![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
18 Cards in this Set
- Front
- Back
|
Clinical signs of a corneal ulcer? |
Hyperaemia of the conjunctiva. Discomfort. Oedema. Neovascularisation. Infiltration of cells. |
|
How do we assess for corneal ulcers? |
Apply proxymetacaine and fluorescein. Look for a cause e.g. an eyelash- ectopic cilia. |
|
|
Causes of corneal ulceration? |
External trauma - centrally located. Hair/lash trauma- ectopic cilia dorsally. Tear film abnormality do a SCC Infection-FeLV. |
|
|
What is contraindicated in an animal with ulceration of the cornea? |
Corticosteroids. |
|
|
How does a superficial ulcer heal?
|
Normal heal with adjacent basal epithelial cells migrating in to replicate to restore full thickness. Only takes a few days. |
|
|
How do deep ulcers heal? |
Fibrin clot then activated keratocytes move in and secrete collagen aided by fibroblasts. New collagen is disorganised and is permenantly opaque. |
|
|
Common causes of exposure keratopathy? |
Prominent globe with poor lid closure- brachycephalics. Facial nerve paralysis. Trigeminal nerve paralysis. |
|
|
How do we go about treating a superficial ulcer? |
Usually heal by themselves but due to severity of if infection established we give topical broad spectrum antibiotics such as chloramphenicol. ARRANGE revisit and treat until fluorscein negative. |
|

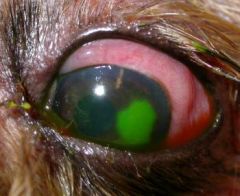
What has occurred here? What is the risk with this? |
Enzymatic degradation down to descemets layer. Deep ulcer and risk of rupturing. |
|

A boxer comes into your practice name an ulcer which this breed is prone to and describe the pathogenesis and how we treat it? |
Superficial chronic corneal epithelial defect. SCCED. Ulcer edges fail to adhere to the stroma creating a flap. Apply topical anaesthetic and swirl a q tip to debride the flaps. Follow up with SGK or SPK. |
|
|
How do we perform SGK? |
25 G needle break the BM in a grid pattern 1-2 mm appart with topical anaesthetic applied. Do not perform this technique on a very oedematous cornea. |
|
|
How do we manage a mid stromal ulcer? |
Topical antibiotics every 2-6 hours. Treat reflex uveitis with atropine to dilate pupil. Give systemic NSAIDs. Topical anticollagenases 3-4 x daily. |
|
|
What do mid stromal ulcers occur secondary to? As a result what must we do?
|
Bacterial infection. Under anaesthetic get a swab around ulcer edge, stain with diff quick to identify if we have rhods or cocci. |
|
|
How do we treat a deep ulcer if referral is impossible for whatever reason? |
Topical fluoroquinolone or fortified cephalosporin apply every 5-30 minutes then every 1-2 hours. Anti colleagenase too. |
|

How do we tell we have a melting ulcer? |
If the ulcer looks gelatinous as though a suture would not hold in it. |
|

How can we treat a melting ulcer? |
Antibiotic therapy with an anti collegenase applied frequently. Collect serum potentially and apply every 1-2 hours until ulcer stops melting. If after 24 hours of this not ceasing to melt emergency surgery is needed by a specialist. |
|
|
An owner phones you after their dog got cleaning liquid in its eye. In the mean time before the dog gets to the practice what advise do you give? On arrival what should we do? |
Advise to flush the eye with thorough rinsing of the cornea, eyelids, conjunctiva with saline. Continue the lavage and pH test until it reachs 7.5 |
|
|
How do we treat a small laceration? |
Topical A/B, atropine, systemic A/B and NSAIDs. |