![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
129 Cards in this Set
- Front
- Back
|
IL-1 |
Secreted: Monocytes, macrophages,B cells, dendritic cells, endothelial cells Target: T helpers, Hepatocytes, Hypothalamus Activity: Costimulatory, Fever, Protein induction |
|
|
IL-2 |
Secreted: T helper 1 cells Target: Activated T helper cells and CTLs Activity: enhance killing, proliferation Clinical: SCID results from gamma chain mutation, blocking increases success of transplants |
|
|
IL-3 |
Secreted: T helper 1 cells Target: Hematopoetic cells Activity: Growth factor for B, NK, T cells |
|
|
IL-4 |
Secreted: T helper 2 cells Target:B cells Activity: Activation, class switching to IgE/IgG blocking treats serious allergies |
|
|
IL-5 |
Secreted: T helper 2 cells Target: B cells Activity: activation, class switching to IgA |
|
|
IL-6 |
Secreted: Macrophages, T helper 2 cells Target: B cells, Hepatocytes, hypothalamus Activity: Differentiation to plasma cells and antibody production, acute phase protein induction, FEVER, stimulates hematopoiesis -blocking treats Rheumatoid arthritis |
|
|
IL-7 |
Secreted: Bone Marrow, thymic cells Target: B and T cell precursors Activity: differentiation |
|
|
IL-8 |
Secreted: Macrophages Target: Neutrophils (chemotaxis) Activity: Chemotaxis (attractant) |
|
|
IL-10 |
Secreted: Macrophages Target:Macrophages, T helper cells Activity: Down regulates pro-inflammatory response, shuts off fever mechanism |
|
|
IL-12 |
Secreted: Macrophages Target:T helper cells Activity:promotes differentiation of T helper cells to T helper 1 cells, also works with IL-18 to induce production of IFN-gamma, first cytokine to stimulate immune response |
|
|
IFN-alpha, IFN-beta |
Secreted: Leukocytes and fibroblasts Target: Infected cells Activity: inhibits viral replication by temporarily shutting off replication machinery in infected cells clinical: treat HBV- alpha, beta treat MS |
|
|
IFN-gamma |
Secreted: T helper cells Target: Macrophages Activity:Activates MO treat chronic granulomas |
|
|
TNF-alpha |
Secreted: Macrophages Target:Inflammatory cells Activity:Induces cytokine secretion, cachexia(wasting), FEVER inhibitors of this treat chronic inflammatory disease |
|
|
TGF-Beta |
Secreted: T regulation cells Target: T regulation cells, B cells Activity: promotes T regulation growth, IgA switching |
|
|
G-CSF |
Secreted: Macrophages, T helper cells Target: Bone marrow precursors Activity:Granulocyte development. |
|
|
GM-CSF |
Secreted: Macrophages, T helper cells Target: Bone marrow precursors Activity:Granulocyte development, MO development |
|
|
RANTES |
chemokine for Tcell/Monocytes |
|
|
Eotaxin |
Eosinophil chemokine |
|
|
T cell Receptor isotypes/ what helps transduce? B cell Receptor isotypes? |
Tcell- alpha/beta (NO SECRETION)/CD3 B-cell- IgM/IgD---/Ig-alpha,Ig-beta, CD19,CD21 |
|
|
Cells in thymic cortex? |
immature lymphocytes, nurse cells |
|
|
cells in thymic medulla |
t cells that survived selection, mature thymocytes |
|
|
signals needed for t cell activation? |

1. IL-1 2. CD28 and B7/CD80 interaction 3. MHC+antigen recongniton by T cell |
|
|
APC |
present antigen to T helper cells are B cells((CD40/CD40L interaction important here), Macrophages(must be activated by IFN-gamma to activate niave t cell) and Dendritic cells express B7 (CD80) |
|
|
Th0 to Th1 needs? |
IL-12, intracellular infection Th1 makes IFN-gamma, IgG isotype switching, activates MO |
|
|
Th0 to Th2? |
IL-4, parasitic infections IgE isotype switching makes IL-5,10 |
|
|
Th0 to Th17? |
IL-23,IL-6,TGF-beta, extracellular infections makes IL-17 and IL-22 to activate neutrophils, and increse barrier fx |
|
|
T regs + mucosal cella at infection site? |
secrete TGF-beta and IgA |
|
|
T Regs |
limits acrivation of Th1 cells, makes IL-10 |
|
|
Fas/FasL |
activation by CD8+ cells causes apotosis |
|
|
Zap-70 |
inside t cell, helps with signal transduction and is a tyrosine kinase |
|
|
CTL (cytotoxic t lymphocyte) |
specifically kills cells w/ TCR, needs MHC class 1 for killing, uses perforin |
|
|
T1 hypersensitivity |
Immediate, effector is IgE |
|
|
T2 hypersensitivity |
Cytotoxic(attacks tissue), IgG and IgM |
|
|
T3 hypersensitivity |
Immune complex, IgG and IgM |
|
|
T4 hypersensitivity |
Delayed response, T cells effectors, within 48hrs |
|
|
Mast cell mediators in T1 hypersensitivty rxn THAT ARE PRESTORED? |
histamine-SM contraction Heprin-anticoagulant ECF- chemotactic |
|
|
MAst cell mediators that are synthesized and released in T1 hypersensitivity rxn? |
Prostaglandin- SM contraction Leukotriene-SM contraction, chemotactic for neutrophil |
|
|
Bacillus anthracis |
dis: Anthrax Subunit: toxoid At risk individuals |
|
|
Corynebacterium diphtheria |
Diphtheria
Subunit: toxoid |
|
|
Haemophilus influenzae type B |
Meningitis Subunit: capsuleconjugate |
|
|
Neisseria meningitidis |
Meningitis Subunit: capsule conjugate (polysaccride+protien) |
|
|
Bordetella pertussis |
Whooping couch Killed Bacteria Subunit: toxoid, fimbriae |
|
|
Streptococcus pneumoniae |
Pneumonia, Meningitis Subunit: capsuleconjugate |
|
|
Clostridium tetani |
Tetanus Subunit: toxoid |
|
|
Salmonella typhi |
Typhoid Subunit: capsuleOral Live, attenuated Travelers |
|
|
Mycobacterium tuberculosis |
Tuberculosis Live, attenuated BCG Not used in the U.S. |
|
|
Vibrio cholerae |
Cholera Oral Killed + subunitOral killed Travelers |
|
|
Adenovirus |
Respiratory infection Oral: Live, attenuated Military personnel |
|
|
Hepatitis A |
Hepatitis Subunit : surface antigen |
|
|
Hepatitis B |
Hepatitis Subunit : surface antigen |
|
|
Human Papilloma virus |
Cervical cancer Subunit: outer coat protein |
|
|
Influenza |
Flu Nasal: live, attenuatedIM: killed |
|
|
Japanese encephalitis |
encephalitis Killed Travelers |
|
|
Measles |
Measles Live, attenuated Contraindicated:pregnant women, AIDS patients |
|
|
Mumps |
Mumps Live, attenuated Contraindicated:pregnant women, AIDS patients |
|
|
Polio |
Polio Sabin OPV: live, attenuated Salk IPV: killed OPV not used in the U.S. |
|
|
Rabies |
Rabies Killed At risk individuals |
|
|
Rotavirus |
Diarrhea Oral: live, attenuated |
|
|
Rubella |
German measles Live, attenuated Contraindicated:pregnant women, AIDS patients |
|
|
Shingles |
Shingles Live, attenuated Adults> 60 yrs old |
|
|
Smallpox |
Smallpox Live, attenuated |
|
|
Varicella |
Chicken pox Live, attenuated Contraindicated:pregnant women, AIDS patients |
|
|
Yellow Fever |
Yellow fever Live, attenuated Travelers |
|
|
Immunization |
Aquired active artifivial |
|
|
exposure to infecive agents |
aquired, active, natural |
|
|
maternal antibodies |
aquired passive, natural |
|
|
antibody infusion (ebola doc) |
aquired passive artificial |
|
|
aquired active? |
own antibodies |
|
|
aquired passive? |
ready made antibodies |
|
|
Small pox history |
edward jenner, started by cowpox(shares surface proteins with smallpox), discontinued imunization in 1972 bc smallpox was eradicated |
|
|
live attunated vaccines issues |
grown in secondary host (chicken) so people allergic to chickens will have issue advantages: confer strong immunity, can replicate disadvant: could revert to virulent form |
|
|
killed vaccine |
killed with formalin or heat adv: safe dis, not as strong immune response, large amounts needed |
|
|
conjugate vaccine? |

|
|
|
conjugate vaccine? |
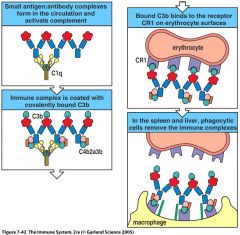
The first panel shows a naive B cell’s surface immunoglobulin binding a carbohydrate epitope on a vaccine composed of a Haemophilus polysaccharide (blue) conjugated to tetanus toxoid (red), a protein. This results in receptor-mediated endocytosis of the conjugate and its degradation in the endosomes and lyosomes, as shown in the second panel. Peptides derived from degradation of the tetanus toxoid part of the conjugate are bound by MHC class II molecules and presented on the B cell’s surface. In the third panel, the receptor of a TFH cell recognizes the peptide:MHC complex. This induces the T cell to secrete cytokines that activate the B cell to differentiate into plasma cells, which produce protective antibody against the Haemophilus polysaccharide (fourth panel).
|
|
|
Adjuvants |
A substance bound to the antigen to illicit a stronger immune response. Freund’s complete adjuvant: not for human useAlum: aluminum hydroxide: humans |
|
|
Autosomal RecessiveImmunodeficiencies |
RareBefore 1950’s, most patients died in childhood making it difficult to pass the gene on |
|
|
X-linked RecessiveeImmunodeficiencies |
More commonAffects mostly Men because they have only 1 copy of X |
|
|
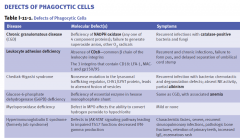
Phagocytic Deficiencies |
S.aureus, S.pnuemoniae, E.coli, Pseudomonas, Candida, Aspergillus recurrent bacterial or fungal infections |
|
|
Chronic Granulomatous Disease (CGD) |
Mutation in one of 4 genes for NADPH Oxidase X-linked Severe and recurrent infections with catalase positive organisms: Staphylococcus, Klebsiella, Serratia, Candida, Pseudomonas and Aspergillus Infections, if unresolved, lead to the formation of granuloma’s NBT(Nitroblue Tetrazolium Reduction)test for diagnosis--cell turns YELLOW for DISEASE, no NADPH Treated with antibiotics and IFN-γIFN tries to help MO do job |
|
|
catalase in bacteria??? |
protein that kills bacterias H2O2 which can casue issue with myleoperoxidase killing mechanism: |
|
|
Oxygen dependent killing? |
NADPH used to split O2 which makes toxic radicals, back up to this is myeloperoxidase which takes H2O2 and makes bleach to kill bacteria |
|
|
Leukocyte Adhesion Deficiency
|
Rare autosomal recessiveAbsence of CD18 (common beta2 chain of integrins)
Leukocytes cannot migrate OmphalitisInfection/inflammation of umbilical chord stump Chronic recurrent bacterial infections No abscess or pus formation leukocyte cannot stop rolling because no Integin to bind Patients suffer with recurrent pyogenic infections, impaired wound healing and severe gum inflammationCBC reveals leukocytosis and flow cytometry can determine the presence or absence of cell adhesion moleculesTreatment of choice is bone marrow transplant, antibiotics and IFN-γ gingivostomatitis |
|
|
Chediak-Higashi |
Rare, autosomal recessive disorder Affects the synthesis and maintenance of storage granules in many cell types including neutrophils, melaocytes, monocytes, NK cells Phagocytosed material is not delivered to the lysosomes because of a fusion defect Error with fusion of vesicles and MELANOCYTES SO ALBINO!!!!! Lab diagnosis is a routine blood smear revealing giant granules and neutropenia Recurrent bacterial Infections No NK activity (increased incidence of lymphomas) |
|
|
phagocyte deficiencies |
|
|
|
Complement Deficiencies |
Manifest similar to phagocytic deficiencies and antibody deficiencies Major sequelae associated with complement deficiencies Defects in opsonization Defects in lytic activity Defects in clearing of immune complexes C’ prevents immune complexes from formingC’ aids in the clearing of immune complexes |
|
|
common complement fx |
C3B-opsinize, clear immune complex Mac (C5-C9)-punch holes in things C5a,C3a—chemotaxis,anaphlatoxins (release of hostamines) inflammatory |
|
|
Complement |
blood proteins produced by the liver, spleen and macrophages primarily. They were originally discovered because of their ability, when activated, to lyse antibody-coated RBCs. |
|
|
complement activated do what? |
induce inflammation lyse certain infectious agents opsonize infectious agents Clear immune complexes |
|
|
classical complement pathway |
ab bind to specific antigen on pathogen surface, IgM and IgG |
|
|
lectin complement pathway |
mannose binding to pathogen surface |
|
|
alternative complement pathway |
pathogen surface creates environment conductive to pathogen binding Spontaneous lysis of C3, if binds to bacteria, initiate pathway |
|
|
complement activation |
All 3 pathways converge at C3 and result in a membrane attack complex (MAC) The larger proteins (b fragments for the most part) acquire enzyme activity The smaller proteins (a fragments) have biological activity and are known as anaphylatoxins |
|
|
opsonization |

Bacteria and other cells are delivered to phagocytes for destructionMolecules that aid this process are called opsoninsAntibody (IgG) and complement (C3b)Occurs via complement receptors |
|
|
Clearance of Immune Complexes |
Immune complexes (antigen and antibody complexes) are insoluble lattices Immune complexes trigger inflammation and type III hypersensitivity reactions |
|
|
Anaphylatoxins |
C3a and C5a split products diffuse away from the site of complement activation Can cause degranulation of mast cells and basophils without IgE Results:Plays a major role in the inflammatory responseC5a is a major chemotactic protein for inflammationIncrease vascular permeability, stimulate phagocytosis |
|
|
MAC!!? |
Pore forming molecules C5-C9 Lyses the cell Appears to be critical only for protection against Neisseria infections Deficiency in C5-C9 increase in Nesseria infections |
|
|
complement inhibitors?? |
C1INH inhibits C1.... |
|
|
(hereditary angioedema)
|
issue with C1-INH results in Overuse of C1, C4, C2; edema at mucosal surfaces bc complement rxn cannot be shut off |
|
|
issue with C5-9? |
recurrent meningococcal infections |
|
|
C3 issue |
recurrent bacterial infections, immune complex diseases |
|
|
issue with C4,C2,C1?
|
infections with pyogenic bacteria(cause purulent infection-pus forming) |
|
|
B Cell Deficiencies |
Usually characterized by recurrent bacterial infections with normal immunity to virus and fungal parasites |
|
|
X-Linked Agammaglobulinemia |
Mutation in a tyrosine kinase (Bruton’s Tyrosine kinase, btk) important in the development of pre-B cells to mature B cellsONLY HUMORAL DEFECT WITH NO B CELLS!. . Usually appears around 6 months of age and 80% present with pneumonia and other sinopulmonary infectionsTreated with IV injections of gamma globulin and antibiotics as needed |
|
|
Hyper IgM Syndrome (HIM) |
X-linked Mutation in CD40L on T cells CD40L is necessary for T cell communication with B cells and the formation of specific antibody, therefore there is no class switching (to antibodies other than IgM) and no germinal centers formed Increased levels of IgM and no IgA, IgG and IgEPatients usually have recurrent bacterial infections and severe diarrhea Treated with monthly gamma globulin injections and antibiotics as needed |
|
|
Hyper IgM and class switching needs |

CD40L on T helper cell |
|
|
Common Variable Immunodeficiency |
Also called “late onset agammaglobulinemia Associated with increased incidence of autoimmunity Occurs in late teens early 20’s Ig levels decrease with ageInadequate T cell:B cell signalling so that B cells can’t differentiate into plasma cellsB cells can be found in the periphery, low Ig levels |
|
|
Transient Hypogammaglobulinemia of infancy |
Also called “early onset agammaglobulinemia” Delayed onset of normal IgG Synthesis usually seen in the 5th to 6th month of life Usually resolves by 2-6 years of agePatients usually have recurrent respiratory infections treatmentantibiotics and gamma globulin replacement |
|
|
Selective IgA Deficiency |
Most common of the Immunodeficiency Diseases (1:800) Genetic component not known In some patients can detect anti-IgA, in others the IgA+ B cells don’t differentiate into plasma cells Patients can be asymptomatic to presenting with an increased incidence of respiratory tract infections, infections at mucosal surfaces Treated with antibiotics as need (NOT IVIG) Pt not making IgA, give Ig-gamma that may have IgA in it, may have anaphalaxis |
|
|
Bruton X-linked hypo- γ globulinemia |
Deficiency of a tyrosine kinase blocks B-cell maturation ↓ Ig all classes, no circulating B cells, pre-B cells in bone marrow normal, normal CMI Monthly γ globulin replacement, antibiotics for infections |
|
|
T Cell Deficiencies |
Because T cells orchestrate the immune response, T cell deficiencies can affect both the humoral and cell mediated responsesMuch more severe than the previously discussed disorders DiGeorge’sBare Lymphocyte SyndromeMHC deficiency |
|
|
DiGeorge’s Syndrome |
Autosomal dominant mutation Absence of a thymus, cardiovascular anomalies and characteristic facial featuresReflects a failure of the 3rd and 4th pharyngeal pouches to develop between weeks 10-12 of gestation (development of aortic arch of heart) , low t cell number, absence of t cell response Recurrent infections with intracelluar pathogens, Candida (Chronic mucocutaneous candidiasis), and viruses Treated with fetal thymic transplants and bone marrow transplants "lack of thymic shadow" IgM is only antibody made |
|
|
Bare Lymphocyte Syndrome |
Autosomal recessive mutation Mutation that prohibits the expression of class II MHC therefore TH cells can’t develop Presentation similar to DiGeorge’s (SCID) Treated with bone marrow transplants There are mutations that effect class I MHC expression which would affect the CD8 TC cells.Recurrent viral infections |
|
|
MHC Class 1 defiency Selective T-cell deficiencies |
failure of TAP1 to transport recurrent viral infections |
|
|
MHC class 2 defieicney- Selective T-cell deficiencies |
Deficient in CD4 cells, no GVHD, ↓ Igs, observed as a SCID
Failure of MHC class II expression, defects in transcription factors |
|
|
SCID-Complete functional T- & B- cell deficiency |
Adenosine deaminase deficiencyOR defect in IL-2 receptor, x linked, chronic squirts, mouth/throat lesions, opportunistic infections, RAG1/RAG2 mutation---> total absence of B/T cells(autosomal recessive) bone transplant/gene therapy |
|
|
Wiscott-Aldrich Syndrome(B&T issue-partial) |

Thrombocytopenia(Bleeding problems, low platelets)eczema, immunodeficiency Complex X-linked disorderMutation in leukosialin (CD43) which is responsible for actin filament assembly and cytoskeletal rearrangement necessary for T cell signalling IgA/E increased,IgM decreased |
|
|
Ataxia-Telangiesctasia(B&T issue-partial) |

Autosomal recessive diseaseMutation in ATM gene IgA and sometimes IgE deficientIgM increased counts, |
|
|
Bright field (light) microscopy
|
Shows most bacteria, not viruses
Parasites and eggs (10-40X) Gram-stain of bacteria (100X ocular) Blood smears (40-100X) ocular is 10X so get lens magnification and multiply by 10 |
|
|
Phase-contrast microscopy |
Shows internal details of microbesCreates 3D image |
|
|
Enriched nonselective media |
Blood, Chocolate agar |
|
|
Selective media |
Thioglycolate broth – anaerobes Sabouraud dextrose agar – fungi MacConkey agar – GNR, lactose-fermentation (differential) |
|
|
Differential media |
Mannitol salt agar – S. aureus Lowenstein-Jensen medium – mycobacteria |
|
|
Specialized media |
Buffered charcoal yeast extract (BCYE) agar - Legionella Thiosulfate citrate bile salts sucrose (TCBS) agar – Vibrios |
|
|
Western Blotting |
Used to identify specific protein in mixture |
|
|
Precipitation |
Soluble proteins become insoluble==Immune complexes |
|
|
Hemagglutination |
RBCs placed on slide and anti-A and anti-B serum used to type Agglutination with A = Type A Agglutination with B = Type B Agglutination with A and B = Type AB No agglutination = Type O |
|
|
Hybridoma |
cancer cell and b cell=clone makes 1 Ab with 1 epitope |
|
|
Enzyme-Linked Immunosorbent Assay (ELISA)
|
Detects Ag or Ab in samples
can tell us antibody levels from pt to pt |
|
|
Flow Cytometry
|
Looking at cell surface expression of proteins
|