Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
52 Cards in this Set
- Front
- Back
- 3rd side (hint)

what is this measure
|
Atlantodental Interspace (ADI)
Projection: lateral neutral; flexion-extension cervical spine Measurements (mm): Min Max Adults 1 3 Children 1 5 Abnormal: Decreased space with age (DJD) Abnormally widened space w/ reduction in the neural canal size - trauma, occipitalization, Down’s syndrome, pharyngeal infections (Grisel’s disease, and inflammatory arthropathies (AS, spondylitis, RA, psoriatic arthritis, and Reiter’s syndrome |
|
|
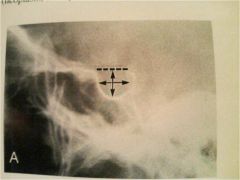
this is the sella turcica. signif of this measurement?
|
Sella Turcica
Projection: Lateral skull Measurements (mm): Avg Min Max AP 11 5 16 Veritical 8 4 12 Sella Turcica Abnormal: Small ST – debatable significance Large ST – pituitary neoplasm, empty sella syndrome, or extrapituitary mass (neoplasm, aneurysm) |
|
|
|
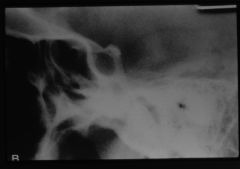
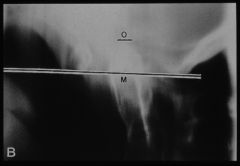
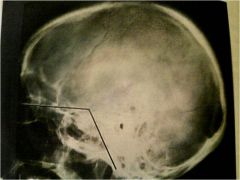
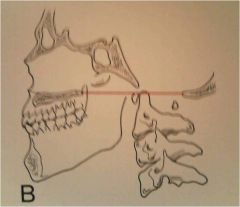
McGregor’s Line
Projection: lateral skull; posterosuperior margin of the hard palate to the inferior surface of occiput Normal measurements: in 90% of individuals the odontoid apex should not lie above this line more than: Males: 8 mm Females: 10 mm Significance: an abnormal superior position of the odontoid indicates basilar impression; platybasia, atlas occipitalization, and bone-softening disease of the skull base (Paget’s disease, osteomalacia, and fibrous dysplasia) |
|
|
|
|
Sella turcica size
– 5mm to 16mm – Avg is 11mm – Pituitary masses can cause enlargement |
|
|
|
|
Basilar Angle
|
– Avg 137 degrees
– 123 to 152 degrees – Baisilar impression and platybasia widen angle • Nasion to sella turcica to basion |
|
|

|
McGregors line
– Males: 8mm – Females: 10mm – Basilar impression when odontoid more than maximum distance above • Hard palate to occiput – Note relative odontoid apex Significance: an abnormal superior position of the odontoid indicates basilar impression; platybasia, atlas occipitalization, and bone-softening disease of the skull base (Paget’s disease, osteomalacia, and fibrous dysplasia |
|
|

|
Chamberlains line
– Basilar impression when odontoid more than maximum distance above – Hard Palate to opisthion |
|
|
Cervical Lordosis (aka angle of the cervical curve, cervical (lordotic) angle)
|
Projection: lateral
A: Depth of Cervical Curve – line from superior post. aspect of odontoid to the post. inferior corner of C7; The greatest transverse distance bet. this line and the posterior vertebral bodies is measured B: Method of Jochumsen – line from ant. border of atlas (tubercle) to the anterosuperior corner of the C7 body Measure from this line to the anterior border of the C5 body C: Angle of Cervical Curve – two lines: one thru and parallel to the inferior endplate of the C7 body and the other thru the midpoints of the anterior and posterior tubercles of the atlas (atlas plane line) Perpendiculars are then constructed to the point of intersection; the resultant angle is measured D: Method of Gore – line thru the posterior surface of C2 body and another through the posterior surface of the C7 body Angle formed by these tow lines is measure Normal Measurements: Average Minimum Maximum Depth(mm) 12 7 17 Jochumsen (mm) 3-8 1 9 Angle (degrees) 40 35 45 |
|
|
|
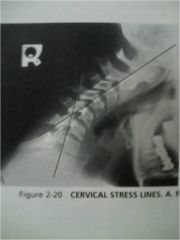
Stress Lines of Cervical Spine
– Flexion C5-C6 joint – Extension C4-C5 joint – Go through C2 and C7 vertebral bodies and note intersection |
|
|
|
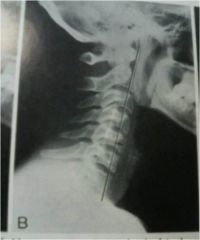
Cervical Gravity Lines
– Vertical line from odontoid apex – Passes through C7 body |
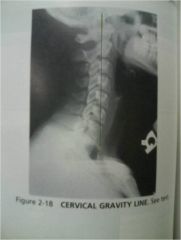
Significance: The line allows a gross assessment of where the gravitational stresses are acting at the cervicothoracic junction
|
|
|
|
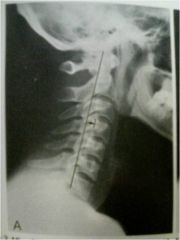
Georges Line
|

Projection: lateral
Normal – continuous / smooth line that traverses each posterior body corner Flexion and Extension films are especially useful in determining disruptions in George’s line Detects post-traumatic cervical injuries |
|
|

|
Atlantodental Interspace (ADI)
– C1 anterior tubercle – odontoid – Adult 1mm-3mm – Child 1mm-5mm – Transverse ligament rupture or instability. Trauma, Down’s, and inflammatory arthritis may increase the measurement |
|
|
|
|
Posterior Cervical Line
(aka Spinal Laminar Line (spinolaminar Line) Projection: lateral cervical spine (neutral, flexion, extension) Normal: when each spinolaminar junction point is joined, a smooth arc-like curve results (most anterior part of the convexity is compared between levels) Abnormal: in children, the spinolaminar junction line in children should not be > 2mm anterior to this line (at C2) Checks for anterior/posterior displacement Useful for detecting subtle odontoid fractures and atlantoaxial subluxation (anterior) Also locates anterolisthesis, retrolisthesis, or frank dislocation in the middle to lower cervical spine |
|
|
|
Saggital Dimension of the cervical spine
– Posterior body-spinolaminar junction. – 12mm minimum – Spinal stenosis when less than 12mm. Intraspinal tumor when enlarged |

|
|
|
|
Atlanto Axial Alignment
|

|
– C1 lateral mass-C2 articular pillar margin alignment
– Jefferson’s or odontoid fractures or alar ligament instability when margins overlap |
|
|
Prevertebral Soft tissue
|

|
– Anterior bodies-posterior air shadow margins
– Retropharyngeal 7mm • C2,3,4 – Retrolaryngeal 7-20mm • C4,5 – Retrotracheal 20mm • C5,6,7 • Soft tissue masses (tumor, infection, hematoma) increase the measurements |
|

|
Riser-ferguson
(not as good as Cobbs) |
Projection: AP Spine
Landmarks: End Vertebra – same as Cobb’s Apical Vertebra – this vertebral segment is the most laterally placed in the curve and usually the most rotated Vertebral Body Center – for each end vertebra and the apical segment diagonals are drawn from opposing corners of the body to locate center Connecting Line – two lines are constructed connecting the body centers of the apical segment with each end vertebra, and the resultant angle is measured. Significance: This method gives values approx. 25% lower than those of Cobb’s |
|
|
Thoracic Cage
|

|
– Posterior sternum-anterior T8 body
– Male: 14cm – Female: 12cm • Straight back syndrome when the distance is less than 13cm in males and 11cm in females |
|

|
– End vertebral endplate lines then intersecting perpendiculars and the angle measured.
– Used for scoliosis evaluation – GOOD METHOD |
Cobb’s Angle
|
|
|
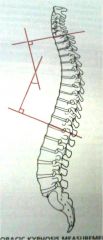
Thoracic Kyphosis
|
– T1 superior endplate-T12 inferior endplate, then intersecting perpendiculars and the angle measured
– Used for Kyphosis evaluation (Scheuermann’s fractures) |
|
|
– Hurxthal method (A) – endplate to endplate
– Farfan Method (B) – Ant Height divided by disc diameter, posterior height divided by disc diameter, then as ratio to each other • If decreased, then DJD, surgery, infection |
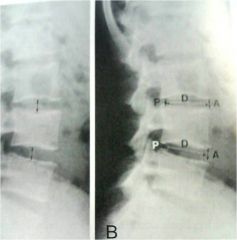
Intervertebral Disc Height
|
|
|

– At each disc endplate lines are drawn and the angles measured
• Altered in various pathologies |
Lumbar intervertbral disc angles
Significance – in facet syndrome the angles may be increased, whereas in acute discal injuries a reduction in the angle may be seen |
|
|

Lumbar lordosis
|
– L1 endplate–S1 endplate; perpendiculars and angle formed
– 50-60 degrees • Altered in various pathologies |
|
|
|
Lumbosacral angle
|
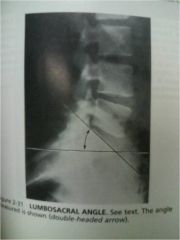
Projection: Lateral Lumbar Spine
Landmarks: two lines are drawn and the resultant angle is measured. First, a horizontal line is made parallel to the bottom edge of the film. Second, an oblique line is drawn through and parallel to the sacral base. The posterior angle thus formed is measured. Normal Measurements – a wide variation exists within normal individuals. Position Average Std Dev Min Max Upright 41 +- 7 26 57 Significance – An increased angle has been implicated as a mechanical factor in producing low back pain by increasing shearing and compressive forces on the lumbosacral posterior joints. An increased sacral base angle does not appear to be associated with an increased incidence of spondylolithesis. |
|
|
|
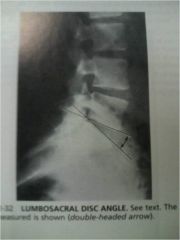
Lumbosacral disc angle
|
|
Landmarks: a line is drawn parallel and through the inferior endplate of L5 and superior endplate of the first sacral segment. The anterior angle formed by these lines is then measured.
Normal Measurements – the normal range appears to be between 10 and 15 degrees Significance – an increase in the lumbosacral disc angle > 15 degrees has been linked to the presence of low back pain caused by facet impaction. Also there may be a decrease in the angle in the presence of acute disc herniation of the L5 disc |
|
|
Hadley’s “S” curve
|

|
Landmarks: A curvilinear line is constructed along the inferior margin of the transverse process and down along the inferior articulating process to the apophyseal joint space. The line is then continued across the articulation to connect with the outer edge of the opposing superior articular process.
Normal Measurements: the resultant configuration of this line will look like the letter “S”. The key region of the “S” is the normally smooth transition across the joint space Significance: an abrupt interruption in the smooth contour of this line may indicate facet imbrication (subluxation), though displacements as great as 3 mm may not be visible on plain film. |
|
|
Van akkerveekens measurement of lumbar instability
|

|
– Endplate lines ar opposing segments. Measure from the posterior body to the point of intersection
– Should be equal measurements – Max is 1.5 mm difference • Nuclear, annular and posterior ligament damage if more than 1.5 mm difference |
|

|
Lumbar Gravity Line
|
Landmarks: The center of the L3 body is located by intersecting diagonals from opposing body corners. A vertical line is then constructed through this point, and the relationship to the upper sacrum is assessed.
Normal Measurements – according to Ferguson, the center of gravity of the trunk passes through the center of the L3 body and continues vertically to intersect the sacral base. Special Considerations – can be performed upright or recumbant Significance – if this line passes anterior to the sacrum by > 0.5 inches (> 10mm), an increase in shearing stresses in an anterior direction between the lumbosacral apophyseal joints maybe occurring. Conversely, it has been suggested that a posterior shift in this gravity line may indicate increased weight bearing forces on these same lumbosacral joints |
|
|
Static Vertebral malposition
Houston conference listings medicare listings |

|
Flexion – the endplates of the opposed segments diverge posteriorly in the lateral view
Extension – the endplates of the opposed segments converge posteriorly more than normal in the lateral view Lateral Flexion – the endplates of the opposed segments diverge laterally on one side and converge on the other side in the AP view Rotation – the pedicles are asymmetrical in shape, and the spinous may be deviated in the AP view Anterolisthesis – an anterior displacement of one vertebra body in relation to the vertebra below Retrolisthesis – a posterior displacement of one vertebral body in relation to the vertebra below Laterolisthesis – a sideways displacement of one vertebral body in relation to the vertebra below |
|

|
– Spinous position
– Intersegmental wedging – Usually toward concavity – Gradually increase away from sacrum • Disc herniation at level failing to laterally flex |
Lateral Bending Sign
|
|
|
Ullman’s Line
|

|
– Endplate line through S1, perpendicular from sacral promontory
– L5 should be behind the line • Detection of subtle spondylolisthesis when L5 body crosses perpendicular line |
|

|
Meyerding Rating System
|
– Sacral base divided into quarters. Relative position of the posterior body of L5 is made.
• Grading severity of spondylolisthesis NOT GOOD METHOD |
|
|
Klein’s Line
|
|
– Tangential line to outer femoral neck. Head just overlaps laterally
• Slipped epiphysis suspected if head does not intersect line. |
|
|
Boehler’s angle
|

|
– Three superior points joined on the calcaneus, posterior angle is measured
– Avg 30-35 degrees – 28-40 degrees is the range • Calcaneal fractures may reduce the angle to less than 28 degrees |
|
|
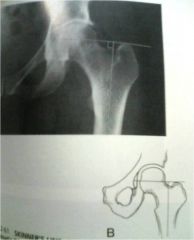
Skinner’s line
|
– Femoral shaft line. Perpendicular second line tangential to the tip of the greater trochanter
– Passes through or below fovea capitus • Hip joint abnormality if line passes above fovea capitus |
|
|
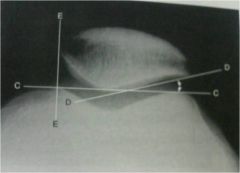
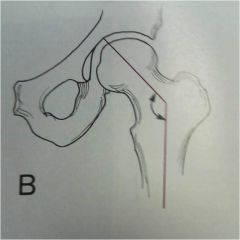
Center edge Angle / Wiberg’s
|
|
– From the center of the femoral head, vertically and acetabular edge, lines are drawn.
– The angle is then measured – Avg. 36 degrees – 20-40 degrees is range • A shallow acetabulum may precipitate DJD |
|
|
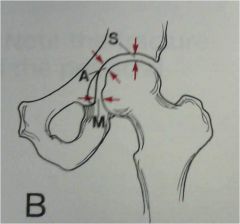
– Femoral head-acetabulum distance
– Superior = 3-6mm – Axial = 3-7mm – Medial = 4-13mm – DO NOT AVERAGE!!! • Various joint diseases increase the space – DJD, RA, Degenerative RA |
Hip joint space
|
|
|
Acetabular Angle
|

|
– Y-Y line drawn. Second line from medial to lateral acetabular surfaces. Angle measured
– Avg. 20 degrees – 12-29 degrees is the range • Congenital hip dislocation widens the angle. Down’s syndrome decreases the angle |
|
|
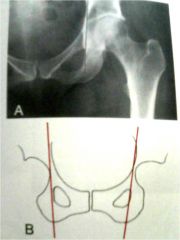
Pre-sacral space
|

|
– Soft tissue density between the rectum and anterior sacral surface
– Child: 3mm (1-5) – Adult: 7mm (2-20) • Diastasis and inflammatory joint disease may widen the joint. |
|
|
– The distance between opposing articular surfaces, Halfway between the superior and inferior margins
– Male:6mm (4.8-7.2) – Female: 5mm (3.8-6.0) • Diastasis and inflammatory joint disease may widen the joint. |

|
• Symphysis pubis width
|
|
|
Heel Pad Measurement
|

|
– Shortest distance between the calcaneus and plantar skin surface
– Male: 19mm – 25mm – Female: 19mm – 23mm • Acromegaly produces skin overgrowth exceeding the max measurement |
|
|
Patellar malalignment
|
– Patella length-patella tendon ratio
– 1:1 • Chondromalacia patellae factor if the ratio is exceeded more than 20% |
|
|
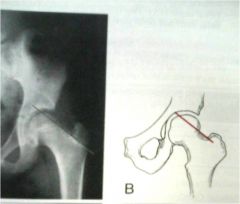
Protrusio Acetabuli / Kohler’s Line
|
– Pelvic inlet-outer obturator. Acetabulum should be lateral to the line
• Could be Paget’s disease when acetabulum is medial to the line |
|
|
|
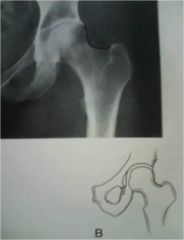
– Smooth curvilinear line along ilium and onto femoral neck and superior obturator border
• Femur dislocation or fracture if line is interrupted |
Shenton’s line
|
|

|
Shenton’s line
– Smooth curvilinear line along ilium and onto femoral neck and superior obturator border • Femur dislocation or fracture if line is interrupted |
|
|
|
Iliofemoral line
|
– Smooth curvilinear line along ilium and onto femoral neck
– Should be bilaterally symmetrical • Asymmetry may denote hip joint abnormality |
|
|
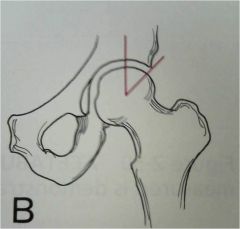
Femoral Angle
|
|
– Lines through the femoral shaft and neck
– 120-130 degrees is the range • Coxa vara: less than 120 degrees • Coxa Valga: Greater than 130 degrees |
|
|
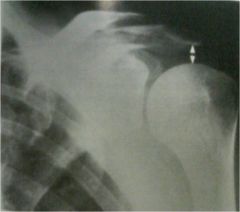
Glenohumeral joint space
|

|
– Average humeral head-glenoid distance (superior, middle, inferior)
– 4-5 mm • Degenerative and crystal arthritis diminish the space. Posterior dislocation may widen it. |
|
|
Metacarpal sign
|

|
– Tangential line through the fourth and fifth metacarpal heads. Third head should be proximal to this line
• Turners Syndrome, postfracture deformity |
|
|
Acromiohumeral joint space
|
– Acromion-humeral head
– Avg 9mm – 7mm-11mm is the range • Rotator cuff tear decreases distance. • Subluxation and dislocation increase the distance |
|
|
Acromioclavicular joint space
|

|
– Avg acromion-clavicular distance (superior, inferior)
– Male: 3.3mm (2.5-4.1mm) – Female: 2.9mm (2.1-3.7mm) • Degenerative arthritis will decrease distance • Seperation and resorption will widen distance |
|
|
Radio-capitellar line
|

|
– Radius axis line through the elbow joint
– Passes through capitellar center • Radius subluxation/dislocation if line misses the capitellar head |