![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
21 Cards in this Set
- Front
- Back
|
Physical properties of human enamel and dentine |
Enamel: 3% water Dentine: Enamel = hard+ stiff Dentine = flexible + compressible (to support enamel) |
|
|
Enamel structure |
HAP crystals (60-90nm width, 25-30nm depth) ordered into prisms/rods, Prisms almost perpendicular to amelo-dentinal junction. Circadian rhythm in enamel production = regular, daily, cross-striation-roughly 5 micron periodicity Incremental lines in periodicity = striae of retzius Crystals in fully mature enamel = less regular as they grow to occlude all available space. |
|
|
Dentine structure |
Non-collagen proteins present e.g. dentine phosphoprotein, growth factors present e.g. BMP, IGF's. Tubules increase + become wider towards pulp Superficial dentinal tubukes occupy 1% of dentine volume to 30% of deeper dentine Hence deeper dentine = more porous + permeable to bacteria + chemicals |
|
|
Early Enamel Caries White spot lesion |
Opaque white spot - sub-surface become porous as result of mineral dissolved by acid produced by plaque bacteria As porosity increases - lesion may take up stain + eventually begin to cavitate. |
|
|
Physical processes of early enamel caries |
Ca10(PO4)6(OH)2 ⇌10Ca2++ 6PO43– +2OH–
|
|
|
Enamel caries physical appearance Enamel caries = Purely chemical process, dissolution of HAP by acid. |
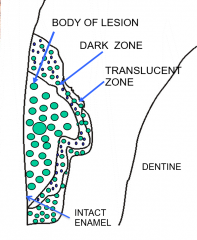
1) Translucent zone 2) Dark zone = increase porosity, small holes inaccessible to imbibing fluid 3) Body of lesion = more porosity, large pores. |
|
|
Caries in dentine |
Caries in dentine (3 stages) 1) Mineral is removed by the bacterial acid 2) Ground substance is removed by enzymes 3) Enzymatic removal of the collagen |
|
|
How does dentine initially respond? |
- Production of peritubular dentine to occlude tubules (inhibit diffusion of bacterial acids + enzymes). - This results in translucent + sclerotic dentine, the lesion will progress slowly here. - Crown of younger tooth wont have time to do that. Odontoblasts will first try wall off the lesion with sclerotic dentine, if they don't have time theyll increase amount of dentine at pulpal surface, producing reactionary dentine. However if lesion progresses rapidly then odontoblasts may be killed and replaced with more bone-like material (reparative dentine) |
|
|
What exists inside the pulp space |
Pulp dentine complex, dentine is vital tissue with cellular component that maintains the dentine structure, takes part in the innervation of the tooth as proprioception, allows defensive mechanism to be instigated. |
|
|
Defensive mechanism is 2 fold: |
1) Expression of chemicals that are antibacterial in nature combat bacterial contamination/infection of the dentinal tubules 2) Secretion of HAP by the odontoblasts to create + lay reactive or secondary dentine to close dentinal tubules from advancing noxious agent + protect the pulp |
|
|
What are the effects of bacteria upon pulp-dentine complex |
Loss of vitality + bacterial colonisation by proteolytic gram -ve facultative anaerobic bacteria of pulp space and dentinal tubules |
|
|
Pulp-dentine complex; response to invasion |
Odontoblasts - live in pulp/dentine interface and extend long cellular processes through dentinal tubules. Odontoblasts also exhibit features of innate immune cells including expression of TLRs Can progress so you can identify 7 to 31 different species, associated with degradation of dentinal matrix and stimulation of odontoblasts. Bacterial stimulation causes odontoblasts to undergo major functional adaptations; deposition of intertubular dentin and accelerated dentinal matrix deposition referred to as reactionary dentine. |
|
|
Spread of caries into dentine (smooth surface caries) Stage 1 |
Plaque layer forms on enamel surface, along with time + fermentable carbohydrates + lack of fluoride ions, causes release of organic acids. Lesion tends to progress down areas of high porosity + low mineral content |
|
|
Spread of caries into dentine (smooth surface caries) Stage 2 |
Acid dissolution of enamel prisms at prism boundaries and centre of prisms, loss of mineral, increased porosity + acid attack advances through enamel. |
|
|
Spread of caries into dentine (smooth surface caries) Stage 3 |
Spreads along ADJ laterally |
|
|
Spread of caries into dentine (Smooth surface caries) Stage 4 |
Dentinal tubules decrease in volume as intertubular dentine is laid down to become sclerotic and reactionary dentine on the pulpal wall |
|
|
Spread of caries into dentine (smooth surface caries) Stage 5 |
Enamel surface cavitates, plaque bacteria enters enamel and into dentine (infected dentine) |
|
|
Spread of caries into dentine: Occlusal/pit caries |
Spread of caries within dentine may produce large hidden lesion below smaller enamel lesion, sometimes called occult caries. Can be called fluoride syndrome resulting from enamel having high fluoride content + being relatively resistant to caries. |
|
|
3 layers when caries process enters into dentine: |
Coronal layer of dentine, exposed through open cavity, exposure to bacteria + saliva. Gross distribution of organic matrix, no recognisable dentinal tubules. Proteolytic bacteria consuming type 1 collagen |
|
|
3 layers when caries process enters into dentine: Affected dentine |
Closer to pulp, recognisable dentine structure affected by waves of demineralisation. Dentine slightly demineralised as crystals are dissolved. Possible to see isolated bacteria in superficial zones of the affected dentine, not heavily infiltrated |
|
|
3 layers when caries process enters into dentine: Normal dentine |
Normal dentine with tubules, tubules reduced in size as odontoblasts lay down secondary dentine inside tubules to form impenetratable layer. As caries gets closer to pulp layer gets thinner so risk of direct pulpal exposure. Likely micro-pulpal exposure has occured before visible exposure. |