Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
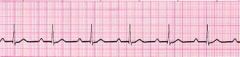
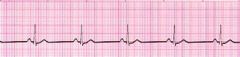
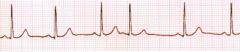
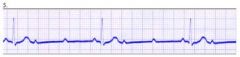
rate < 60
p-p / r-r regular PR int 0.12-0.20 constant QRS < 0.12 |
Sinus Brady
|
|
|
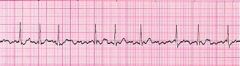
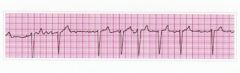
indiscernable Ps
irreg R-R fine fib baseline QRS < 0.12 |
A-fib
|
|
|
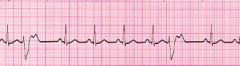
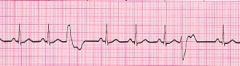
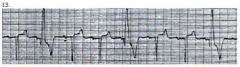
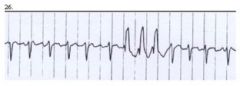
widened QRS (>0.12)
comp pause reg rhythm w/ premature beats rate usually normal |
PVCs
|
|
|
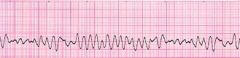
no discernable rythym/patterns
|
V-fib
|
|
|
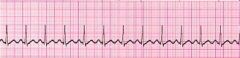
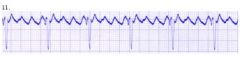
classic sawtooth waves
atrial rate regular vent rate reg to irreg PR not measurable QRS < 0.12 |
A-flutter
|
|
|
rate < 60
p-p / r-r regular PR int 0.12-0.20 constant QRS < 0.12 |
Sinus Brady - check for CCBs, BBs, digoxin
|
|
|
lengthening PR int
dropped QRS normal QRS int atrial rate reg vent rate irreg |
2 deg AV block Mobitz 1 (wenkebach)
|
|
|
widened QRS (>0.12)
comp pause reg rhythm w/ premature beats rate usually normal |
Multi-focal PVCs - more dangerous than uni-focal b/c both ventricles are involved - get BP then check hx/trends
|
|
|
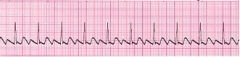
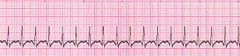
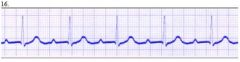
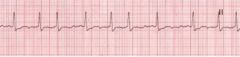
rate 101-180 bpm
PP / RR int regular PR int < 0.20 QRS < 0.12 |
Sinus tachy
|
|
|
rate 101-180 bpm
PP / RR int regular PR int < 0.20 QRS < 0.12 |
Sinus tach
|
|
|
usually normal rate
regular rhythm w/ premature beats PR int may be normal or prolonged QRS < 0.12 |
PACs
|
|
|
indiscernable Ps
irreg R-R fine fib baseline QRS < 0.12 |
A-fib
|
|
|
dropped QRS
atrial rate > vent rate P waves normal QRS int usually normal |
2 deg AV block Mobitz 2 (classic)
|
|
|
classic sawtooth waves
atrial rate regular vent rate reg to irreg PR not measurable QRS < 0.12 |
A-flutter
|
|
|
widened QRS (>0.12)
comp pause reg rhythm w/ premature beats rate usually normal |
Uni-focal PVCs - trigemini (every 3rd beat) - underlying rythym is neg def
|
|
|
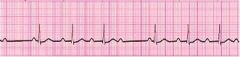
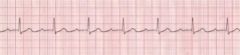
rate usually normal
rhythm regular P waves normal PR > 0.20 QRS normal |
1 deg AV block
|
|
|
indiscernable Ps
irreg R-R fine fib baseline QRS < 0.12 |
A-fib w/ triplet
|
|
|
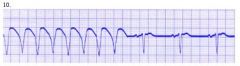
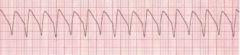
rate 101-250 bpm
rhythm reg P absent QRS > 0.12 |
V-tach followed by normal sinus
|
|

|
classic sawtooth waves
atrial rate regular vent rate reg to irreg PR not measurable QRS < 0.12 |
A-flutter
|
|

|
widened QRS (>0.12)
comp pause reg rhythm w/ premature beats rate usually normal |
Multi-focal PVCs
|
|

|
usually normal rate
regular rhythm w/ premature beats PR int may be normal or prolonged QRS < 0.12 |
PACs
|
|

|
indiscernable Ps
irreg R-R fine fib baseline QRS < 0.12 |
A-fib
|
|

|
widened QRS (>0.12)
comp pause reg rhythm w/ premature beats rate usually normal |
Uni-focal PVCs
|
|

|
widened QRS (>0.12)
comp pause reg rhythm w/ premature beats rate usually normal |
PVCs - uni-focal couplets
|
|

|
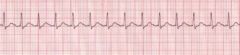
rate 101-180 bpm
PP / RR int regular PR int < 0.20 QRS < 0.12 |
Sinus tach
|
|
|
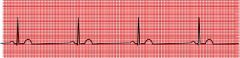
rate < 60
p-p / r-r regular PR int 0.12-0.20 constant QRS < 0.12 |
Sinus brady
|
|
|
lengthening PR int
dropped QRS normal QRS int atrial rate reg vent rate irreg |
2 deg AV block Mobitz 1 (wenkebach)
|
|
|
indiscernable Ps
irreg R-R fine fib baseline QRS < 0.12 |
A-fib
|
|
|
rate 101-250 bpm
rhythm reg P absent QRS > 0.12 |
V-tach
|
|
|
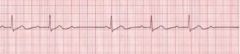
rate usually normal
rhythm regular P waves normal PR > 0.20 QRS normal |
1 deg AV block
|
|
|
rate 101-180 bpm
PP / RR int regular PR int < 0.20 QRS < 0.12 |
Sinus tach
|
|
|
dropped QRS
atrial rate > vent rate P waves normal QRS int usually normal |
2 deg AV block Mobitz 2 (classic)
|
|
|
tx for asymptomatic sinus brady
|
nothing
|
|
|
|
tx for symptomatic sinus brady
|
O2
IV access atropine ext pacing |
|
|
|
what is the atropine dose for sinus brady
|
0.5-1.0 mg up to total of 3 mg...if that is ineffective consider ext pacing
|
|
|
|
tx for sinus tachy
|
direct tx at underlying cause - beta blockers
|
|
|
|
tx for PACs
|
reduce stress
eliminate stimulants tx CHF correct electrolyte imbalance |
|
|
|
non-pharm tx for SVT
|
valsalva
CCBs BBs O2 and IV access |
|
|
|
pharm tx for SVT
|
adenosine 6 mg rapid IV push
repeat w/ 12 mg x 2 if BP drops <90 sys cardiovert @ 100 joules |
|
|
|
tx for a-fib
|
CCBs
BBs digoxin amniorarone cardiovert if meds ineffective |
|
|
|
tx for a-flutter
|
CCBs
BBs digoxin amniorarone cardiovert if meds ineffective |
|
|
|
tx for PVCs
|
tx underlying cause
Lidocaine mag replacement |
|
|
|
what is the lidocaine dose for PVC tx
|
lidocaine 1-1.5 mg/kg bolus
follow w/ lidocaine drip 1-4 mg/min |
|
|
|
tx for V-tach w/ pulse and BP > 90 systolic
|
lidocaine 1-1.5 mg/kg and 1-4 mg/min drip
amniodarone 150 mg |
|
|
|
tx for V-tach w/ pulse and BP < 90 systolic
|
cardiovert 100j, 200, 300, 360j
|
|
|
|
tx for pulseless v-tach
|
CPR - back board
defibrillation @ 360j 5 cycles CPR EPI 1 mg IV q 3-5 min or vasopressin 40 units IV bolus if no response to vasopress resume EPI after 10-20 mins amiodarone 300mg bolus and may repeat in 3-5 mins |
|
|
|
tx for v-fib
|
CPR - back board
defibrillation @ 360j 5 cycles CPR EPI 1 mg IV q 3-5 min or vasopressin 40 units IV bolus if no response to vasopress resume EPI after 10-20 mins amiodarone 300mg bolus and may repeat in 3-5 mins |
|
|
|
tx for 1 deg AV block
|
monitor closely
|
|
|
|
tx for 2 deg block mobitz 1 (wenkebach)
|
monitor for deteriorating rythms
temp ext pacing |
|
|
|
tx for 2 deg block mobitz 2 (classic)
|
temp pacing
EPI drip if pacing ineffective |
|
|
|
tx for 3 deg AV block (complete)
|
temp pacing
EPI drip if pacing ineffective |
|
|
|
atrial rate > vent rate
reg atrial rate irreg vent rate P waves normal PR int not measurable - inconsistent QRS can be narrow or widened |
3 deg AV block (complete)
|
|
|
|
rate = 150-250 bpm
rhythm reg to slightly irreg PR int not measurable QRS < 0.12 P waves not identifiable b/c hidden in preceding T wave |
SVT
|
|