![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
70 Cards in this Set
- Front
- Back
|
Hypocalcemia: presentation |
Convulsions Arrhythmias Tetany Spasms and stridor |
|
|
Hypernatremia |
Fever Restless Increased fluid retention & BP Edema Decreased urine output, dry mouthhy |
|
|
Hyperkalemia |
Muscle weakness Urine oliguria/anuria Resp distress Decreased cardiac contractility ECG changes Reflexes- hyper or flaccid |
|
|
Abdo pain: Ix |
- CBC, lytes, BUN/Cr, glucose, Urine, B-hCG if Repro age - +/- liver enzymes, LFT’s, lipase, troponin, ECG, VBG/lactate - +/- AXE, CXR, U/S, CR |
|
|
ALT & AST |
AST > ALT alcohol related ALT < AST viral, drugs, toxins |
|
|
Chest Pain: History |
- OPQRST - Previous episodes? Change frequency/severity? - Assoc. w/ meals, exercise, stress, position? - Assoc. w/ sweating, pallor, nausea, SOB, cough, palp, presyncope? - Relieved by rest or walking? |
|
|
Chest Pain: PMHx |
- Cardiac RFs- HTNN, DM, DLD, obesity, smoking - Recent events- med procedure, immob, travel, Ca, preg, illlness, trauma |
|
|
Chest Pain: Ix |
- CBC, lytes, glucose, troponin, CK, PTT, INR, ECG - +/- D-dimer, echo, spiral CT, CT chest, TEE |
|
|
Chest Pain: STEMI, NSTEMI, Angina |
STEMI- morphine, O2, nitro, ASA, BB, Clopidogrel NSTEMI- same Angina- ASA, BB, ACEi, nitro prn |
|
|
Chest Pain: Tension pneumo |
needle decompression at 2nd ICS MCL then chest tube |
|
|
Chest Pain: PE |
Heparin or LMWH |
|
|
Chest Pain: Red flags |
- sudden onset, tearing pain - nitroglycerin doesn't work - (pre-) syncope - dyspnea at rest - pleuritic chest pain - hemoptysis |
|
|
Dyspnea: History |
- OPQRST - Previous episodes - Chest pain - Orthopnea, PND - Leg swelling/pain/erythema - Hemoptysis, trauma - URTI, rhinorrhea, pharyngitis, cough, sputum, swallowing dysfunc, sick contacts, travel - Environmental exposures |
|
|
Dyspnea: ROS |
- neck mass - CHF - cough - fever - chills - bowel & bladder - bleeding |
|
|
Dyspnea: Risk Factors |
- obesity - smoking - occupational exposure - aspiration - decreased mobilization |
|
|
Dyspnea: Red Flags! |
- fever, night sweats, weight lolss - syncope - chest painn - hemoptysis |
|
|
Dyspnea: Ix |
- CBCd, lytes, Cr, urea, glucose, troponin, CK, VBG - +/- D-dimer - CXR, ECG +/- Echo, VQ scan |
|
|
Dementia |
- acute onset fluctuating LOC - disordered attention & cognition - impaired orientation - hallucinations - transient delusions - asterixis +/- tremor |
|
|
Delirium |
- insidious onset, stable over 24 hrs - alert consciousness - normal attention - impaired cognition & orientation - no hallucinations or delusions - no abn mvmts |
|
|
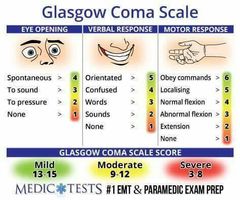
GCS |
|
|
|
Delirium: Ddx |
Drugs/toxinns Infection Metabolic Structural SAH, neurosyph, encephalitis, meningitis |
|
|
Delirium: Ddx |
- hemodynamic instability, collapse - sudden N/V - pregnancy - extremes of age - thunderclap H/A |
|
|
Delirium: Cushing's reflex |
- sign of high ICP - HTN, bradycardia, irregular respirations |
|
|
Delirium: Ix |
- CBCd, Cr, urea, lytes & extended, glucose, VitB12, PTH, liver enzymes, bilirubin, INR, TSH, tox screen, B-hCG, serum osmolality, osmolar gap, ABG/VBG - UA, C&S, blood culture, urine/blood tox - CXR, CT head, MR brain - +/- ECG, EEG, LP, paracentesis |
|
|
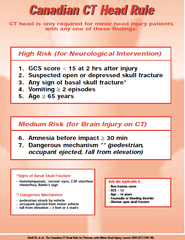
Canadian CT head rules |
|
|
|
Abdo Pain: Red Flags! |
- severe pain - shock (hypoTN, oliguria, abn MS, met acidosis, cold/clammy) - peritoneal signs - abdo distension - blood in urine/stool - anorexia, weight loss - abdo pain, organomegaly - fever - jaundice - waking up in pain |
|
|
Abdo Pain: Ix |
- CBCd, lytes, Cr, urea, glucose, B-hCG - UQ or middle abdo pain- AST, ALT, ALP, bili, lipase - Urine & blood culture - INR, PTT, T&S (if imminent OR) - +/- CXR, AXR, U/S, CT, CT angio |
|
|
Tox screen |
- CBC - Electrolytes, including Ca, Mg, Phos - Creatinine - Glucose - Urea - ALT, AST, - INR - VBG - Serum osmols - Acetaminophen level - Salicylate (ASA) level - EtOH level |
|
|
Sympathetic nervous system findings |
- Mydriasis - Aggitation, arrhythmia, angina - Tachycardia - Hyperthermia, HTN - Seizure, sweating - Slowed GI secretions - Tachycardia - Vasoconstriction - Dilated Airways - Diaphoresis / paleskin / Temp up |
|
|
Parasympathetic nervous system findings |
- Miosis - Increased GI secretions - Bradycardia - Vasodilation - Heart block - Constricted airways |
|
|
ABCs of toxicology assessment |
Airway Breathing Circulation D- GCS, pupils (clonus, hyperreflexia) E- flushed vs. pale, dry vs. diaphoretic, trauma F- find antidote |
|
|
Toxidromes: Anticholinergics |
- mad, blind, red, hot, dry - common culprits- TCAs, antihistamines, tegratol, cogenitin, anti-psychotics, atropine, Jimson weed |
|
|
Toxidromes: Anticholinergic mgmt |
- supportive - benzos for aggitation - ice packs, fans, chilled IV fluids for hyperthermia |
|
|
Toxidromes: Sympathetic common culprits |
- caffeine, alcohol withdrawal, cocaine, amphetamines, LSD (acid), MDMA/ecstacy |
|
|
Toxidromes: Sympathetic mgmt |
- supportive - benzos for aggitation - manage hyperthermia - wide qrs- have pads on, sodium bicarb |
|
|
Toxidromes: Muscarinic |
|
|
|
Toxidromes: Nicotinic |
Muscle cramps Tachycardia Weakness Twitching Fasciculations |
|
|
Cholinergics: Common culprits |
- anticholinesterase - nicotine - mushrooms |
|
|
Cholinergics: mgmt |
- consider external decontamination - scene safety - tx aggitation w/ benzos - significant doses of atropine |
|
|
Toxidrome: Opioids |
- Miosis - hypothermia - bradycardia - hypotension - respiratory depression - decreased LoC |
|
|
Opioid: Mgmt |
- monitor resp status - naloxone - Tx goals: SpO2 > 92%RR > 12EtCO2 < 45 |
|
|
Migraine |
- unilateral throbbing h/a - worse with activity, moderate-severe - N/V, photophobia, phonophobia - aura- flashing lights, loss of vision, paresthesia, dysarthria |
|
|
Tension H/A |
- unilateral non-throbbing h/a - not worse with activity - 30 min-7 days - triggered by stress, sleep-deprivation |
|
|
SAH |
- thunderclap h/a - worse with exertion, N/V, meningeal signs - CT - LP if suspecting SAH but normal CT after 6 hrs |
|
|
High ICP H/A |
- worse in AM/supine/bending/cough/Valsalva - CN exam!! - Papilledema |
|
|
Meningitis |
- H/A, fever, nuchal rigidity, altered LoC, petechiae - early antibiotics +/- acyclovir, dexamethasone |
|
|
Temporal Arteritis |
- H/A, scalp tenderness, jaw claudication, arthralgia, myalgia, malaise - temporal artery tenderness, RAPD, optic disc edema - high ESR, CRP - temporal artery bx, high dose steroids |
|
|
Causes of syncope by system |
HEAD, HEART, VeSSELS Hypoxia/hypoglycemia Epilepsy Anxiety Dysfunc brainstem Heart attack Embolism Aortic obstruction Rhythm disturbance Tachycardia Vasovagal Situational Subclavian steal ENT Sensitive carotid sinus |
|
|
Back pain: Emergencies |
Extraspinal- Aortic dissection, AAA, PE, MI, retroperitoneal bleed, pancreatitis Intraspinal- osteomyelitis, cauda equina, epidural, hematoma, spinal fracture |
|
|
Lower back pain: Mechanical causes |
- Lumbar strain/sprain - Degen (OA, spondylosis) - Spondylolisthesis - Osteoporosis - Fracture - Congenital (kyphosis, scoliosis) - Spondylosis - Facet joint asymmetry |
|
|
Lower back pain: Neurogenic causes |
- herniated disc - spinal stenosis - osteophytic nerve root compression |
|
|
Lower back pain: Non-mechanical causes |
- Neoplasia- MM, lymph, leuk, SC tumor, retroperitoneal tumor, mets - Inf- OM, septic disc, paraspinal absc, epidural abs, endocarditis, herpes zoster - Inflamm- AS, RA, IBD, psoriatic spond - Osteochondrosis - Pagets |
|
|
Lower back pain: Visceral causes |
- Pelvic- prostatitis, endometriosis, PID - Renal- nephrolithiasis, pyelo, perinephritic abs - AAA - GI- pancreatitis, cholecystitis, penetrating ulcer - Fat herniation of lumbar spine |
|
|
Lower back pain: History |
- onset, duration, trauma/injury - site, severity, radiation (hip, bum, legs, feet) - timing - previous episodes - alleviating, aggravating factors - fever, weight loss, bowel/bladder/sexual dysfunc |
|
|
Lower back pain: Red Flags |
- loss of bowel/bladder control - saddle anesthesia - severe worsening at night/laying down - weight loss, hx cancer, fever - steroid/IV drug use - first episode >50 yo - widespread neuro signs - sig trauma |
|
|
Ddx flank pain |
Life-threatening- AAA, PE, appendicitis, renal vein thrombosis, renal malig/infarction, ectopic preg, obst, pancreatitis, cholecystitis Non life-threatening- MSK, pyelo, renal cysts, nephrolithiasis, hepatitis, shingles, PUD, diverticulitis, colitis |
|
|
Ddx hemoptysis |
PULM
a) Airway- acute/chronic bronchitis, bronchiectais, Ca, trauma, foreign body b) Parenchyma- inf (TB, pneum, absc, fungal), Ca, alveolar hemorrhage c) Vascular- PE, arteriovenous malf, pulm HTN, iatrogenic Cardiac- CHF, mitral stenosis Hem- thrombocytopenia, coagulopathy, anticoag |
|
|
Hemoptysis: History |
- OPQRST, previous episodes - quantity, color - recent RTI, inf contacts, incarc, travel, IVDU, homeless - Cough, dyspnea, epistaxis, CP, palp, PND/orthopnea - Immunosupp, bruising, joint infl - N/V, abdo pain, hematemesis, melena, BRBPR, hematuria |
|
|
Hemoptysis: Ix |
- CBCd, lytes, LFTs, liver enzymes, Cr, INR, PTT, U/A - +/- D-dimer, T&S, sputum gram stain & culture, cytology, blood culture - CXR!!! Consider CT, doppler U/S, CTA, V/Q scan - Flex bronch if normal CXR in male, >50 yo, >40 py |
|
|
Fatigue: types |
1) Generalized, difficulty initiating tasks 2) Fatigability, difficulty maintaining tasks 3) Mental fatigue
Somnolence (excessive sleepiness) is different. |
|
|
Fatigue: Killers |
- CHF - COPD - Angina - Malignancy - HIV |
|
|
Fatigue: Common |
- Anemia - Hypothyroid, DM - Depression/Anxiety - Viral illness - Post-MI - OSA - Disordered sleep - Meds - CKD |
|
|
Ddx: Falls |
Intrinsic cause- (pre) syncope, dizziness, MSK, neurogenic Extrinsic- drugs (anti hol, antiHTN, diuretics, EtOH), env, footwear Other- sensory, motor, cognition |
|
|
Falls: HPI |
S- symptoms associated w/ fall P- previous falls L- location A- activity preceding fall T- time of fall and on ground T- trauma |
|
|
Anaphylaxis: Diagnostic criteria |
- acute onset - skin and/or mucosal involvement - respiratory compromise and/or symptomatic hypotension |
|
|
Anaphylaxis: HPI |
- OPQRST - skin/mucosal sx- hives, swollen lips, tongue, uvula - airway sx- SOB, wheeze, bronchospasm, stridor - GI sx- crappy abdo pain, N/V/D - chronological order of exposure & sx - triggers |
|
|
Anaphylaxis: mgmt |
- ABCs, O2, GCS < 8 intubate - epi IM STAT - venous return- supine, LE elevated - IV access - continuous monitoring x 8 hrs |
|
|
Anaphylaxis: meds |
- solumedrol 125 mg IV - antihistamines - inhaled salbutamol - glucagon |
|
|
Back pain killers |
Epiduralabscess Caudaequina Cona medullaris AAA/AD Pyelo Pneumothorax PE OM Discitis, Myelitis |
|
|
Colon cancer- most commonly metastasizes to… |
- liver - |