![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
A 71-year-old woman with a past medical history of coronary artery disease, type 2 diabetes mellitus, and hypertension is brought to the Emergency Department with altered mental status. According to her husband, she has complained of polyuria and dysuria in the last three days and has taken some antibiotics left over from her previous urinary tract infection. Vital signs recorded immediately upon arrival reveal that her temperature is 37.1°C (98.8°F), pulse is 80/min, respirations are 14/min, and blood pressure is 145/90 mm Hg. The patient is not oriented to self, time, or place. She opens her eyes to command, and withdraws from painful stimuli. On physical examination, she has dry mucus membranes, decreased skin turgor, and delayed capillary refill. Laboratory workup is shown below. Blood Sodium 127 mEq/L Potassium 3.8 mEq/L Chloride 105 mEq/L Bicarbonate 24 mEq/L Urea nitrogen 41 mg/dL Creatinine 1.7 mg/dL Glucose 950 mg/dL Urine WBC >10 Bacteria many RBC 0-5/HPF Leukocyte esterase 2+ Nitrates 1+ Ketones none Bilirubin noneWhich of the following is the most likely cause of her altered mental status?[ 9.3%]A.Adverse drug reaction[ 9.3%]B.Diabetic ketoacidosis[ 0.0%]C.Hypertensive crisis[76.7%]D.Hyperosmolar hyperglycemic state[ 4.7%]E.Sepsis |
D.Hyperosmolar hyperglycemic state |
|
|
altered mental status can be caused by volume depletion - true/false |
true |
|
|
hyperosmolar hyperglycemic state is a complication of |
DM2 which can occur if a UTI is untx or not tx sufficiently |
|
|
lab findings for HHS in DM2 |
low Na normal bicarbonate high serum glucose elevated osmolarity |
|
|
immediate tx for HHS |
ABCs rehydration and correction of serum glucose |
|
|
diabetic ketoacidosis is a complication of |
DM1 but it can occur in DM2 also |
|
|
HHS has |
high serum glucose and osmolarity without (anion gap) metabolic acidosis seen in diabetic ketoacidosis infxn is a common trigger for HHS |
|
|
infxn is a common trigger for HHS true/false |
true |
|
|
A 31-year-old man with a history of type 1 diabetes mellitus presents to the Emergency Department for evaluation of generalized weakness. He is accompanied by his wife, who reports that the patient recently lost his job. Since that time, he has been drinking alcohol more often and has not been taking his insulin regularly. This morning he began to complain of nausea and had several episodes of non-bloody emesis. His temperature is 37.3°C (99.1°F), pulse is 108/minute, respirations are 22/minute, and blood pressure is 94/56 mmHg. On physical examination, he is ill-appearing with dry skin and mucous membranes and a fruity odor is noted on his breath. Mild epigastric tenderness is present without rebound or guarding. Laboratory studies are shown below. Blood Sodium 139 mEq/L Potassium 4.5 mEq/L Chloride 112 mEq/L Bicarbonate 10 mEq/L Urea nitrogen 16 mg/dL Creatinine 1.2 mg/dL Glucose 425 mg/dL Arterial blood gas pH 7.25 pCO2 21 mmHg pO2 94 mmHg Urine Glucose 4+ Blood negative Leukocytes negative Ketones 3+Which of the following is the most appropriate treatment for this patient? A.Insulin only[16.7%]B.Insulin and intravenous fluids[58.3%]C.Insulin, intravenous fluids, and potassium[25.0%]D.Insulin, intravenous fluids, potassium, and sodium bicarbonate[ 0.0%]E.Intravenous fluids only |
C.Insulin, intravenous fluids, and potassium |
|
|
diabetic ketoacidosis most often occurs when |
concomitant infxn missed insulin tx newly dx or previously unknown DM1 |
|
|
diabetic ketoacidosis fxs |
hyperglycemia low bicarb metabolic acidosis with ketones present in blood and urine |
|
|
dka is characterised by relative/absolute insulin |
def, thus insulin is key in tx fluid resus also key, as pxs are almost always vol. deplete +- K |
|
|
in DKA pxs usu. have depleted total body K despite |
normal/raised serum K this is due to extracellular shift of K, which occurs in the setting of acidosis in which excess H is transported into cell and K is transported out of the cell pxs with normal/low K should have K r/t initiated early in tx |
|
|
is sodium bicarb. used in tx of DKA |
RARELY - except in cases of severe acidosis <7 acidosis typically resolves in DKA with insulin and IV fluids |
|
|
DKA occurs most often in DM1 in the setting of |
infxn insulin noncompliance previously undx pxs |
|
|
tx for DKA |
insulin, IV fluids, K r/t |
|
|
A 39-year-old woman with a past medical history of anxiety presents to her primary care physician with weight gain in the past three months. She has had no recent change in her diet or exercise. She also complains of increasing fatigue, as well as swelling in her legs bilaterally. She takes buspirone for her anxiety. Her annual physical examination from 10 months ago was normal. Her temperature is 36.5°C (97.7°F), pulse is 82/minute, respirations are 12/minute, blood pressure is 152/105 mm Hg, height is 5' 2", and weight is 150 lbs (up 20 lbs since her last visit 10 months ago). Her examination is significant for a round face with excess facial hair, deep, purple striae on her abdomen and thighs, multiple ecchymoses on all four extremities, and 1+ pitting edema in the bilateral lower extremities.Question 1 of 2 in this setWhich of the following is the most appropriate next step?[85.4%]A.24-hour urine cortisol level[ 0.0%]B.CT scan of the abdomen[ 0.0%]C.MRI of the brain[14.6%]D.Serum adrenocorticotropic hormone (ACTH) level[ 0.0%]E.Serum corticotropin-releasing hormone (CRH) level |
A.24-hour urine cortisol level |
|
|
what are the screening tests of choice for suspected Cushing syndrome |
24hr urine cortisol OR low dose dexatheasone suppression test |
|
|
fxs of cushings syndrome |
unexplained weight gain new onset HTN hirsutism easy bruising pitting edema |
|
|
in cushings syndrome, once hypercortisolism is estabblished how do differentiate b/w ACTH dependent and ACTH independent Cushings |
serum ACTH level nb never use serum CRH |
|
|
A 39-year-old woman with a past medical history of anxiety presents to her primary care physician with weight gain in the past three months. She has had no recent change in her diet or exercise. She also complains of increasing fatigue, as well as swelling in her legs bilaterally. She takes buspirone for her anxiety. Her annual physical examination from 10 months ago was normal. Her temperature is 36.5°C (97.7°F), pulse is 82/minute, respirations are 12/minute, blood pressure is 152/105 mm Hg, height is 5' 2", and weight is 150 lbs (up 20 lbs since her last visit 10 months ago). Her examination is significant for a round face with excess facial hair, deep, purple striae on her abdomen and thighs, multiple ecchymoses on all four extremities, and 1+ pitting edema in the bilateral lower extremities.Question 2 of 2 in this setLaboratory workup reveals elevated 24-hour urine cortisol and elevated serum ACTH. Which of the following is the most reliable way to differentiate between pituitary and ectopic ACTH secretion?[ 2.1%]A.CT scan of the chest[12.5%]B.Inferior petrosal sinus ACTH[77.1%]C.Low dose dexamethasone suppression test[ 6.3%]D.MRI of the brain[ 2.1%]E.Peripheral venous ACTH |
B.Inferior petrosal sinus ACTH |
|
|
in cushings syndrome, after you've demonstrated elevated cortisol, what does an elevated ACTH represent |
suggest an ACTH dependent hypercortisolism |
|
|
ACTH can be secreted by the |
pituitary or ectopic sources ie small cell lung cancer |
|
|
inferior petrosal sinus directly drains |
venous blood from the pituitary, thus, the most reliable way to monitor ACTH production from the pituitary |
|
|
cushing syndrome work up |
check cortisol if high using either: -24 urine cortisol or - low dose dexamethasone suppression test once you have confirmed high cortisol with one of these tests, next measure ACTH, to see if pituitary or ectopic source of ACTH, using: - inferior petrosal sinus ACTH OR - high dose dexamethasone suppression test remember that high dexamethasone suppression test will only tell you if pituitary cause of high ACTH not ectopic production |
|
|
why is CT/MRI not initial mgmt for pituitary cause of cushings |
because of incidentalomas may be found elsewhere |
|
|
peripheral vein ACTH does not differentiate b/w |
pituitary and ectopic production of ACTH |
|
|
inferior petrosal sinus drains the |
pituitary |
|
|
the inferior petrosal sinus ACTH is the most reliable way of differentiating b/w |
pituitary and ectopic production of ACTH |
|
|
A 45-year-old female with a past medical history of hypertension, type 2 diabetes mellitus, obesity, and obstructive sleep apnea presents to her physician for routine follow up. She is taking hydrochlorothiazide, lisinopril, glyuburide, and insulin. She has also been using a continuous positive airway pressure (CPAP) machine every night for the past 3 months. The patient reports compliance with her medications. In addition, she exercises 30 minutes daily for five days a week and has been consistent with the dietary recommendations made by her nutritionist; she has lost 10 pounds over the last 9 months. Her pre-prandial blood glucose concentrations range from 140 to 160 mg/dL and post-prandial concentrations range from 170 to 190 mg/dL. Her temperature is 37.1°C (98.8°F), pulse is 90/minute, respirations are 14/minute, blood pressure is 148/95 mm Hg, and body mass index (BMI) is 39 kg/m2. Which of the following is the best next step in the management of this patient?You left this question blank.[ 7.9%]A.Add atenolol[44.7%]B.Add insulin glargine[ 2.6%]C.Decrease oral food intake[44.7%]D.Evaluate for bariatric surgery[ 0.0%]E.Increase exercise level |
D.Evaluate for bariatric surgery |
|
|
indications for bariatric surgery |
BMI >40 or BMI b/w 35-40 with comorbidities ie DM2 and OSA - esp. if b/g difficult to control with lifestyle/meds |
|
|
a px who is b/w 35-40 with comorbidities ie DM2 and OSA who given the optimal meds and compliant with lifestyle mods ie 150min/week but still have poorly controlled b/g can be indicated for |
bariatric surgery |
|
|
A 54-year-old Caucasian woman with a history of asthma presents to her physician for her annual physical exam. Her asthma has been well-controlled other than an occasional cough at night. She notes an unintentional five pound weight loss over the previous three months. Her medications include albuterol as needed and a daily multivitamin. Physical examination reveals a 2 x 3 cm firm, non-tender, non-mobile mass in the thyroid gland. No cervical lymphadenopathy is noted. Examination of other systems is otherwise unremarkable. A serum thyroid stimulating hormone (TSH) level is normal. Question 1 of 2 in this setWhich of the following is the most appropriate next step in diagnosis?You left this question blank.[ 2.0%]A.CT scan of the neck[35.3%]B.Fine needle aspiration[ 0.0%]C.Immediate lobectomy and await final pathology report[ 3.9%]D.Thyroid scintigraphy[58.8%]E.Ultrasound of the thyroid gland |
E.Ultrasound of the thyroid gland |
|
|
what are the risk factors the increase the risk of malignancy for a thyroid nodule |
age <20 and >70 male dysphagia hx of neck irradiation firm, hard, or immobile nodule cervical lymphadenopathy |
|
|
first step in evaluation of a thyroid nodule |
TFTs if TSH normal, next step = US to evaluate size and anatomic spread If concern for cancer - do FNA |
|
|
whats the preffered imaging technique for pxs with isolated thyroid nodules found on exam |
US |
|
|
if px has thyroid malig. whats the tx |
lobectomy/thyroidectomy |
|
|
thyroid scinitigraphy uses radionuclide scanning to determine is a thyroid nodule is |
hot warm or cold based on the amount of radioactive isotope uptake only use if TSH decreased |
|
|
A 54-year-old Caucasian woman with a history of asthma presents to her physician for her annual physical exam. Her asthma has been well-controlled other than an occasional cough at night. She notes an unintentional five pound weight loss over the previous three months. Her medications include albuterol as needed and a daily multivitamin. Physical examination reveals a 2 x 3 cm firm, non-tender, non-mobile mass in the thyroid gland. No cervical lymphadenopathy is noted. Examination of other systems is otherwise unremarkable. A serum thyroid stimulating hormone (TSH) level is normal. Question 2 of 2 in this setThe patient undergoes ultrasound and then fine-needle aspiration biopsy of the thyroid nodule. A sample of the specimen is shown below. Which of the following is the most likely diagnosis? You left this question blank.[ 3.9%]A.Anaplastic thyroid carcinoma[17.6%]B.Follicular thyroid carcinoma[ 7.8%]C.Hürthle cell tumor[13.7%]D.Medullary thyroid carcinoma[56.9%]E.Papillary thyroid carcinoma |
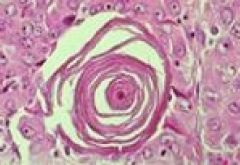
E.Papillary thyroid carcinoma |
|
|
Papillary thyroid carcinoma accounts for |
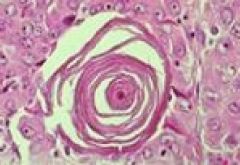
74-80% of all thyroid cancer histology will show lots of psammmoma bodies = round collection of calcium, with empty looking nuclei that stain uniformly, aka orphan annie nuclei, |
|
|
anaplastic thyroid cancer |
rare extremely aggressive pxs usually die within months of dx |
|
|
follicular thyroid carcinoma |
histology variable ie well formed follicles to mainly solid growth pattern key distinction = invasion of BVs by neoplastic follicles |
|
|
medullary thyroid carcinoma |
may be sporadic or familial familial type assoc. with MEN 2a/2b syndromes tumors derive from calcitonin producing parafollicular C cells histology = solid masses of cells with large vesicular nuclei; often large amount of fibrosis and amyloid deposition |
|
|
tumors that contain psamomma bodies mnemonic |
PSAMMoma Papillary thyroid cancer Serous cystadenocarcinoma of ovary Adenocarcinoma of the endometrium Meningioma Mesothelioma |
|
|
A 30-year-old woman presents with complaints of fatigue for the last 3 months. Over the last year she has been gaining weight, and is 10kg (22 lbs.) heavier. She used to be extremely active but has decreased energy throughout the day. She does have interest in hobbies such as skiing and running but does not have the energy to perform them now. She has also become very sensitive to cold. Her temperature is 37.5°C (99.5°F), pulse is 85/min, respirations are 15/min, and blood pressure is 100/55 mm Hg. On physical examination, she appears tired and has brittle hair and dry pale light colored skin. There is also some fullness of her face. Serum laboratory values are shown below. Hemoglobin 14 mg/dL Leukocytes 8000/mm3 Sodium 138 mEq/L Potassium 4.1 mEq/L TSH 0.1 µU/mL Free T4 3.5 µg/dL Cortisol (8 am) 2 µg/dLWhich of the following is most likely given this patient’s findings?You left this question blank.[ 6.7%]A.Autoimmune adrenal insufficiency[ 2.2%]B.Adrenal infarction[ 2.2%]C.Ectopic ACTH production[ 6.7%]D.Graves' disease[48.9%]E.Pituitary tumor[33.3%]F.Primary hypothyroidism |
E.Pituitary tumor |
|
|
pituitary tumor can cause |
hypothyroidism and adrenal insufficiency = 2o not 1o |
|
|
a px with a pituitary tumor may get hypothyroidism with decreased TSH due to |
damage to the pituitary (remember usu. in pit. tumor causing hypothyroidism, TSH is elevated) |
|
|
in 1o adrenal insuff. the cortisol and aldosterone are are usu. |
low leading to hyperkalemia and hyponatremia whereas in 2o adrenal insuff. - the Na and K may be normal |
|
|
1o adrenal insuff. |
darkening of skin due to increased ACTH prodxn to try compensate for lack of aldos. prodxn also up K and low Na due to deficiency in aldos. |
|
|
aldosterone moa |
works on collecting ducts to retain sodium by exchanging it for K without aldosterone, sodium will be excreted = low, and pxs develop hyperkalemia |
|
|
adrenal infarction follows periods of |
severe hypotension, usu. during surgery or trauma |
|
|
fxs of excess ACTH |
HTN, elevated Na, low K - due to up aldos raised cortisol |
|
|
graves dis. is an |
autoimmune condition that causes 1o hyperthyroidism |
|
|
2o adrenal insuff. and 2o hypothyroidism together suggest |
pituitary insufficiency, most likely caused by a pituitary adenoma |
|
|
sheehans syndrome |
post partum hypotension causing infarction of the pituitary |