adults BP tends to rise w advancing age) Stress (anxiety, fear, acute pain increase BP) Ethnicity (HTN in African Americans & Hispanics) Gender (males after puberty higher BP, after menopause higher BP) Daily variation (lower during sleep between midnight & 3 AM. highest 11 AM- 6 PM) Medications (antihypertensives, diuretics, other cardiac meds, opioid analgesics lower BP, vasoconstrictors & an excess volume of IV fluids increase BP) Activity & weight (a period of exercise can reduce BP for several hours afterward. During activity= increased BP. Inadequate exercise=weight gain & obesity= HTN smoking (BP rises during & returns 15 mins after stopping) |
|
|
Antihypertensive medications |
Back (Definition) |
|
|
Hypertension |
More common than hypotension Often asymptomatic Thickening and loss of elasticity in the arterial walls
|
|
|
Risk factors for hypertension |
Obesity, smoking, heavy alcohol consumption, high salt intake, sedentary lifestyle, stress. Greater in patients with diabetes and older adults |
|
|
Hypotension |
Systolic 90 or below Dilation of the arteries, loss of blood volume (hemorrhage), or failure of heart muscle to pump adequately (MI) |
|
|
S/S of hypotension |
Pallor, confusion, increased HR, decreased UOP, |
|
|
Orthostatic hypotension |
When a normotensive person develops symptoms & a drop in systolic pressure by at least 20 or diastolic by 10 within 3 mins of rising to an upright position Dehydrated, anemic, prolonged Bestest, recent blood loss most at risk |
|
|
Pain |
Intensity Location Quality |
|
|
In an older adult fever is present when _______________________. |
a single oral temperature is over 37.8 C (100 F), or repeated oral temperatures over 37.2 C (99 F) |
|
|
Peripheral resistance |
As resistance rises, arterial BP rises. When vessels dilate and resistance falls, arterial BP falls. |
|
|
Antihypertensive medications |
Back (Definition) |
|
|
Blood volume |
Most adults have a circulating blood volume of 5000 mL. When it rises, BP elevates. When blood volume falls (ex hemorrhage, dehydration) the BP falls. |
|
|
Viscosity |
The thickness or viscosity of blood affects the ease with which blood flows thru small vessels. Hematocrit determines blood viscosity. When hematocrit rises and blood flow slows, arterial BP increases. |
|
|
Hematocrit |
Percentage of RBC in the blood |
|
|
Elasticity |
Normally walls of an artery are elastic. As pressure in the arteries increases, the diameter of vessel walls increase. Arteriosclerosis- vessel walls lose their elasticity resulting in greater resistance to blood flow. Systolic pressure is more elevated than diastolic. |
|
|
Variations in BP |
Hypotension- systolic 90 or below Elevated 120-129 or 80 or above Stage 1 HTN 130-139 or 80-89 Stage 2 HTN 140 or above 90 or above |
|
|
False low BP reading |
Bladder or cuff to wide Arm above heart level |
|
|
False high BP |
Bladder or cuff too short Too loose Arm below heart level Arm not supported |
|
|
False low systolic & false high diastolic |
Deflating cuff too quickly Stethoscope fits poorly or impairment of hearing |