Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
|
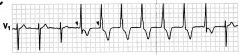
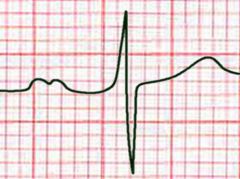
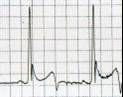
this is first degree heart block and may be caused by digoxin toxicity, beta blockers, hyperkalemia, acute rheumatic fever, inferior ischemia, sick sinus, myocarditis
|

What are some causes of this?
|
|
|
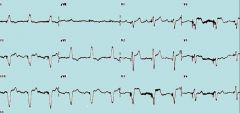
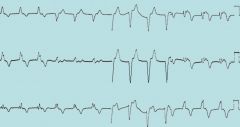
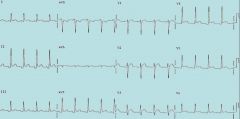
This is third degree block and should be treated with a pacer, as it will not respond to medications.
|

How do you treat this arrhythmia?
|
|
|
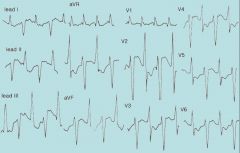
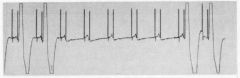
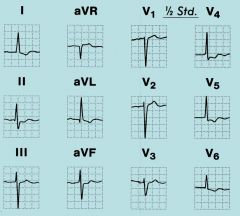
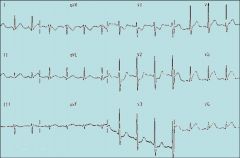
This is an accelerated idioventricular rhythm, which is a reperfusion rhythm in the setting of MI and should not be treated.
|
This patient had a STEMI and was lysed. What should you do about this rhythm?
|
|
|
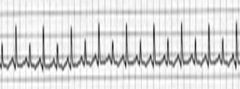
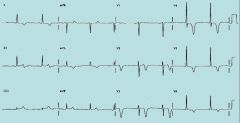
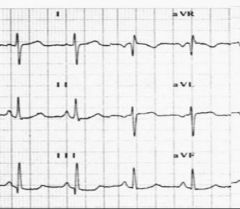
This is atrial fibrillation with aberrancy resulting in wide and bizarre QRS complexes.
|

What is this rhythm?
|
|
|
Any ST depressions in V1 or V2, concordant ST changes of 1mm or more, or discordant ST changes of 5mm or more.
|
This is a patient with a pacemaker. What changes make you concerned about MI in patients with pacers?
|
|
|
This is bidirectional V Tach, and it is pathognomonic for digoxin toxicity.
|
What is this pathognomonic for?
|
|
|
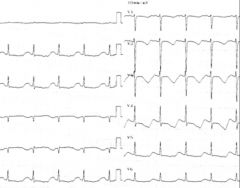
This is Brugada's syndrome, which is caused by an abnormality of sodium channels. Most patients present with syncope, and it is treated with AICD.
|

How did this patient likely present?
|
|
|
Thsi EKG shows electrical alternans, characteristic of pericardial effusion. In the setting of hypotension, this is tamponade, and is treated with pericardiocentesis.
|
This patient is hypotensive. How should he be treated?
|
|
|
This is a DDD pacer, and this strip demonstrates failure to capture. This can be caused by lead fracture, Twiddler's syndrome, ischemia, myocardial fibrosis, electrolyte abnormalities, or end of battery life.
|
What kind of pacer is this, and what are some causes of the problem?
|
|
|
This is hyperkalemia, and it is treated with calcium, glucose/insulin, bicarb, albuterol, kayexalate, and dialysis.
|
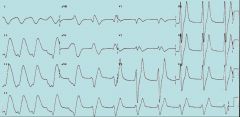
How can you treat this?
|
|
|
hypokalemia (hints are U waves and prominent P waves).
|
What electrolyte abnormality does this patient have?
|
|
|
this is an inferior MI, and is usually from a RCA lesion and sometimes from a circumflex lesion.
|
Where is the lesion?
|
|
|
left atrial enlargement
|
What does this show?
|
|
|
This is LBBB, and if it is new for the patient, that meets cath lab criteria. In addition, with an old LBBB, ST depressions in V1 and V2, concordant changes of 1mm, and discordant changes of 5mm are all suggestive of infarction.
|
What is this abnormality, and how can you detect a MI in its setting?
|
|
|
This is LVH, and it is caused by hyertension, aortic valve abnormalities, or it can be congenital.
|
What are some common causes of this?
|
|
|
This is Mobitz II, which is a high degree AV block. It is treated with pacing. Atropine is generally unaffected and may worsen the block to third degree.
|

What is this, and how is it treated?
|
|
|
Lung disease and right atrial enlargement
|

What are the common causes of this arrhythmia?
|
|
|
This EKG may represent a non ST elevation MI, or these may be Wellen's waves, which are deep, symmetrically inverted or biphasic T waves which signify left main coronary artery disease.
|
What is the significance of this EKG?
|
|
|
This patient has Osborne waves, which are downward slurring of the QRS. These occur with hypothermia.
|
What is likely wrong with this patient?
|
|
|
This patient has evidence of pericarditis, with PR depression and diffuse ST elevations which are concave upward. It is caused by viruses, bacteria, Lyme, uremia, autoimmune disease, radiation, MI, and several other causes. There are generally no EKG findings with uremic pericarditis.
|
What are some common causes of this abnormality?
|
|
|
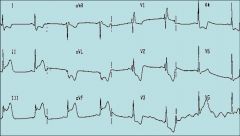
This is a posterolateral MI. Posterior MIs classically present with right sided heart failure and hypotension. They should be initially treated with fluid.
|
What kind of MI is this, and how should you initially treat hypotension?
|
|
|
This is right axis deviation, and it is caused by PE, lung disease, misplaced pacer, old anterolateral MI, left posterior hemiblock, and it is a NORMAL FINDING in children.
|
What are some causes of this?
|
|
|
This patient has peaked, narrow P waves, characteristic of right atrial enlargement.
|
What is this finding?
|
|
|
Right bundle branch block.
|

What is this finding?
|
|
|
RBBB, right ventricular hypertrophy, and sinus bradycardia.
|
What does this EKG show?
|
|
|
This is right ventricular hypertrophy. The criteria are R wave in V1 greater than 5mm, R to S ratio in V1 of >1, deep S in V5 and V6, and strain pattern in V1 and V2.
|
What is this finding?
|
|
|
This is SVT with retrograde P waves.
|

What is this?
|
|
|
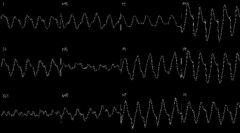
This is torsades, and may respond to magnesium or bicarb if it is associated with tricyclic overdose.
|
What medication might this patient respond to?
|
|
|
WPW type A. The short PR and delta wave give it away as WPW, and type A has a tall R wave in V1.
|
What does this EKG show?
|
|
|
This is an anteroseptal MI, and the lesion is in the LAD. This is known as the widowmaker.
|

Where is the lesion?
|
|
|
Hyperkalemia
|
This is a dialysis patient with hypotension. What is wrong?
|
|
|
This is an inferior MI.
|
Identify the problem.
|
|
|
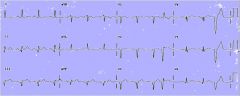
Nothing. He has evidence of J point elevation, which is common in this population.
|

This is a young African American male patient who got this EKG for pre-op screening. What is wrong with him?
|
|
|
This is ventricular fibrillation, which is treated with defibrillation at 200J.
|
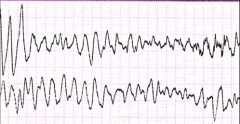
How is this treated?
|
|
|
This is Mobitz I, or Wenckebach, and if the patient has no symptoms, it is not treated.
|

What is this and how is it treated?
|
|
|
This EKG shows A-fib with a VVI pacer. This is the usual pacer for patients in a-fib, because it does not sense the atrial rhythm and therefore will not respond to the fibrillation with tachycardia, which would be undesirable.
|

What kind of pacer is this?
|