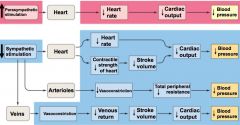
Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
145 Cards in this Set
- Front
- Back
|
layers of digestive tract
|
mucosa
submucosa muscularis externa serosa |
|
|
digestive tract mucosa
|
mucous membrane- epithelial barrier w/ mucus producing cells
lamina propria- acellular connective tissue "basement membrane" muscularis mucosa- smooth muscle >> tube runs down from mouth to anus; basic components remain the same but certain layers will be emphasized depending on the area/function 1/ esophagus- transport; thick muscularis, minimal mucosa 2/ small intestine- thin muscularis, elaborate mucosa layer for max absorption |
|
|
muscularis externa
|
outer longitudinal muscle
contraction >> shortens tube inner circular muscle contraction >> decreases tube diameter |
|
|
epithelial tissue
|
made of epithelial cells that are specialized for selective transport across membranes; *very tight junctions
|
|
|
apical v. basal v. lateral surfaces
|
apical- faces anterior lumen
basal- faces underlying vascular tissue lateral- faces neighboring epithelial cells |
|
|
goblet cells
|
produce mucus
|
|
|
exocrine v. endocrine cells
|
exocrine- secretes/releases digestive enzymes & juices into anterior of GI
endocrine- produce/releases GI specific hormone into blood stream; designed to regulate and coordinate GI function |
|
|
serous membrane
|
visceral peritoneum- covers organ
parietal peritoneum- lines inside the organs *continuous w/ one another |
|
|
mesentery
|
double layer of peritoneum that connects the visceral and parietal portion
serves as a conduit for blood vessels, nerves, and lymphatic vessels |
|
|
digestive processes
|
1/ motility
2/ secretion 3/ digestion 4/ absorption |
|
|
motility // mechanism rules
& their exceptions |
propulsive movements // peristalsis
wave of muscle contraction that moves down GI tract *accomplish both movements in stomach mixing // segmentation contraction primarily circular muscle contraction that moves around the tube *accomplish both movements in small intestine |
|
|
secretion
|
mucus is secreted throughout the gut, product is dependent on location within tract/accessory gland(s)
HCl-, digestive enzymes, & bile salts |
|
|
digestion
|
carbohydrates--
polysaccharides uses amylase >> maltose >> monosaccharides disaccharides (e.g. sucrose and lactose) can be broken down by the tongue proteins >> polypeptide fragmins >> amino acids fats-- triglyceride (3 fatty acid chains attached to glycerol backbone) uses lipase >> monoglyceride & two free fatty acid chains |
|
|
absorption
|
*most important
small intestine has specific mechanism for transporting water, monosaccharides, fatty acids, and AA across mucosal wall and into blood vessels |
|
|
non-digestive functions of GI tract
|
excretion
fluid/electrolyte balance- small intestine reabsorbes up to 9-11 L/day immunity- large barrier for pathogens; lymphocytes and mast cells are located in b/w epithelial and lamina propria GALT |
|
|
What happens if pathogen is able to cross GI and get into the blood stream?
|
hepatic phagocytic system!
Kupffer cells can endocytose pathogen and initiate immune response. |
|
|
short loop v. long loop regulation
|
short loop- local, gut can regulate digestive function autonomously w/o input from brain
long loop- brain can influence or override short loop |
|
|
enteric nervous system (ENS)
|
short loop, part of PNS
*intrinsic has two major neural networks-- 1/ myenteric plexus 2/ submucosal plexus |
|
|
myenteric plexus
|
located between longitudinal and circular muscle layers
>>regulates motility |
|
|
submucosal plexus
|
receives information r/t composition inside GI tract (e.g. distention, fat content, osmolarity, pH, bacteria content)
>> directly controls secretion >> indirectly influences gut motility by communicating w/ myenteric plexus >> indirectly influences absorption depending on what secretions it stimulates and its effect on motility |
|
|
How does the submucosal plexus influence absorption?
|
It can enhance digestive enzymes and slow down motility, resulting in (+) absorption. It can decrease digestive enzymes and have the opposite effect.
Toxins in the GI tract will cause increased water/mucus secretion and gut motility, (-) absorption. The net effect is the removal of the toxin. |
|
|
extrinsic control of gut
|
controlled by sympathetic stimulation and vagus nerve input (which is part of PNS but not part of the enteric system)
|
|
|
control and regulation of GI
|
endocrine cells release hormones via
1/ directly senses change in gut 2/ instructed by enteric submucosa plexus 3/ brain triggers release via vagus n. 4/ different GI hormone |
|
|
stomach
|
fundus
body antrum >>has two types of motility >>physically uniformed across the three portions w/ secretory cells @ bottom of gastric pits |
|
|
receptive relaxation
|
gastric filling
volume of stomach when empty- 50 mL >> can increase 20x when ruggae stretches before distention @ stomach wall |
|
|
peristalsis
|
pace setter cells are located along the fundus and are spontaneously active; depolarization only reaches threshold while consuming food
>> peristalsis will move down from fundus before reaching pyloris sphincter, chyme is able to get into duodenum || once it reaches sphincter, it will close, rebounding the chyme up the stomach to be mixed again |
|
|
oxyntic mucosa
|
*in body & fundus of stomach
mucosa cells-- produce thick alkaline mucus that acts as a protective coating against acidity of stomach chief cells-- produce pepsinogen >> pepsin, which breaks down proteins parietal cells-- HCL and intrinsic factor intrinsic factor binds to vit B12, it is necessary for the uptake of B12 in the terminal portion of the small intestine enterochomaffin-like cells-- acts like chief and parietal cells |
|
|
pyloric gland area (PGA)
|
only found in antrum
gastrin aka G-cells stimulates gastric secretion and motility by (+) chief & parietal cells and peristalsis somatostatin aka D-cells decreases gastric secretion and motility |
|
|
phases of gastric secretion
|
1/ interdigestive
2/ cephalic 3/ gastric 4/ intestinal |
|
|
interdigestive phase
|
not thinking about or eating food
gastric secretion is lowest in AM and highest in PM |
|
|
cephalic phase
|
cues are anticipatory; food has not entered stomach
*control is from long loop; (+) secretion & motility |
|
|
gastric phase
|
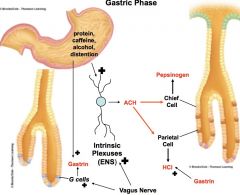
food enters stomach
*short and long loop; (+) secretion and motility |
|
|
intestinal phase
|
food leaving stomach & entering duodenum
*short and long loop; (-) secretion and motility predominately sensed by D-cells protein withdrawal & drop in pH >> (+) somatostatin |
|
|
What are three strong stimulus for the intestinal phase?
|
1/ low pH
2/ protein 3/ fat other factors include hypertonicity, distension when mucosa of duodenum sense these changes >> 1/ enterogastric reflex- slows gastric emptying 2/ enterogastrones- triggers 2 hormones responsible for pancreas and liver secretions |
|
|
What is the purpose of inhibiting motility?
|
slows gastric emptying so that duodenum can stimulate pancreas and liver for secretions
pancreas- digestive enzymes & NaHCO3 neutralizes acid liver- bile salts help w/ fat digestion >> fat slows down gastric emptying the most b/c its digestion starts and ends in duodenum |
|
|
enterogastrones
|
cholecytokinin (CCK)
(-) gastric emptying (+) pancreatic secretion (+) bile secretion secretin-- (-) gastric emptying (-) gastric acid secretion (+) NaHCO3 |
|
|
acinar cells v. duct cells
|
acinar cells- stimulated by CCK, releases digestive enzymes
duct cells- stimulated by secretin, releases NaHCO3 both pancreatic cells, digestive enzymes and NaHCO3 are secreted together |
|
|
pancreatic enzymes
|
1/ proteolytic
trypsin- first to be activated by amino peptidase >> will activate the rest- chymotrypsin, carboxypeptidase 2/ pancreatic amylase 3/ pancreatic lipase; the only source of lipase! therefore, if you eliminate pancreas function, fat digestion will be affected the most |
|
|
How are carbohydrates digested?
|
salivary amylase, start at the mouth
|
|
|
bile
|
composed of bile salts, cholesterol, lecithin, & bilirubin suspended in aqueous alkaline fluid
amphipathic and creates emulsification droplets when interacting w/ fat so that they cannot reform >> increases SA that lipase can act on |
|
|
CCK action
|
-secretes bile
-opens sphincter of odii -gall bladder contraction >> bile will emulsify >> 50% will get reabsorbed, when bile is reabsorbed back into liver, it is a strong stimulus for more bile secretion >> this system will only shut down when fat digestion is complete and CCK is no longer secreted |
|
|
small intestine
|
*where all food digestion and absorption will be completed
divided into duodenum, jejunum, & ileum primary motility is segmentation; responsible for mixing and propulsive actions |
|
|
segmentation
|
-a response to distention in the duodenum
-increases surface area of absorption w/ food -slow frequency at earlier, lower parts of intestine; higher frequency of segmentation in upper areas >> slow propulsive movements |
|
|
mucosal membrane of small intestine
|
brush border- membrane bound digestive enzymes
1/ enterokinases 2/ disaccharidases 3/ aminopeptidase arranged in villi and microvilli which increases SA available for digestion by 600x |
|
|
central lacteal of villas
|
fat that gets absorbed enters here, and eventually gets drained into the liver
|
|
|
disaccharides >> enzymes >> monosaccharides
|
maltose >> maltase >> glucose
sucrose >> sucrase >> fructose lactose >> lactase >> galactose amino fragments >> amino peptidase >> AA |
|
|
fat digestion/absorption
|
lipid emulsion droplets- triglyceride surrounded w/ bile salt
pancreatic lipase breaks down triglycerides to form micelles- fatty acid and monoglyceride surrounded by bile salts micelle is absorbable form of digestive fat, gets into brush border |
|
|
large intestine
|
no more food; if food gets into colon, bacteria will go into fermentation reactions >> gas
feces w/ H20, electrolyses, and mineral that we want back; moves from terminal ilium through iliocecal valve into cecum >> ascending colon >> transverse colon >> descending colon >> sigmoid colon >> rectum, etc. |
|
|
motility in colon
|
haustral contractions--
type of segmentation, mixes feces, increases contact w/ colon wall to (+) absorption mass movements-- propulsion, drives feces 3/4 or whole length of colon stimulated by gastrin if pushed into rectum, distention will stimulate defecation reflex |
|
|
defecation reflex
|
stretch receptors of rectal wall will cause relaxation of internal anal sphincter (smooth muscles, involuntary)
external anal sphincter- skeletal muscles, voluntary if defecation is delayed for too long, mass movement will move feces back into rectum >> the longer it stays in colon, the more water is absorbed >> stool will get hard >> constipation |
|
|
causes of diarrhea
|
1/ colonic motility is too fast, not enough time to absorb water
2/ osmotic- osmolarity of feces is elevated esp. undigested material in colon (usually caused by enzyme deficiency e.g. lactose, fiber) we cannot digest fiber and it is used as stool softener |
|
|
kidneys
|
-perfused by renal arteries
-filters blood and forms urine -filtered blood returns to heart via renal vein -urine goes through ureter >> bladder >> urethra two major zones-- 1/ cortex- outer, lighter in color 2/ renal medulla- organized into renal pyramids where urine collects before it is drained into renal pelvis >> ureters >> bladder |
|
|
How many nephrons does each kidneys have?
|
1 million; a healthy adult has a total of 2 million nephrons
each nephron has vascular and tubular component |
|
|
renal vascular blood flow
|

>> afferent arterioles- renal arteries form arterioles right before it enters kidneys
>> glomerulus (capillaries) >> efferent arteriole >> peritubular- network of of capillaries wrapped around tubule portion of nephron >> out of kidneys via renal veins |
|
|
exchange @ capillaries
|
1/ glomerulus 20%
2/ peritubular capillaries 80% |
|
|
glomerulus exchange
|
bowman's capsule >> proximal tubule >> descending loop of henle >> ascending loop of henle >> distal tubule >> urine is emptied into collecting duct
has same composition as plasma excluding particles that could not cross bowman's capsule (WBC, RBC, plasma proteins) as it moves down the nephron, there is opportunity for exchange (reabsorption) but once it leaves collecting duct into renal pelvis, there is no more modification in the composition of that urine |
|
|
nephron's regional differences
|
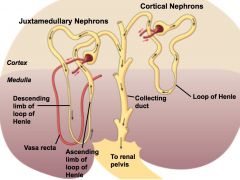
all originate in the cortex of the kidney, difference lies in the proximity to the glomeruli
cortical nephrons (80%) -outer cortex -short loop of henle that only enters superficial portion of medulla -peritubule capillaries wrapped around the entire tubule juxtamedullar nephrons (20%) -inner cortex -long loop of henle -peritubule capillaries wrapped only around tubule found only in cortex -vasa recta runs along the loop of henle -important in producing urine @ various concentrations |
|
|
formation of urine
|
1/ glomerular filtration
2/ tubular reabsorption 3/ tubular secretion if you knock out glomerular filtration, will be unable to form urine |
|
|
renal corpuscle
|
refers to glomerulus and bowman's capsule
|
|
|
glomerular membrane
|
barrier b/w glomerular capillaries and interior of bowman's capsule; composed of three layers
1/ capillary walls are composed of endothelial cells w/ pores **glomerulus' pores are significantly more leaky and allow small plasma proteins to pass endothelial layers 2/ basement membrane; acellular connective tissue **charge filter; glycoprotein has net (-) charge that repels plasma proteins that are also (-) 3/ inner membrane of bowman's **size filter; pedocytes have projections that wraps around glomerular capillaries--they inter digit, creating a very small slit |
|
|
forces in glomerular filtration
|
1/ capillary blood pressure
pushing of blood against capillary wall, wants to push fluid out into bowman's >> filtration 55 mmHg 2/ plasma colloid osmotic pressure pulling exerted by plasma protein, wants fluid in >> opposes filtration 30 mmHg 3/ bowman's hydrostatic pressure pushing, water pushes against its container >> opposes filtration 15 mmHg **capillary BP > colloid and hydrostatic pressure for normal filtration to occur net filtration pressure: 10 mmHg |
|
|
glomerular filtration rate (GFR)
|
depends on
-net filtration pressure -surface area available -permeability of glomerular membrane GFR = Kf x net filtration pressure, where Kf = SA x permeability Variation of GFR- gender and age Men has bigger kidneys >> more SA Decline of healthy nephron mass as people age >> less SA |
|
|
control of GFR
|
1/ autoregulation- maintain GFR w/ normal fluctuations in BP w/o regard to systematic BP; kidneys able to maintain independently via vasoconstriction and vasodilation
2/ extrinsic- alter GFR inorder to control blood volume and BP; stress response, emergency goal |
|
|
tubuloglomerular feedback mechanism
|
mediates autoregulation @ juxtaglomerular apparatus- part of distal tubule where afferent and efferent arteriole bifurcates
macula densa- tubule cells monitor the rate of fluid flow; indirectly measures GFR--(+) GFR will (+) fluid rate granular cells- vascular cells sense BP @ afferent arteriole; indirectly monitors systemic BP >> rise in either component will trigger vasoconstriction >> drop in either component will trigger vasodilation |
|
|
extrinsic control of GFR
|
sympathetic input can override autoregulatory responses
smooth muscle cells of afferent and efferent arterioles contain many a-adrenergic receptors (epinephrine and norepinephrine) >> stimulation will cause vasoconstriction afferent arterioles constrict >> (-) glomerular BP >> (-) GFR efferent arterioles constrict >> (+) filtration fraction **reduce GFR to lose less volume |
|
|
tubular reabsorption
|
100% of glucose is reabsorbed
99.5% of salt filtered in reabsorbed 99% of water filtered is reabsorbed >> has to cross laminal membrane, interior of cell, basolateral membrane, interstitial fluid, and endothelial of peritubular capillary |
|
|
reabsorption of Na+
|
80% of energy requirements of kidneys is used for Na+; usually coupled to reabsorb other solutes and perform other tasks
passively crosses luminal membrane // Na/ATP pump @ basolateral membrane reabsorbed @ every portion of nephron EXCEPT the descending loop of henle |
|
|
locations of Na+ reabsorption
|
proximal tubule- crucial role in reabsorption of glucose, AA, water, and urea
ascending loop of henle- important role in urine concentration distal tubule and collecting duct- under hormonal, regulates ECF volume and BP |
|
|
Na+ reabsorption in proximal tubule
|
*major adjustments to urine composition will occur in proximal tubule
Na+ is a cotransporter; sneaks in glucose, AA, water-soluble vitamins |
|
|
How does glucose end up in urine?
|
tubular max (TM)- maximal rate of transport, limited by # of cotransporters
renal threshold- max plasma concentration @ which you reach TM high concentration of glucose will overwhelm and saturate cotransporters; TM for glucose is 375 mg/min |
|
|
Na+ reabsorption in ascending loop
|
symports K+ and Cl- at laminal membrane
K+ and Cl- passively cross basolateral membrane |
|
|
Na+ reabsorption in distal tubule
|
symports Cl- at laminal membrane
Cl- passively cross basolateral membrane |
|
|
Na+ reabsorption in collecting duct
|
Na+ is alone, passive channel only @ laminal membrane
|
|
|
H2O reabsorption
|
80% of H2O is reabsorbed in the proximal tubule and loop of henle
usually follows Na+ reabsorption; however, H2O reabsorption is independent in distal tubule and collecting duct two mechanisms-- paracellular route- between epithelial cells transcellular route- through epithelial cells |
|
|
paracellular route
|
H2O moves through leaky tight junctions
lateral membranes are packed w/ K+/Na+ pump, causing an extremely high osmolarity @ tight junctions >> sucks H20 into interstitial space |
|
|
transcellular route
|
H20 has to move through cell via aquaporins
>> always present @ basolateral membrane >> varies @ luminal membrane H2O is NEVER reabsorbed @ ascending loop of henle |
|
|
chloride reabsorption
|
*electrical gradient
Na+ in the lateral membranes attracts Cl- across |
|
|
What follows H2O reabsorption?
|
H2O creates a concentration gradient by leaving; the solutes left behind (urea, Cl-, K+) will also move down its gradient through leaky tight junction
most commonly seen @ proximal tubule |
|
|
reabsorption of PO4- and Ca+
|
reabsorption of some substances helps regulate plasma levels of those substances
renal threshold = normal plasma levels >> if plasma level increases, only "X" amount will get reabsorbed and excess is secreted through urine *glucose is not apart of this system b/c its renal threshold is 3x normal |
|
|
What does not get reabsorbed?
|
waste products (except urea)
1/2 N+ gets recycled to make AA |
|
|
tubular secretion
|
movement of substances from peritubular capillaries into tubular lumen for elimination
|
|
|
H+ ion secretion
|
plays an important role in acid/base balance
acid ionizes in blood stream, H+ >> actively pumped through basement membrane >> exits laminal membrane via Na+/H+ antiporter @ proximal tubule facilitated diffusion @ collecting duct & loop of henle |
|
|
K+ secretion
|
K+ reabsorption is unregulated; it's passive and proportional to Na+ and H2O reabsorption @ proximal tubule
K+ secretion is regulated *only occurs in collecting duct and distal tubule where K+ channels are on the luminal membrane Aldosterone opens luminal Na+ channels and increases Na+/K+ ATPase expression |
|
|
anion/cation secretion
|
these organic ions can be endogenous or exogenous (e.g. food additives, pollutants, drugs); their excretion involves energy, and Na+ reabsorption
reasons why proximal tubules contains two secretory pathways for organic ions 1/ some are bound to plasma proteins and is never filtered by the glomeruli >> this is a second opportunity to get rid of them 2/ increase the speed of elimination |
|
|
urine concentration
|
![100 mOsm to 1200 mOsm
body is in perfect balance when it produces 300 mOsm, which is isotonic
[urine] increases as it gets closer to the renal pelvis](https://images.cram.com/images/upload-flashcards/1018754/2408101_m.jpg)
100 mOsm to 1200 mOsm
body is in perfect balance when it produces 300 mOsm, which is isotonic [urine] increases as it gets closer to the renal pelvis |
|
|
obligatory water loss
|
we have to lose water, cannot stop producing urine--therefore, body is better dealing w/ persistant overhydration than persistant dehydration
|
|
|
loop of henle permeability
|
descending
permeable to H2O, impermeable to Na+ ascending permeable to Na+, impermeable to H2O >> urine that leaves loop of hence will have low osmolarity (after losing Na+); 100 mOsm >> sets up absorption gradient for collecting duct |
|
|
medullary countercurrent system
|
![nephron structures working together to vary [urine]
-loop of henle of juxtamedullary nephrons are responsible for creating gradient
-collecting duct uses this gradient
water gets reabsorbed at collecting duct and will increase [urine]](https://images.cram.com/images/upload-flashcards/1018754/2408104_m.jpg)
nephron structures working together to vary [urine]
-loop of henle of juxtamedullary nephrons are responsible for creating gradient -collecting duct uses this gradient water gets reabsorbed at collecting duct and will increase [urine] |
|
|
vasopressin (ADH)
|
determines how much water is reabsorbed by determining the permeability of H2O
>> binds to tubular epithelial cell, increases cyclic AMP to increase aquaporins on laminal surface @ distal tubule and collecting duct |
|
|
ECF volume
|
helps maintain blood pressure and blood supply to tissue
|
|
|
ECF osmolarity
|
helps maintain cell volume
regulated by maintaining water balance; assuming body has fixed # of solute, you want to maintain water to keep osmolarity @ isotonic concentration total body osmolarity is defined as the ratio of total-body osmoles to total-body water, where body osmoles is primarily determined by ECF sodium content regulation involves the detection of plasma osmolarity |
|
|
Na+ balance
|
gains- ingested Na+ absorbed through GI tract
losses- renal excretion & nonrenal loss (sweat, feces) |
|
|
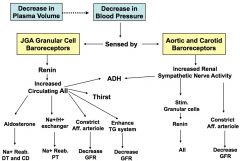
baroreceptors
|

changes in plasma volume are sensed by monitoring blood pressure
short term- aortic arch & carotid sinus long term- renal |
|
|
angiotensin II actions
|
these are long term regulations; sensed by JGA granular cell receptors; "renin, aldosterone, angiotensin"
increases sodium (and water) reabsorption 1/ stimulates aldosterone release @ distal tubule and collecting duct (indirect) 2/ stimulates Na+/H+ exchanger in proximal tubule (direct) decreases GFR 3/ direct vasoconstriction of afferent arterioles, elevating BP 4/ enhances tubuloglomerular feedback increased water consumption and reabsorption 5/ stimulates thirst and ADH secretion |
|
|
non-renal baroreceptors
|
any decrease in BP sent to brain >> increases sympathetic activity
1/ increase norepinephrine from renal nerve onto renal arterioles >> vasoconstriction to afferent arteriole 2/ renal nerves innervate JGA, stimulates granular cells >> increase renin >> angiotensin II 3/ increases ADH secretions |
|
|
summary control of plasma volume
|
|
|
|
water balance
|
gains- water consumed & water liberated from metabolic processes
losses- through urine, feces, sweat |
|
|
effector mechanisms for water/osmolarity balance
|
1/ diuresis
2/ thirst both part of negative feedback loop that starts in hypothalamus |
|
|
central osmoreceptors
|
circumventricular organs (CVOs)
SFO & OVLT senses the change in osmolarity >> releases ADH |
|
|
sensitivity of ADH release
|
plamsa osmolarity is 290 mOsm in healthy adults
threshold for ADH release is ~280 mOsm; that means any lower will shut down ADH release increases by as little as 1% in plasma osmolarity can produce a large increase in plasma ADH |
|
|
Where does angiotensin II intersect w/ the osmolarity system?
|
There are angiotensin II receptors on SFO and OVLT; brainstem is increasing sympathetic activity while simultaneously stimulating thirst and ADH
>> plasma osmolarity rises, plasma volume/BP drops |
|
|
inappropriate ADH release
|
rate of ADH breakdown--
e.g. when liver function declines, (+) plasma ADH pain, fear, trauma-- increases sympathetic activation, (+) ADH alcohol, (-) ADH |
|
|
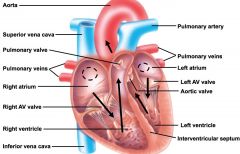
CV blood flow
|
|
|
|
AV valves
|
right <3 is tricuspid
L <3 is mitral -ensures unidirectional flow -strong cartilage to prevent collapse -leaflets are anchored by cordinae tendinae |
|
|
semi-lunar valves
|
shaped more like cusp; blood fills these cusp and helps seal this valve to prevent back flow of blood
|
|
|
pericardial sac
|
reduces frictional forces during contraction
|
|
|
cardiac muscle
|
-striated
-branching pattern *intercalated discs attach cardiac muscle cells to one another; at this junction; there are-- 1/ desmosome- protein anchors that physically attach one cardiac cell to the next 2/ gap junction- allows the 2 cells to be coupled electrically so that simultaneous contractions can occur |
|
|
cardiac cells
|
contractile muscle cells 99%
autorhythmic cells 1% |
|
|
contractile cells AP
|
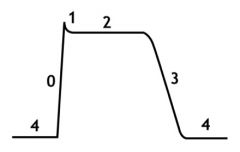
4/ resting membrane potential
0/ rapid depolarization; Na+ in 1/ closure of Na+ channel 2/ plateau; sustained by balance of Ca+ in and K+ out *AP is wider, plateau allows it to spend more time @ depolarization so that they can fire and contract muscles @ same time 3/ repolarization; Ca+begins to close while K+ continues to go out |
|
|
autorhythmic cells AP
|
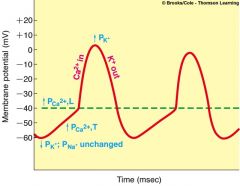
*never sustains a membrane potential
@ -60 mV, no gated channels are open but there is a leakage in Na+ channels >> causes slow depolarization transient Ca+ channel opens up enough for Ca+ to go in and reach threshold long type Ca+ channel opens, cell depolarizes Ca+ closes, K+ channel opens and K+ goes out |
|
|
autorhythmic cells
|
70-80 APs/min SA
40-60 APs/min AV 20-40 APs/min bundle of his & perkinje fibers SA node fires >> interatrial pathway to L atrium and internodal pathway to AV node *AV nodal delay (100 msec) maximizes ventricular filling; want this delay so that AV will cause R and L bundle of his to fire @ same time |
|
|
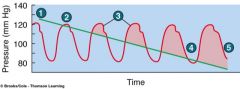
EKG
|
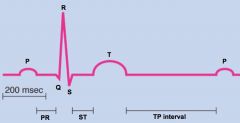
records all the cells in the heart
1/ P wave- depolarization of atria once SA node fires 2/ PR- represents AV nodal delay 3/ QRS- depolarization of both ventricles 4/ ST- ejection of blood from ventricles 5/ T- repolarization of both ventricles 6/ TP- diastolic time |
|
|
P wave
|
before--
atrial pressure > ventricular pressure allowing for passive filling >> ventricular volume increases during-- contraction (+) atrial pressure (green line exceeds red) (+) ventricular volume |
|
|
QRS complex
|
ventricular pressure exceeds atrial pressure (red line shoots up)
AV valve shuts causing -first heart sound -flat line of ventricular volume "end diastolic volume" isovolumetric contraction- time it takes for ventricle to create enough pressure to open aortic valve; must overcome aortic pressure |
|
|
ST
|
ventricular ejection
aortic valve opens; (+) in both aortic & ventricular pressure but ventricular pressure stays slightly higher than aortic (-) ventricular volume >> end systolic volume s/p ejection SV= EDV-ESV |
|
|
T wave
|
isometric ventricular relaxation
ventricular pressure falls below aortic pressure >> closure of aortic and pulmonic valves; causes 2nd heart sound and will continue to resting *dicrotic notch- when aortic valve closes, there is a bump in aortic pressure |
|
|
TP
|
passive filling
cardiac suction- dip in atrial pressure so that draws blood into atria; occurs during ejection phase while ventricles are contracting when ventricular pressure falls below atrial pressure, valves will open again >> passive rush of blood into ventricles *most of filling of ventricle is done passively during diastole |
|
|
CO
|
*primary measure of cardiac performance
CO = HR x SV cardiac reserve = max CO - reserve CO -max CO is affected by age; 220-age -exercise increases max SV, making the heart more efficient -heart failure will cause reserve to narrow >> activity intolerance |
|
|
<3 parasympathetic pathway
|
decreases heart rate
R and L vagus n. stimulate both SA and AV nodes SA receives more R vagus n. stimulation- releases acetylcholine and (-) firing rate AV receives more L vagus n. stimulation and (+) AV nodal delay |
|
|
<3 sympathetic pathway
|
releases norepinephrine
(+) firing rate @ SA (-) nodal delay @ AV; normally does not reduce ventricular filling unless you are very tachy |
|
|
T/F. Athletes have lower firing rate @ SA node.
|
False; natural firing rate remains the same--they have a higher vagal tone @ rest, which is why their HR is usually much lower
|
|
|
ejection fraction
|
healthy person should be able to eject ~55% w/ every beat
|
|
|
control of SV
|
SV is a function of contractility
1/ intrinsic control- increased filling *frank starling- more filling >> more stretch >> more force in contraction *length-tension relationship; changing length can change its potential tension -positional changes can enhance filling (if you feet are above your heart >> increase venous return to heart) 2/ extrinsic control- sympathetic stimulation to <3, directly creates stronger muscle contractions |
|
|
frank-starling graph
|
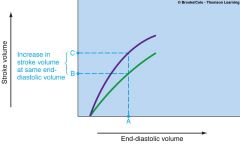
green- normal frank-starling
purple- frank-starling on sympathetic stimulation |
|
|
flow dynamics
|
F = pressure gradient / resistance
resistance -viscosity (ratio of plasma to RBC is stable) -radius of blood vessels (causes dramatic change) |
|
|
arterial BP
|
arteries
1/ transport from heart to tissues 2/ store pressure and provide driving force for flow when heart is resting BP- force of blood against vessel wall <3 contracts and empties >> stretch in arteries, registers as systolic BP <3 relaxes and fills >> arteries rebound, registers as diastolic BP |
|
|
mean arterial pressure (MAP)
|
MAP = diastolic pressure + 1/3 pulse pressure
average BP at anytime in artery; represents perfusion pressure @ all times ----------- How does arteriole diameter relate to BP? MAP = CO x TPR TPR is most influenced by arteriolar resistance |
|
|
measuring BP
|
korotkoff sounds--
(1) when radial pulse is no longer palpable >> above systolic pressure (2) cuff is just below systolic pressure; first sound is an estimate of systolic every subsequent tap is when BP exceeds cuff pressure sounds get more muffled as cuff pressure gets closer to resting pressure >> (5) no longer hear sound, cuff pressure is below diastolic; blood flow is no longer forceful and does not generate sound |
|
|
<3 intrinsic control
|
chemical--
local metabolic changes histamine release >> vasodilation physical-- temperature myogenic response to stretch >> momentary vasoconstriction |
|
|
What local metabolic changes will lead to vasoconstriction/vasodilation?
|
vasoconstriction
*endothelin released when endothelium senses (-) metabolic rate (+) O2 (-) CO2 (-) acidity, rise in pH (-) adenosine vasodilation *EDRD identified as nitric oxide is released (-) O2 (+) CO2 (+) acidity, rise in pH (+) adenosine |
|
|
<3 extrinsic control
|
sympathetic nerve fibers supply arteriole smooth muscle everywhere but the brain
releases norepinephrine which binds to 1/ beta receptors are found on smooth muscles that perfuse skeletal muscles >> vasodilation 2/ alpha receptors are found everywhere else >> vasoconstriction generally speaking-- (+) sympathetic >> vasoconstriction (-) sympathetic >> vasodilation |
|
|
@ rest v. exercise
|
@ rest-- total CO = 5,000
27% digestion 20% kidney 9% skin 13% brain exercise-- CO = 12,500 64% skeletal muscle 4.8% digestion 4.4% kidneys *no change in blood flow |
|
|
hormonal influence on arteriolar diameter
|
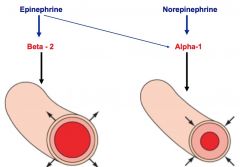
sympathetic activity releases epinephrine and norepinephrine--
-epinephrine has stronger affinity for beta receptors >> vasodilation -norepinephrine binds to alpha receptors >> vasoconstriction vasopressin (ADH) and angiotensin II >> vasoconstriction |
|
|
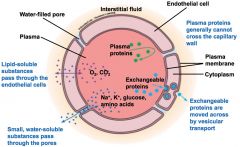
How are capillaries are highly adapted for diffusion?
|
1/ diffusion distance is minimized
2/ thickness of diffusion barrier is minimized 3/ surface area is maximized 4/ blood velocity slows down through capillary beds, maximizing the opportunity for diffusion |
|
|
How does blood flow rate remain constant if blood velocity slows down @ the capillary beds?
|
The increase in cross-sectional area compensates for the decrease in velocity.
|
|
|
transport across capillary wall
|
|
|
|
Explain why diameter of capillary is usually equal the diameter of RBC.
|
It is designed to minimize diffusion difference.
|
|
|
metarteriole v. capillary bed
|
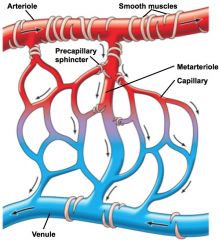
*precapillary sphincter determines whether blood will diffuse into capillary bed or if it will be diverted into metarteriole
> high metabolic activity relaxes sphincter >> capillary beds for more exchange, greater SA > low metabolic activity constricts sphincter >> metarterioles for less exchange, smaller SA *metarterioles are like shortcuts, moves quickly from arteries straight into venules |
|
|
bulk flow
|
-movement of ECF between plasma and interstitial fluid
-determined by passive forces >> ultrafiltration & reabsorption -will affect BP |
|
|
bulk flow forces
|
1/ capillary BP "pushing" >> ultrafiltration
2/ capillary oncontic "pulling" caused by plasma that cannot leave capillary >> reabsorption 3/ interstitial hydrostatic pressure "pushing" >> reabsorption 4/ interstitial oncotic pressure "pulling" >> ultrafiltration *minimal; this is theoretical--if protein is able to escape capillary |
|
|
reabsorption v. filtration
|
reabsorption--
capillary oncotic pressure & interstitial hydrostatic pressure is fixed in healthy adult; capillary oncotic pressure will decrease in ill patients w/ low albumin count filtration-- capillary BP is variable and will be greater than capillary oncotic and interstitial hydrostatic pressures if 1/ capillary sphincter is relaxed 2/ (+) plasma volume, (+) BP; will increase capillary BP pressure regardless of action @ sphincter site |
|
|
veins
|
-high capacitance vessel capable of holding large volume of blood
-vasoconstriction of veins means decreasing compliance and not allowing them to expand; this will cause (+) venous return to the heart |
|
|
increasing venous return
|
1/ sympathetic stimulation >> vasoconstriction >> (-) compliance >> (+) return
2/ skeletal muscles contract >> milk veins and encourages blood flow back to <3 3/ venous valves >> open and (+) venous return; close to prevent backflow 4/ thoracic cavity is 5 mmHg less than atm >> sucking pressure (+) return 5/ cardiac suction; ventricles contract >> atrial volume increases >> negative pressure >> (+) return |
|
|
orthostatic hypotension
|
blood starts to poll to leg after standing upright for a long period of time >> syncope
(-) venous return (-) CO (-) MAP |
|
|
baroreceptor reflex
|
short term regulation- carotid sinus baroreceptor & aortic arch baroreceptor respond to BP changes by altering their firing rates
**will eventually adapt to persistent change in BP and return to normal firing rate (+) BP >> (+) firing rate (-) BP >> (-) firing rate act by stimulating CV center in medulla >> (+) vagus n. >> (-) HR >> (-) CO >> (-) MAP |