![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
1237 Cards in this Set
- Front
- Back
|
ASD
|
|
|
|
subclavian steal |
|
|
|
amiodarone
|
|
|
|
ABI
|
|
|
|
Leriche syndrome
|
thigh and butt claudicat w ED
|
|
|
lipid screening
|
|
|
|
no PCI w/in 90 min (of first medical contact, and 12 hrs w/ing symptom onset)
|
|
|
|
IABPs
|
increase coronary artery perfusion
|
|
|
thrombolytics absolute contraindicats
|
|
|
|
adenosine
dypiramidole persantine |
|
|
|
MVP |
|
|
|
valsalva and standing
|
|
|
|
squat and handshake
|
|
|
|
cardiogenic shock
|
tx w inotropes to increase contractility and CO
|
|
|
AS
|
|
|
|
DVT tx
|
hospital, LWMHep, warf 2-3 INR
|
|
|
INR 3-4
|
mechanical valve
|
|
|
tamponade
|
elevates pressures in all chambers
|
|
|
HOCM
|
|
|
|
stress test
|
|
|
|
beta blockers, ACE, and aspirin lower mortality
|
|
|
|
constrictive pericardit
|
|
|
|
restrictive cardiomyopathy
|
|
|
|
verapamil
|
good for rate control, AF tx
|
|
|
stage I HTN
|
|
|
|
mitral stenos
|
|
|
|
valve eval
|
|
|
|
MC intracardiac tumor
|
|
|
|
RV dysfx
|
|
|
|
CHF
|
|
|
|
fibromuscular dysplasia
|
|
|
|
IV nitro
|
|
|
|
AAA dx
|
|
|
|
ACEi vs ARB
|
|
|
|
LDL >100
|
|
|
|
asthma and cocaine or prinzmetal
|
cant give betablocks, give NON HR-increasing
CCBS - verapamil diltiazem |
|
|
L main artery occulsion
|
|
|
|
PCI
|
|
|
|
beta blocks good for
|
preop pts w cardiac risk facts
|
|
|
HTN+hypokalemia (muscle weakness)
|
hyperaldosteronism
|
|
|
HTN+hyperglyc and hypercortisol
|
cushing's
|
|
|
captopril renal scan
|
|
|
|
thiazides for healthy pts
|
|
|
|
Afib in stable pt
|
|
|
|
digox tox seein in
|
|
|
|
mitral regurg
|
|
|
|
MCC of diastolic heart dysfx
|
|
|
|
RCA occlusion
|
|
|
|
decrease mortality in CHF
|
|
|
|
displaced PMI to axilla
|
|
|
|
JVD up on inhalat
|
|
|
|
>10mm decrease in BP on inhalat
|
|
|
|
ST elevat in V2-V4
|
|
|
|
PR interval > 200
|
1st degree block
|
|
|
ST depression in V2-V4
|
|
|
|
check reinfarction with
|
CKMB
|
|
|
door to PCI
door to thromoblysis |
|
|
|
ST depression
|
|
|
|
GpIIa/IIIb
|
|
|
|
VT/Vfib
|
|
|
|
3rd degree AV block
|
|
|
|
tamponade/wall rupture
|
|
|
|
RV infarct
|
|
|
|
Vfib
|
loss of pulse
|
|
|
valve rupture
|
|
|
|
septal rupture
|
|
|
|
ACE decreases CHF mortality by
|
by lowering preload
|
|
|
pulmonary congestion
|
LV fail - backup into lungs
|
|
|
chronic AR can cause CHF
|
L side fail burdens HR = R side fail
|
|
|
RV fail
|
|
|
|
diastolic LV fail
|
|
|
|
systolic LV fail
|
|
|
|
no prophylaxis for acquired valve dz
|
|
|
|
RV infarct
|
|
|
|
LV infarct
|
|
|
|
pulm edema
|
|
|
|
do stress test post MI
|
|
|
|
internal mammary
|
better than saphenous in CABG
|
|
|
constrictive pericardit
|
|
|
|
best test for pheochromo
|
free plasma fractionated metanephrines
|
|
|
best way to lower BP
|
|
|
|
manage stable angina
|
|
|
|
pre HTN
|
|
|
|
high risk pt LDL goal
|
|
|
|
moderate risk pts w 2 risk facts LDL goal
|
|
|
|
low risk pt w 0-1 factors LDL goal
|
|
|
|
prolonged CPR
|
relative contraindicat to thrombolytics
|
|
|
endocardit dx/tx
|
|
|
|
TEE vs TTE
|
|
|
|
nml BNP
and nml wedge |
|
|
|
best initial therapy for acute pulm edema
|
|
|
|
high/low thyroid can cause
|
CHF
|
|
|
dyspnea sudden onset clear lungs
|
PE
|
|
|
dyspnea sudden wheezing, up exp phase
|
asthma
|
|
|
dyspnea slower progress, fever, sputum, unilat ronchi
|
pna
|
|
|
dyspnea decreased unilat breath sounds , trach deviat
|
|
|
|
dysp numbness caffeine anxiety
|
panic attack
|
|
|
dysp gradual pallor
|
anemia
|
|
|
dysp dull percuss at base
|
|
|
|
dysp smoking, barrel chest
|
COPD
|
|
|
dysp palpitats, syncope
|
arrythmia
|
|
|
dysp anesthetic, brown blood, O2 not helping, cyanosis
|
methhemoglobinemia
|
|
|
dysp burning car wood stove suicide
|
CO2 poison
|
|
|
papillary muscle rupture
|
murmur and MR
|
|
|
sinus brady can occur after inferior wall MI
|
|
|
|
synch cardiovert
unsynch |
|
|
|
thallium test
|
if pt cant exercise, has EKG abl/unclear, or is on digox
|
|
|
stress echo
|
use w abl/unclear EKG
|
|
|
valsalva and standing
|
|
|
|
neurocardiogenic
|
|
|
|
somatomedin C
|
|
|
|
pericardit tx
|
|
|
|
beck's traid
|
|
|
|
inhalation
|
|
|
|
regurigitation responds best to
|
|
|
|
stenosis and fibrosis
|
|
|
|
biphasic wave in V1V2
|
|
|
|
handgrip and AS
|
|
|
|
papillary muscle rupture + HTN
|
|
|
|
ACE/ARB best for
|
|
|
|
stenotic lesions need
|
replacement
|
|
|
aortic regurg
|
|
|
|
reflex syncope
|
|
|
|
bradycardia alternating with atrial flutter
|
|
|
|
dilated cardiomyopathy
|
|
|
|
hypertrophic cardiomyopathy
|
|
|
|
all cardiomyopathies
|
|
|
|
S4
|
stiff, noncompliant
|
|
|
mitral stenos unaffected by
|
|
|
|
amyl nitrate
|
|
|
|
restrictive cardiomyopathy
|
can't contract OR relax
|
|
|
pericardit on EKG
|
|
|
|
pulsus paradoxus
|
|
|
|
cilostazol
|
|
|
|
screen every smoker male
|
for AAA at 65
|
|
|
bad heart stuff in preggo
|
|
|
|
variant angina assoc w
|
|
|
|
ST depression
|
unstable plaque partially blocks blood flow
|
|
|
diastolic dysfx
|
|
|
|
avoid beta blocks in
|
|
|
|
ACE survival benefit
|
more for pts w EF < 40
|
|
|
SVT
|
|
|
|
multifocal atrial tachy
|
|
|
|
WPW
|
|
|
|
femoral pseudoaneurysm
|
|
|
|
don't dc amiodarone if
|
txing arrythmia
|
|
|
acute asthma exacebat check
|
|
|
|
stable asthma
|
|
|
|
zariflukast
|
|
|
|
asthma reversibility
|
12% inc of FEV1 w albuterol
|
|
|
asthma tx for mild intermit
|
|
|
|
asthma mild persist
|
|
|
|
asthma moderate persist
|
|
|
|
asthma severe persist
|
|
|
|
cromolyn
|
|
|
|
theophylline
|
|
|
|
anticholinergics
|
|
|
|
COPD/asthma exacerbation
|
|
|
|
respiratory rate and normalization of ABG
|
|
|
|
COPD findings
|
|
|
|
COPD dx/tx
|
|
|
|
COPD bugs
|
|
|
|
ABPAspergill
|
|
|
|
bronchiectasis
|
|
|
|
CF dx/tx
|
|
|
|
gross hemoptysis
|
|
|
|
rapid shallow breathing
|
|
|
|
idiopathic pulm fibrosis
|
|
|
|
p53 and Rb
|
tumor supressors
|
|
|
RAS
telomerase |
|
|
|
malignant cells resist meds with
|
|
|
|
hoarseness
|
|
|
|
benign pulm nodule
|
|
|
|
small cell lung ca synds
|
|
|
|
silicosis increases risk of
|
TB - do annual PPD
|
|
|
leukotrienes vs NSAIDS
|
|
|
|
ARDS
|
|
|
|
PE
|
|
|
|
thoracentesis
|
|
|
|
lung CA tx
|
|
|
|
aldosterone
|
|
|
|
squam cell carci and renal cell carci and breast
|
|
|
|
ventilator pna
|
|
|
|
atypical pna
|
|
|
|
CXR
|
first but not most accurate for ID
|
|
|
empyema
|
|
|
|
exudative pleural effusion
|
|
|
|
transudative pleural effusion
|
|
|
|
PCP dx/tx
|
|
|
|
outpt tx - mild, no abx hx
|
|
|
|
inpt tx
|
|
|
|
CURB65=admit
|
|
|
|
hospital pna = after 48 hrs
|
|
|
|
mc side off of TMPSMX
|
|
|
|
DLCO
|
|
|
|
don't use LMW heaprin with
|
|
|
|
COPD chronic VQ mismatch
|
hypoxic vasoconstriction --> pulm HTN
|
|
|
bilateral hilar LAD
|
|
|
|
pulsus paradoxus in asthma
|
is bad - intubate
|
|
|
tidal vols for COPD, asthma, ARDS
|
|
|
|
langerans cells
|
|
|
|
mesothilioma
|
|
|
|
restrictive pulm dz
|
|
|
|
mcc of brain tumor
|
mets from lung
|
|
|
pulm nodules eval
|
|
|
|
PE eval
|
|
|
|
b agonists like albuterol worsen
|
tachycardia
|
|
|
most accurate TB dx
|
pleural biopsy
|
|
|
positive PPD
|
|
|
|
pulmonary fibrosis
|
|
|
|
interstitial dz dx
|
|
|
|
most likely to respond to steroids
|
|
|
|
decreases mortality in ARDS
|
|
|
|
hypoxia dt damaged parenchyma in COPD or pulm fibros
|
|
|
|
hypoxia dt high altitude
|
|
|
|
hypoxia dt shunt
|
|
|
|
hypoxia dt VQ mismatch
|
|
|
|
AMS, petichiae, refractory hypoxemia
|
fat embolus
|
|
|
sitting
|
|
|
|
tension pneumo
|
|
|
|
oral prednisone
|
|
|
|
sarcoid dx
|
most accurate - lymph node biopsy
|
|
|
PE eval
|
|
|
|
PE tx
|
|
|
|
hypoxemia = vasoconstriction -->
|
|
|
|
allergic rhinit refract to meds
|
10 day oral steroids
|
|
|
best prognostic factor for COPD
|
|
|
|
pancoast tumor
|
|
|
|
bloody pleural effusion
|
|
|
|
pulm lesions with doubling times in under 30 days
|
|
|
|
primary pulm HTN tx
|
|
|
|
bronchopulm dysplasia in kids
|
|
|
|
mc cyanotic heart defect after infancy
|
|
|
|
3 holosyst murmurs
|
|
|
|
transposition of great vessels
|
|
|
|
pulsus alternans
|
LV systolic dysfx
|
|
|
pulsus bigeminus
|
HOCM
|
|
|
pulsus bisferiens
|
aort regurg - double pulse dt blood backflow
|
|
|
puslsus parvus et tardus
|
aort stenos
|
|
|
pulsus paradoxus
|
|
|
|
hypoplastic left heart
|
|
|
|
truncus arteriosus
|
|
|
|
total anomalous pulm ven return
|
|
|
|
mc congenital heart lesion
|
|
|
|
ASD
|
|
|
|
PDA
|
|
|
|
tricuspid and pulmonary lesions radiate to
|
back
|
|
|
aortic lesions radiate to
|
neck
|
|
|
long QT syndrome
|
|
|
|
coarctation of aorta
|
|
|
|
marfan presents w AR murmur
|
|
|
|
immobilization causes
|
|
|
|
DKA
|
|
|
|
health for DM
|
|
|
|
gastroparesis
|
|
|
|
diabet neuropathy
|
pregabalin/gabapentin, TCA
|
|
|
primary adrenal insuffic
|
|
|
|
trousseau synd
|
|
|
|
cushing ups DVT risk
|
INC factor VIII and vonWF, DEC fibronolysis
|
|
|
low morning cortisol and high ACTH
|
|
|
|
MC CAH
|
|
|
|
autoimmune hyperthyroid
|
|
|
|
benign adrenal nodule
|
|
|
|
Barter synd
|
|
|
|
Grave's scan will show
|
|
|
|
metformin
|
|
|
|
DM dx
|
|
|
|
exercising muscle
|
doesn't need insulin
|
|
|
sulfonylurea
|
|
|
|
gliptins
|
up insulin, down glucagon
|
|
|
glitazone/thizolidenidone
|
not in CHF - fluid overload
|
|
|
nateglinide repaglinide
|
like sulfonylurea minus the sulfa
|
|
|
incretins - exenatide
|
|
|
|
alpha glucosidase inhibitors - acarbose/miglitol
|
|
|
|
amylin pramlintide
|
lowers gestric emptying to decrease appetite
|
|
|
long acting oral antiglyc
|
glargine more stable than NPH, add insulin if uncontrolled with orals
|
|
|
short acting oral antiglyc
|
lispro, aspart - take before meals
|
|
|
PTH-like peptide
|
|
|
|
1st line cushing's test
|
|
|
|
cushing SYND ectopic hyper cortisol
|
|
|
|
cushing DZ
|
|
|
|
weight gain and osteoporosis in cushing's
|
|
|
|
in the morning cortisol increases
|
|
|
|
Addison's
|
|
|
|
cosyntropin test
|
|
|
|
adrenal fail
|
rise of ACTH due to lack of feedback inhibition
|
|
|
Conn's
|
|
|
|
pheo
|
|
|
|
low calcium
|
|
|
|
alk phos found in
|
bone
liver GI placenta if up, check GGT - if up - liver US |
|
|
adrenal insufficiency
|
|
|
|
prolactin cosecreted with GH
|
|
|
|
squam vs small cell carci hormones
|
squam - ups Ca via PTHrP
small cell - ectopic ACTH (cushing) |
|
|
facticious insulin
|
|
|
|
insulinoma
|
|
|
|
carcinoid synd
|
|
|
|
give to hyperthyroid pts even before scan
|
beta blocks
|
|
|
adrenal nodule
|
|
|
|
primary hypothyroidism can cause
|
|
|
|
glucagonoma
|
|
|
|
primary polydipsia
|
|
|
|
hot nodule
|
|
|
|
seminoma
|
|
|
|
lyedig
|
|
|
|
symptomatic hypercalcemis
|
|
|
|
tangier dz
|
|
|
|
unique to graves hyperthyroid
|
|
|
|
hyperCA
|
|
|
|
sarcoid granuloma tx
|
prednisone
|
|
|
hyperthyroid tx
|
|
|
|
radiactive iodine uptake before FNA
|
for cold, malignant nodule
|
|
|
solitary nodule
|
|
|
|
euthyroid sick syndrome
|
nml or up TSH
low T3 T4 |
|
|
water deprivations test tells apart
|
|
|
|
nephro vs central DI
|
|
|
|
poor healing diabetic ulcers
|
|
|
|
vit D defic
|
|
|
|
hypercalc
|
|
|
|
MEN1
|
|
|
|
MENIIa
|
|
|
|
MENIIb
|
|
|
|
hypovolemia
|
|
|
|
DM assoc w celiac
|
screen w tissue transglutaminase Iga abs
|
|
|
metabolic sydrome
|
|
|
|
pit adenoma
|
|
|
|
congentical hypothyroid dt
|
thyroid dysgenesis
|
|
|
adrenoleukodystrophy
|
|
|
|
21 hydroxy CAH
|
|
|
|
diGeorge dx
|
PCR of 22q11 to confirm
|
|
|
LH and FSH in turners
|
UP
|
|
|
moms of potential CAH kids
|
|
|
|
SCID
|
|
|
|
acuye laryngotracheobronchit
|
|
|
|
if can't comply w oral abx for strep
|
can do penicill G IM
|
|
|
asthma dx in kids
|
clinical
|
|
|
congenital diaphragmatic hernia
|
|
|
|
apnea of prematurity
|
|
|
|
what to do to hypoactive infant
|
dry and warm to stimulate, then check HR and breathing
|
|
|
MC pneum in kids
|
|
|
|
choanal atresia dx
|
|
|
|
insp striod W/O cough
|
laryngomalacia
|
|
|
common variable immunodefic
|
|
|
|
bruton's X agammaglob
|
|
|
|
first reflexes to disappear in babies
|
rooting and palmar grasp
|
|
|
truncus arteriosus
|
|
|
|
transposit of great vessels
|
|
|
|
JONES
|
joints carditis subcut nodules erythema MARGINATUM sydeham chorea
|
|
|
tetralogy of fallot
|
|
|
|
ebstein anomaly
|
|
|
|
erythema marginatum
|
erythematous serpiginous macular lesions w pale centers, nonpruritic, trunk and limbs
|
|
|
confirm recent strep
|
|
|
|
innocent murmur
|
soft (mid)systolic vibratory 2/6 age 3-7
|
|
|
VSD
|
|
|
|
congenital long QT and deafness and arrythmias
|
Jervell lang nielsen synd
|
|
|
hypoplastic left hear
|
|
|
|
TAPVR
|
|
|
|
kawasaki
|
|
|
|
coxakie
|
|
|
|
coarctation rib notching
|
posterior
|
|
|
MCC of HTN in kids
|
renovasc
|
|
|
aort stenos in kids
|
|
|
|
hypoplastic left ventricle
|
|
|
|
painless serosangionous breast dicharge with no mass or tumor cells
|
intraductal papilloma
|
|
|
anti histone autoabs
|
|
|
|
congenital toxo
|
|
|
|
congenital CMV (HHSV5)
|
|
|
|
congenital rubella
|
|
|
|
mc child leukemia
|
ALL
Bcells |
|
|
meningit bugs
|
|
|
|
calcium gluconate
|
|
|
|
post circ bleeding
|
|
|
|
dorsal column (posterior)
|
vibration, proprioception, and touch localization
|
|
|
transferance is what patient places onto you
|
countertrasferance is what therapist feels from patient
|
|
|
EPS management
|
|
|
|
P value BELOW .05
|
|
|
|
case control study
|
identifies ppl w dz and compares to comparable group without dz
|
|
|
cohort vs restrospective cohort
|
|
|
|
CLL
|
B cell disease
thrombocyto bad prognosis 8-10 survival years smudge cells = fragile, partially disintegrade CD20 cell surface antigen |
|
|
intestinal lymphom
|
|
|
|
whipple dz
|
|
|
|
dx acoustic neuroma
|
MRI w gadolinium
|
|
|
pyloric stenosis imaging
|
abd US
|
|
|
neonate w bilious vomiting
|
|
|
|
dilated loops of bowel
|
|
|
|
pseudodementia
|
|
|
|
CP
|
|
|
|
optic glioma
|
|
|
|
pigment retinitis
|
bilateral vision loss
|
|
|
retinal hamartoma
|
found in tuberous sclerosis
|
|
|
acute limb ichcemia
|
|
|
|
validity/accuracy
|
how well a test measures what it is supposed to measure - as compared gold standard
|
|
|
reliability
|
similar results on repeat measurements
|
|
|
interstitial cystitis
|
|
|
|
cross-section study
|
exposure and outcome measured simultanously, not seperated by time period
|
|
|
diarrhea in HIV
|
|
|
|
SIADH tx
|
|
|
|
neonatal chlamidial conjunctivit
|
|
|
|
nosocomial UTI
|
enterococci - can cause endocardit
|
|
|
transient monocular vision loss
|
|
|
|
aldost/renin ratio over 20
|
|
|
|
raising cutoff level for diagnostic test
|
|
|
|
precision
|
|
|
|
thymoma
|
|
|
|
hazard ratio
|
|
|
|
mesenteric angio
|
|
|
|
live attentuated vaccines
|
|
|
|
arm drop
|
|
|
|
PPV and NPV
|
|
|
|
seminoma
|
elevated betaHCG, NORMAL AFP
|
|
|
anterior mediastinal mass
|
|
|
|
pyoderma gangrenosum
|
|
|
|
seizure not contraindication for
|
vaccination. but anaphylaxis and neuro/encephalopathy
|
|
|
rheumatic fever
|
give penicillin to prevent reoccurence and limit progression of rheumatic heart dz
|
|
|
posterior urethral valves
|
|
|
|
basal cell carci
|
|
|
|
bilirubin in urine
|
|
|
|
PACs benign but
|
smoking and alcohol are reversible risk factors
|
|
|
circulating lymphocytes reduced in
|
|
|
|
splenectomy causes defects in
|
|
|
|
actinic/solar keratosis tx
|
fluorouracil cream
|
|
|
PNH and acute intermit porphyria
|
|
|
|
schistocytes
|
|
|
|
cerebral septic emboli
|
|
|
|
signs of increased cardiac filling pressures
|
|
|
|
cryoprecipitate |
|
|
|
endometrial hyperplasia
|
|
|
|
lithium therapy
|
long term if 2 manic episodes, lifetime if more
|
|
|
cushing reflex
|
|
|
|
5% dextrose
|
|
|
|
diabetic retinopathy |
|
|
|
closed angle glaucoma
|
|
|
|
orbital cellulitis
|
|
|
|
prerenal failure
|
|
|
|
nonselective beta blockers and aspirin promote
|
|
|
|
intramembranous deposits staining for C3 with nephrotic proteinuria
|
|
|
|
BPH evaluation
|
|
|
|
osteomalacia
|
|
|
|
clavicular fracture
|
require neurovasc exam to r/o brachail plexus or subclavian artery injury
|
|
|
immune complex mediated kidney damage
|
|
|
|
acetaminophen tox |
HAV, HBV, HPV age9-26, Influ annually, meningococc 11-18, PCV13 once, PPSV23 8 wks later EVERY 5, Tdap once, repeat Tdap for preggos, Td every 10 years following
|
|
|
dipyridamole
|
in myocard perfusion scans reveals areas of lower perfusion - redistribution of coronary flow to non-diseased areas = coronary steal
|
|
|
bernard soulier |
cardiac tamponade - nml cardiac silouette on CXR
|
|
|
tinea corporis
|
|
|
|
postviral sinovitis
|
ship pain resolves in a week post URI or rubella vaccine
|
|
|
rubella
|
|
|
|
measles
|
|
|
|
parvo B19
|
|
|
|
roseola infantum
|
|
|
|
infant chlamidya
|
|
|
|
staph scalded skin
|
|
|
|
preggos w listeria
|
|
|
|
brain abscess in meningit
|
|
|
|
entameba histolytica
|
|
|
|
clostridium botulinim and tetani and listeria char
|
gram + rod
|
|
|
ecoli and h influ char
|
|
|
|
s agalacticae
|
|
|
|
impetigo
|
|
|
|
nisseria char
|
|
|
|
cat bite tx
|
amox clavulan for p multocida and s aureus
|
|
|
CFbest for osteomyelit dx
|
MRI - if have metal - nuclear triphasic scan
|
|
|
gonorrhea
|
|
|
|
s aureus pnemonia
|
|
|
|
zoster
|
|
|
|
herpes encephalit
|
|
|
|
bacterial meningit CSF
|
|
|
|
TB meningit CSF
|
|
|
|
cryptococc lyme rickettsia CSF
|
|
|
|
thick walled cavitary lesion
|
|
|
|
white plaques in mouth in HIV
|
|
|
|
immunocompetent pt w ring enhancing lesion
|
|
|
|
zidovudine
|
|
|
|
needlestick HIV
|
|
|
|
peritonsillar abscess
|
|
|
|
nml iron |
stridor and drool
|
|
|
COPD exacerbat bugs
|
spneum and mor catarell - tx w amox/clavu
|
|
|
glanzman thrombastenia |
botulism has papillary dilation
|
|
|
empiric meningit tx
|
|
|
|
complicated pyelo
|
hosp + IV genta, ceftriax, fluoroquinolone
|
|
|
gram pos cocci in clusters
|
staph
|
|
|
gram pos diplococci
|
gonorrhea
|
|
|
bell's palsy occurs post
|
|
|
|
tinea capitis
|
|
|
|
atropic gastritis |
|
|
|
red eyes in neonate
|
|
|
|
transient polysythemia and spelomegaly in newborn
|
|
|
|
microcephaly, short palpebral fissures, maxillary hypoplasia, micrognathia, thin upper lip
|
etoh baby
|
|
|
hydrocephalus, microcephaly, CNS defect
|
retinoic acid baby
|
|
|
narrow bifrontal diamater, high forhead, epicantal folds, low nasal bridge, midfacial hypoplasia, small mouth w long philtrum, cleft lip and meningomyelocele
|
valproate baby
|
|
|
glycogen storage dz type 2 |
opiate - respi distress in newborn
|
|
|
low birth weight, hypogonadism, almond eyes, hypotonia
|
prader willi - FISH: 15q11-13
|
|
|
adams test
|
forward bend to easy test for scoliosis, but gold standard is XRay
|
|
|
mc complicat of very low birth weight baby
|
intracranial hemorrage
|
|
|
legg calve perthes
|
|
|
|
fair blond blue babay w vomit, photosensitivity, rash
|
PKU, also musty smell
|
|
|
newborn skull fract |
depressed=surgery, linear =mc, basilar=fatal
|
|
|
capUt saccUdaneum
|
crosses sUtUre lines, but cephalohematoma does not
|
|
|
brachial plexus injury - dystocia, erb, klumpke
|
|
|
|
WAGR
|
|
|
|
bartter synd
|
|
|
|
mom DM can cause in baby
|
|
|
|
cyanosis w feeding
|
|
|
|
worst complication of juvenile RA
|
|
|
|
osgood schlatter
|
|
|
|
poorly formed bulky stools w low weight gain
|
|
|
|
VEAL CHOP fetal tracings
|
|
|
|
varicella vaccine done at
|
12-15 months
|
|
|
duchenne musc dyst
|
|
|
|
air fluid levels on CXR
|
diaphragmatic hernia - bowels in thorax
|
|
|
omphalocele vs gastroschisis
|
|
|
|
umbilical hernia assoc w
|
hypothyroid, weak rectus muscle should close by itself by 3yo
|
|
|
anticholinergics |
|
|
|
mcc of increased AFP
|
|
|
|
kids exposed to TB
|
get isoniazid regardless of PPD results
|
|
|
if replace folate in b12 defic |
cocaine baby
|
|
|
sisters of fragile x boys
|
evaluate genetically as heterozygotes can present w ADHD
|
|
|
hydroceph, poor feed, irritable, down activitiy, tense fontanelle, distended scalp veins, sunset eyes
|
germinal matrix hemorragea
|
|
|
atopic dermatit
|
|
|
|
nevus sebaceus
|
congenital hamartoma on scalp surrounded by alopecia - small well demarcated oval yellow orange raised plaque
|
|
|
herpetic whitlow
|
|
|
|
osteoid osteoma
|
|
|
|
hydroxyurea |
painful mass w bone destruction and periosteal elevation
|
|
|
ewing's
|
malig bone tumor from medullary tissue of cylindrical bones - pain fever leukocytos w onion skinning
|
|
|
CF
|
|
|
|
Her2/neu |
post viral encephalopathy w high ammonia levels
|
|
|
gaucher
|
|
|
|
hunter synd
|
x linked mucorpolysacc w coarse facial features and bone abl. lysosomal hydrolase deficiency
|
|
|
chalazion
|
|
|
|
hordeolum
|
|
|
|
dacrocystitis
|
|
|
|
forceful torsion of knee with foot planted and popping with sever pain
|
|
|
|
low calcium and PTH w high phosphate
|
hypoparathyroid
|
|
|
diabetic kidney
|
microangiopathy and glomerulosclerosis
|
|
|
sodium bicarb |
|
|
|
fever and sore throat with antithyroid drugs
|
|
|
|
antimitochond abs |
testost ovarian, DHEAS adrenal
|
|
|
wallenberg synd
|
|
|
|
fever w leukopenia and throbocytopenia and elevated LFTS
|
ehrlichiosis - tx w doxy - rash uncommon
|
|
|
f
|
f
|
|
|
adenomyosis
|
|
|
|
prosthetic join infection
|
|
|
|
irritable, high pitch cry, poor sleep and feed, tremor/seizures, sweating, sneezing, tachypnia, vomit/diarrhea in neonate
|
heroin baby
|
|
|
kallman synd
|
|
|
|
tremor at rest that improves w activity
|
|
|
|
elevation of semidiaphragm on CXR |
volume more important than insulin
|
|
|
bradycardia, hypotens, wheezing, hypoglyc, delirium, seizures, cardiogenic shock
|
|
|
|
comedonal acne tx
|
topical retinoids and benzoyl peroxide
|
|
|
nitroprusside toxicity
|
|
|
|
hypersensitivities 1-4
|
|
|
|
paget dz = osteitits deformans
|
|
|
|
proteinuria in kids
|
often transient - repeat urine dipstick
|
|
|
citrate
|
|
|
|
chi square
|
compares proportions of a 2x2 table
|
|
|
PSVT
|
|
|
|
pregnancy screening for all
|
|
|
|
2 months
|
|
|
|
4 months
|
|
|
|
6 months
|
|
|
|
9 months
|
|
|
|
12 months |
|
|
|
increase in cortisol with cosyntropin
|
rules out primary adrenocort insuffic = addison's
|
|
|
trachoma
|
follicular conjunctivitis and pannus (neovascularization)
|
|
|
septic shock
|
|
|
|
primary amennorhea with uterus eval
|
|
|
|
amehorrhea w no uterus
|
|
|
|
number needed to treat
|
|
|
|
Right axis deviation
|
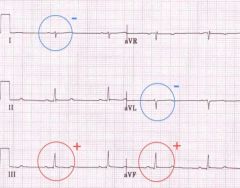
leads III and aVF are positive; leads I and aVL are negative
|
|
|
glycogen storage dz type I |
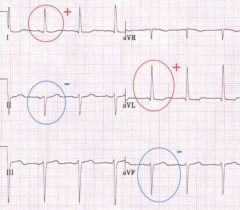
leads i and avl are positive; leads ii and avf are negative
|
|
|
bipolar I does not require |
an episode of deperession for dx |
|
|
edward's synd |
|
|
|
stress incontinence tx |
|
|
|
syphilis dx |
|
|
|
postinfectious GN |
|
|
|
IgA nephropathy |
|
|
|
complete AV canal defect |
|
|
|
round blue inclusions of RBCs on wright stain |
howel jolly bodies assoc w hypo/asplenism |
|
|
langherhan's cells histiocytosis |
solitary painful lytic bone lesion w overlying swelling and hypercalcemia in kid |
|
|
3yrs |
|
|
|
4yrs |
|
|
|
HIV pt w ICP |
|
|
|
3yrs |
|
|
|
4yrs |
|
|
|
amiloride |
|
|
|
syphilis tx if can't penicill |
doxy |
|
|
mc injured nerve assoc w midshaft humerus fracture |
radial nerve |
|
|
IUP seen on US if bHCG at |
1500-2000, if level below, repeat in few days |
|
|
clear cell adenocarci vs squamous cell carci of vag and cervix |
|
|
|
down hematocrit = |
|
|
|
CHF effect on kidney |
vasoconstriction of efferent arterioles = up intraglomerular pressure to maintain GFR |
|
|
warfarin inhibits |
sythesis of vit K = 2,7,9,10,C,S |
|
|
diamond blackfan |
|
|
|
fanconi's anemia |
|
|
|
plantar warts |
|
|
|
mysathenia tx |
|
|
|
hashimoto abs |
|
|
|
severe abdominal pain worsening w food leading to avoidance of food |
early activation of adrenal gland (peripheral) |
|
|
mc nutritional defic in kids |
|
|
|
sinusoidal congestion w hemorragic necrosis of liver |
hepatopathy of CHF |
|
|
reye synd |
|
|
|
abort cluster headache |
|
|
|
best way to reduce diabetic nephropathy |
BP control |
|
|
abl secretin |
folate - homocysteine, b12 - MMA |
|
|
abort cluster headache |
NPV, varies w pretest probability of dz. Pt w high probability of dz whill have low NPV |
|
|
alcoholic electolytes |
|
|
|
antiparietal abs |
|
|
|
ABO mismatch vs IfA anaphylax |
|
|
|
dysphagia w solids and liquids together |
100% oxygen |
|
|
thyroid changes in preggos |
increased thyroid hormone w increased total T3 and T4 and DOWN TSH |
|
|
lupus anticoagulant |
|
|
|
high iron |
100% oxygen |
|
|
dead space |
wasted ventilation of poorly perfused areas = PE. no hypoxemia |
|
|
CD4 below 200 |
|
|
|
CAH vs aromatase defic |
CAh hass estrogen, aromatase defic doesn't. Virilization of females w normal internal but abl external genitals |
|
|
metoclopramide |
|
|
|
consolidation vs pleural effusion |
vivid dreams |
|
|
methanol poison |
|
|
|
guillan barre |
|
|
|
poly and dermatomyosistis dx/tx |
|
|
|
anticholinergic poisoning |
|
|
|
dx of diverticulitis |
abd CT |
|
|
pneumopariutoneum |
|
|
|
beta blockers or CCB tox |
hydralazine for emergencies methyldopa for long term in HTN preggos |
|
|
mobile cavitary mass in the lung |
aspergilooma - presents w hemoptysis |
|
|
alcoholic hepatitis |
ast twice ALT and ferretin and GGT UP |
|
|
hydro vs varicocele |
|
|
|
hypospadias vs epispadias |
|
|
|
anuria in neonate 24 hrs |
|
|
|
chronic otitis media over 3 months |
|
|
|
bullous impetigo |
toxin B desmoglein1 |
|
|
ITP in kids |
|
|
|
beta thalassemia |
|
|
|
infant weight |
|
|
|
when trasfuse w RBCs |
if hypotensive or organ dysfx |
|
|
mc heart problem in babies w DM mom |
|
|
|
GAS strep pyogenes |
|
|
|
painful red eye with blurred vision photophobia and tearing |
|
|
|
unilateral eye redness with purulent discharge |
|
|
|
meckel's diverticulitis |
|
|
|
HSP |
|
|
|
clinodactly (deflected pinky) + enlarged tongue |
trisomy 21 |
|
|
6 months vaccinats |
HBV, DTap#3, IPV#3, PCV#3 |
|
|
abacavir |
|
|
|
corneal ulcer |
|
|
|
dacryostenosis |
lactic acidos, hepatit, hypersens rxn |
|
|
abacavir |
inc indirect bili |
|
|
fitzhugh curtis |
adhesion btw liver capsule and diaphragm in PID |
|
|
choking/drooling at feeding |
lactic acidos, hepatit, hypersens rxn |
|
|
pancreatit |
can have nml amylase levels |
|
|
DM babies |
|
|
|
infantile hemangioma |
benign vascular tumor - spontaneous involution, asympt but assoc w CHF dt inc vascular flow |
|
|
duodenal atresia |
can be seen on prenatal US = scaphid abdomen and epigast fullness |
|
|
ulcerative colitis marker |
|
|
|
congenital cataract |
lens opacity dt rubella or galactosemia |
|
|
free air on lateral decubitus baby |
replaces fibrinogen |
|
|
optic glioma and osseous lesions |
NF - sphenoid dysplasia or thinning of long bone cortex |
|
|
neovascularization of choroidal vessels |
|
|
|
wbautoantibodies in DM1 |
|
|
|
|
|
|
|
rrdx of hirschprung |
first anal manometry, then biopsy |
|
|
crohn's |
|
|
|
ulcerative colitis |
|
|
|
punctuate hemorrages on strawberry cervix |
|
|
|
corneal abrasion |
|
|
|
allopurinol safe in renal fail but |
|
|
|
pesudogout |
|
|
|
DJD osteoarthritis |
|
|
|
gout |
|
|
|
RA |
|
|
|
septic arthrit |
|
|
|
epidural abscess |
|
|
|
negative straight leg excludes |
|
|
|
cord compression |
cancer, vertebral tenderness, sensory level, hyperreflexia
|
|
|
cauda equina |
bowel/bladder incont, ED, bilat leg weak, saddle anesth |
|
|
ankylosing spondylitis |
|
|
|
disk herniation |
pain/numb in calf or foot, down knee/ankle reflex and positive straight leg raise |
|
|
spinal stenosis |
|
|
|
dilated retinal veins, microaneurysms, retinal hemorrage, edema, hard exudate |
non-proliferative diabetic retinopathy |
|
|
loefingen |
|
|
|
calcium hyydroxyapatite |
DJD/osteoarthrit + hyperparathyroid |
|
|
bisphosphonate mech |
inhibit osteoclasts |
|
|
painful/tingly butt |
piriformis syndrome - worse w sitting |
|
|
popping at time of injury |
ACL - hyperextended knee |
|
|
wegener |
|
|
|
churg strauss |
|
|
|
anticentromere |
CREST |
|
|
gray vesicles/ulcers on posterior oropharynx |
RA |
|
|
dermatomyositis |
|
|
|
polymiositis |
|
|
|
soft tissue sarcoma (fibrosarcoma) |
under 5 cm - resect, over 5 cm - radiation then resect |
|
|
hordeolum vs chalazion |
|
|
|
retinal artery occlusion |
|
|
|
retinal vein occlusion |
|
|
|
retinal detachment |
|
|
|
Caplan |
RA+ pneumoconiosis _ lung nodule |
|
|
young pt w high spiking fever and rash |
|
|
|
IgG IgM antibods against neg phospholipids |
|
|
|
cyclosporine |
|
|
|
osteoporos |
|
|
|
polycythemia vera |
|
|
|
multiple myeloma |
|
|
|
reactive arthritis |
|
|
|
CREST |
|
|
|
triptans should not be given with |
|
|
|
anticholinergics tox |
|
|
|
de quevrain's tenosenovitis |
|
|
|
relapsing polychondritis |
|
|
|
hematuria + hemoptysis |
|
|
|
antimitochond abs |
|
|
|
antiparietal abs |
pernicious anemia (which doubles gastric cancer risk) |
|
|
anti smooth musc |
autoimmune hepatitis |
|
|
Sjorgen |
|
|
|
tennis elbow |
lateral epicondiliytis - extensor carpi radialis brevis |
|
|
stoke in young pt |
|
|
|
pencil in cup, nail pitting, sausage finger |
psoriatic arthrit. neg RF |
|
|
charcot joint |
|
|
|
silver wiring and AV nicking on retina |
HTN retinopathy. cotton wool spots and flame hemorrages also possible |
|
|
tumor lysis |
|
|
|
CT of intersitial lung dz |
|
|
|
colchicine |
|
|
|
quad screen |
|
|
|
JRA |
|
|
|
atrial tachycardia w AV block |
digitalis toxicity |
|
|
JRA |
|
|
|
5 alpha reductase defic |
|
|
|
vasa previa |
|
|
|
low set ears, micrognathia, cleft palate, no thymus, tuncus arteriosus |
|
|
|
normocytic anemia |
|
|
|
CLL
|
|
|
|
isoniazid hepatotox |
cryptococcal menengit - look for antigen in serum or CSF or yeast on ink stain of CSF, CD4 below 100 |
|
|
fatigue dyspnea anemia w reticulocytosis |
|
|
|
babesiosis |
|
|
|
PE pressures |
|
|
|
mg sulfate |
|
|
|
absent bowel sounds w gaseous distention |
|
|
|
inflammatory breast CA |
|
|
|
TTP |
inability to take oral meds dt nausea/vomit |
|
|
ropinirole
|
|
|
|
selegiline |
MAOB inhbitor for parkinsos - causes confusion and insomnia |
|
|
obesity and bones |
adipose tisuue stores estrogen and causes extra weight bearing so actually prevents osteoporosis, but is associated w osteoarthritis |
|
|
osteoporosis risks |
age, thin body, smoking, etoh, corticosteroids, menopause, hyperthyroid, malnutrition, fam hx, asian and cauc
|
|
|
tx for lyme dz when can't use doxy (preggos, lactating, kids) |
amoxicillin |
|
|
constitutional growth delay |
delayed growth spurt, puberty, and bone age |
|
|
normal jugular venous pressure |
less than 3 cm above sternal angle |
|
|
cyclophosphamide |
prevents sicle recurrence by upping HbF |
|
|
cisplatin and carboplatin |
|
|
|
ethambutol and hydroxychloroquine side eff |
optic neuritis |
|
|
peripheral neuropathy caused by |
phenytoin, isoniazid, vincristine, heavy metals, etoh |
|
|
paroxysmal nocturnal hemoglobinuria vs acute intermit prophyria |
|
|
|
giant cell tumor of bone |
|
|
|
osteitis fibrosa cystica |
|
|
|
glycogen storage dz type I |
|
|
|
glycogen storage dz type 2 |
|
|
|
glycogen storage dz type 3 |
|
|
|
HIV pt w ICP |
cryptococcal menengit - look for antigen in serum or CSF or yeast on ink stain of CSF, CD4 below 100 |
|
|
severe abdominal pain worsening w food leading to avoidance of food |
|
|
|
Her2/neu |
|
|
|
HCG up in all testic cancers, alphafetoprot only in |
|
|
|
ASCUS |
|
|
|
normocytic anemia |
acute blood loss or hemolysis |
|
|
FFP |
|
|
|
cryoprecipitate |
replaces fibrinogen |
|
|
low ferretin |
|
|
|
high iron |
|
|
|
nml iron |
|
|
|
anemia of chron dz |
bleeding only (plt fx and #) |
|
|
if replace folate in b12 defic |
|
|
|
down hematocrit = |
up LDH, indi bili, reticulocytes |
|
|
CLL
|
|
|
|
anemia of chron dz |
|
|
|
hemophilia |
|
|
|
aspirin affects |
bleeding only (plt fx and #) |
|
|
bernard soulier |
|
|
|
glanzman thrombastenia |
|
|
|
tumor lysis |
|
|
|
atrophic gastritis type A |
|
|
|
abl secretin |
|
|
|
what is up in folate and b12 defic |
folate - homocysteine, b12 - MMA |
|
|
polycythemia vera |
|
|
|
TTP |
|
|
|
hydroxyurea |
prevents sicle recurrence by upping HbF |
|
|
parvovirus b19 in sickle cell |
|
|
|
down MCV, up MCHC, negative coombs |
|
|
|
spherocytes also seen in |
|
|
|
quadruple screen - betaHCG, inhibinA, estriol, AFprotein |
|
|
|
flail chest |
|
|
|
elevation of semidiaphragm on CXR |
|
|
|
organophosphate poinsoning |
|
|
|
TCA overdose |
|
|
|
acetaminophen tox |
|
|
|
anticholinergics tox |
|
|
|
beta blockers or CCB tox |
|
|
|
cyanide poison |
|
|
|
isopropyl alcohol posion |
|
|
|
methanol poison |
|
|
|
ethelyne glycol (antifreeze) poison |
|
|
|
salicylate poison |
|
|
|
gray vesicles/ulcers on posterior oropharynx |
herpangina from cocksackie A virus - supportive tx |
|
|
randomization controls |
confounders |
|
|
dx of zenker's diverticulum |
|
|
|
kids fall on outstretched hand |
entrapment of brachial artery and median nervevolkman's contracture = ischemia and infarction from compartment syndrome (rare) |
|
|
subarachnoid bleed delayed morbidity |
vasospasm leading to infarction - can be prevented with nimodipine |
|
|
viral conjunctivitis |
warm/cold compresses. adenovirus |
|
|
gastrinoma |
|
|
|
VIPoma |
|
|
|
normal amniotic fluid index |
5-25 |
|
|
hypoalbuminemia also shows up with |
|
|
|
barrett's and GERD assoc w |
|
|
|
pneumonitis and colitits |
|
|
|
viridans tx |
|
|
|
steroids and splenectomy for |
warm igG AIHA |
|
|
HUS and TTP |
|
|
|
anagrelide/hydroxyurea |
for essential thrombocythemia/polycythemia |
|
|
myelofibrosis |
|
|
|
MALT lymphoma |
|
|
|
CML |
|
|
|
familial melanoma gene |
CDKN2A - also ups risk of panc cancer |
|
|
platelet bleeding |
|
|
|
factor bleeding |
|
|
|
up PT/INR (extrinsic) |
|
|
|
up PTT |
inactivated factors iia, 9a, 11a, 12a (heparin) |
|
|
only 2 factors not made by liver |
vWF and VIII |
|
|
von williebrand |
|
|
|
AML |
|
|
|
IgA heavy chain dz |
|
|
|
leukemoid rx |
leukocytosis over 55k in resoinse to infexn/trauma, also elevates leuk alk phos |
|
|
NSAIDs decrease and increase |
down platelet thromboxane 2 and up bleed time |
|
|
ITP |
|
|
|
myelodysplastic synd |
|
|
|
cladribine pentostatin |
|
|
|
hyper IgM |
|
|
|
monoclonal spike IgG |
most specific finding of multiple myeloma (sometimes IgA) |
|
|
monoclonal spike IgM |
|
|
|
phototoxicity in sun exposed areas |
doxy, thisazies, sulfa, fluoroquinolones, NSAIDS = keratinocyte necrosis in UV |
|
|
cisplatin |
ren fail and deaf |
|
|
bleomycin and busulfan
|
|
|
|
cytarabine |
eye problems - prevent w topical steroids |
|
|
NHL |
|
|
|
hodgkin's lymphoma |
|
|
|
radiation ups risk of solid tumor |
breast lung thyroid |
|
|
keloids can be tender and pruritic |
tx w intralesional steroids |
|
|
plummer vinson |
|
|
|
ALL |
|
|
|
thyroid meds |
propilthyuracil and methimazole - cause agranulocytosis |
|
|
no tx for afebrile neurtopenia |
common after chemo, but if fever - tx w cefepime and carbapenem |
|
|
INR for mitral vlave replace |
2.5-3.5 |
|
|
aplastic anemia |
|
|
|
splenectomy vaccination |
n mening, h influ, pneumococc |
|
|
factor V leiden |
hypercoag/throbophilia. warf 2-3 INR 6mo |
|
|
bugs in sickle cell |
|
|
|
cardiogenic shock |
|
|
|
lmanomentry for |
achalasia, spasm, scleroderma |
|
|
steatorrhea in chrohn's |
|
|
|
chronic Hep B |
anti HBC igG and HbsAg |
|
|
previous Hep B infect |
anti HBC igG and anti-HBs |
|
|
surface ag appears w , and core w |
|
|
|
HbsAg and igM antiHBC |
acute infexn |
|
|
antiHBs only |
vaccination (surface antigen) |
|
|
hepatitis B surface antiGEN (HBsAg) |
tests for the presence of virus. A "positive" or "reactive" HBsAg test result means that the person is infected with the hepatitis B virus, which can be an "acute" or a "chronic" infection |
|
|
hepatitis B surface antiBODY (HBsAb oranti-HBs) |
person has successfully responded to the hepatitis B vaccine or has recovered from an acute hepatitis B infection |
|
|
hepatitis B core antiBODY (HBcAb) |
|
|
|
acute HepB |
|
|
|
vaccine HepB |
|
|
|
past HepB |
|
|
|
chronic HepB
|
|
|
|
window HepB |
|
|
|
HepB tx |
lamivudine and IFN alpha |
|
|
HepC tx |
peg interferon and ribavirin for portal/bridging fibrosis |
|
|
IBS gets better with |
at night. normal mucosa |
|
|
tenesmus, urgency, bloody diarrhea in AIDS pt |
CMV colitis |
|
|
gastric ulcers need to be |
biopsied to r/o malignancy |
|
|
if penicill allergy, tx h pylori w |
metro, tetra, bismuth, omeprazole |
|
|
hyperTG can cause |
acute pancreatit if TG over 1000. amy/lipase will be artifically reduced |
|
|
smoking+ CDKN2A+ chronic pain |
panc CA |
|
|
renal stone imaging |
NONcontrast CT!!!! |
|
|
degeneration of dorsal and lateral spine tracts |
B12 defic - imparied vibration/proprioception and spastic muscle weakness |
|
|
cytochrome p450 inhibitors (up warfarin effect and bleeding risk) |
|
|
|
cytochrome p450 inducers (down warfarin) |
|
|
|
ASCUS |
|
|
|
5% dextrose and .45% saline |
for mild hypovolemic hypernatremia |
|
|
angioedema |
from ACE-is. can occur anywhere in body. also possible - cough and hyperkalemia |
|
|
bony mets |
|
|
|
clopidogrel |
|
|
|
sharply demarccated erythematous edematous tender skin lesion w raised borders and fever |
erysipelas - mc = group a strep |
|
|
mcc of mitral regurg |
MVP |
|
|
chronic bronchitis |
|
|
|
mcc brain mets |
|
|
|
pulmonary contusion |
|
|
|
pertussis post exposure prophylax |
|
|
|
mcc nephrotic synd in kids |
|
|
|
neuroblastoma |
|
|
|
TSS presentat |
fever, rash throughout body including palms and soles, hypotens |
|
|
noncardiogenic pulm edema |
up CO, low or nml PCWP |
|
|
increased marrow cellularity with megakaryocytic hyperplasia |
essential thrombocytosis |
|
|
hypernatremia, low urine, high serum osmolality |
diabet insipidus |
|
|
hypotonic hyponatremia and euvolemia with low plasma and high urine osmolality with high urine sodium |
|
|
|
slowly progressive anterior him pain w limitation of ROM |
|
|
|
IV acyclovir |
|
|
|
AIN - interstitial nephritis |
|
|
|
male pattern baldness seen in |
PCOS |
|
|
SBO |
|
|
|
corticosteroids for preemies |
under 34 wks |
|
|
mgmt of chorioamnionit |
broad spectrum abx followed by deliver, NOT c-section |
|
|
cor pulmonale |
|
|
|
portal HTN/venous resistance |
cirrhosis - palmar erythema, spider angiomata, caput medusae, gynecomastia |
|
|
serum to ascites albumin (SAAG) |
|
|
|
loop diuretics lytes disturb |
|
|
|
untreated hyperthyroid risk |
rapid bone loss dr up osteoclasts, also tachyarrythm like afib |
|
|
attributable risk percent = excess risk in exposed popl that can be attributed to risk |
|
|
|
multiple small abscess cavities/pneumatocoeles |
s aureus necrotizing bronchopneumona |
|
|
distortion of straight lines on visual acuity test |
macular degeneration |
|
|
coccidiodomycosis |
|
|
|
histoplasmosis |
|
|
|
blastomycosis |
|
|
|
raising cutoff value |
|
|
|
AIDS pt w multiple ring enhancing lesions on CT |
|
|
|
yellow-white patches of retinal opacification and hemorrages |
CMV retinitis, CD4 below 50 |
|
|
enuresis |
desmopressin first line, imipramine next |
|
|
methotrexate side eff |
GI, oral ulcers, stomatitis, rash, alopecia, hepatotox, BM suppress - supplement w folic acid |
|
|
RA predisposes to AA amyloidosis, multiple myseloma to AL |
renal involvement = nephrotic syndo. congo red apple green birefringence under polarized light |
|
|
hyalinosis affecting afferent and efferent arterioles |
diabetic nephropathy |
|
|
linear deposits on IM |
antiglomerular basememt memb = goodpasture |
|
|
granular deposits = immune complex glomerulonephrit |
lupus nephritis, IgA, postinfectious GN |
|
|
h pylori + pernicious anemia + nitrosamines |
adenocarci |
|
|
high fat, lw fiber, ulc colit |
colon CA |
|
|
hemochromatos, NAfatty liver, Hep B/C, aflatoxin, wilson, alpha1antitrypsin |
hepatocell carci |
|
|
pancreatic pseudocyst |
surgically drain if symptomatic |
|
|
nonbloody diarrhea that presents like appendicit - fever + RLQ pain and lekocytosis |
yersenia, but appendicit comes w CONSTIPAT |
|
|
ulc colit + pruritus + up alk phos |
|
|
|
ascites and cirrhotic edema tx |
spironolactone + HCTZ |
|
|
potassium sparing |
spironolact, eplenerone, triametrene, amiloride |
|
|
RUQ |
cholecystit, biliary colic, cholangit, perf duod ulcer |
|
|
LUQ |
splenic rupture, IBS |
|
|
RLQ |
appendicit, ovarian torsion, ectopic, cecal diverticulit |
|
|
LLQ |
sigmoid, volvolus, diverticulit, pregg/egg |
|
|
midepigast |
pancreatic, aort dissect, peptic ulcer dz |
|
|
mcc of epigast pain |
nonulver dyspepsia. eval of epigast pain is w endoscopy |
|
|
PPI |
-prazole. before H2 - tidine |
|
|
mc invasive blooby diarrhea in all age groups |
intrecellular and interstitial edema - soft tissue swelling - compartment syndrome |
|
|
reprefusion after arterio-occlusive ischemia over 4-6 hrs can lead to |
solid food only - from stricture |
|
|
acute vs chronic panc |
|
|
|
if recently exposed to hepA |
|
|
|
first test for dysphagia |
|
|
|
obstruction starts w solid |
EGD |
|
|
NASH / fatty liver |
assoc w DM / metabolic synd - asympt w abl LFTs |
|
|
familial polyposis |
|
|
|
prodromal nausea/pallor/sweat vs prodromal dizziness/blurred vision before syncope |
|
|
|
chest pain, down CO, pulsus paradoxus after viral infection |
|
|
|
lymphocytic pleocytosis, up protein, UP RBC, nml gluc |
HSV encephalit - hemorragic destruction of frontal lobes |
|
|
lymphocytic pleocytosis, up protein, slightly DEC glucose |
chronic bacterial menengit - myco TB |
|
|
nml FEV1/FVC |
|
|
|
down FEV1, nml FVC, down FEV1/FVC |
COPD - bronchitis and emphysema |
|
|
ectopic ACTH is a polypeptide protein |
|
|
|
arrest |
cervix ceases to dilate after reaching 4 cm |
|
|
decrease risk of stroke in Afib |
warfarin |
|
|
empyema vs TB exudate |
|
|
|
SVC syndrome |
lung cancer or lymphoma - tx w radiation |
|
|
blistering of flexure surfaces, groin and axilla w subepidermal blisters on biopsy |
bullous pemphigoid - autoimmune |
|
|
mc intracranial tumor in adults |
brain mets from lung, breast, renal, melanoma |
|
|
upper motor neuron |
hyperreflexia, babinski |
|
|
lower motor neuron |
|
|
|
blank stare, automatism, postictal confusion and (todd's) paralysis |
|
|
|
verapamil |
for SVT if adenosine ineffective |
|
|
wide complex vtach tx |
amiodarone |
|
|
pneumomediastinum suggests |
|
|
|
|
|
|
|
hematuria can be dt glomerular or extraglomerular. proteinuria suggests |
glomerular - igA or poststrep |
|
|
|
|
|
|
urinary frequency, nocturia, freqent small volume leakage |
|
|
|
intense urges that can't be delayed |
|
|
|
urine leaks with laughing/coughing |
|
|
|
iron tox |
|
|
|
afib, dizziness, and weight loss |
hyperthyroid - check T4 and TSH |
|
|
locking and catching joint, knee effusion, pain w squatting |
|
|
|
mammogram |
every 2 years after 50 |
|
|
pain relief w elevation of testis |
|
|
|
SAAG |
|
|
|
lennox gestault |
children under 7 with wide array of seizure types accompanied by MR, slow spike and wave activity on EEG |
|
|
juvenile myoclonic epilepsy |
|
|
|
amebic vs hydatid cyst |
|
|
|
mcc pharyngitis in kids |
|
|
|
distributive shock |
UP CO, DOWN PVR and PCWP |
|
|
anemia hypoalbuminemia coaglopathy in elderly |
malnutrition |
|
|
abort cluster headache |
100% oxygen |
|
|
DKA |
|
|
|
lamivudine |
hepatotox |
|
|
efavirenz |
vivid dreams |
|
|
abacavir |
lactic acidos, hepatit, hypersens rxn |
|
|
triptans should not be given with |
ergotamine |
|
|
migraine abortives |
|
|
|
tocolytics that can cause pulm edema |
|
|
|
migraine abortives |
|
|
|
tocolytics that can cause pulm edema |
|
|
|
best way to prevent progress of diabetic nephropathy |
BP below 130/80 |
|
|
tenderness or nodularity in rectovaginal septum |
|
|
|
loss to followup |
type of selection bias |
|
|
worst risk for stroke |
HTN |
|
|
long PT and PTT |
vit K defic |
|
|
increased bleeding time and PTT, but nml PT |
von williebrand |
|
|
standard deviations in bellshaped distribution |
|
|
|
adult lower GI bleed |
|
|
|
small bowell stasis |
|
|
|
zollinger ellison |
|
|
|
prokinetics for diabetic gastroparesis |
|
|
|
gallstones in sickle cell |
|
|
|
preggo itching in 2nd/3rd trimester |
|
|
|
gardner synd |
|
|
|
turot synd |
polyps and CNS tumors |
|
|
peutz-jagers |
|
|
|
hepatic adenoma |
|
|
|
toxic megacolon tx |
|
|
|
dopamine and hydromorphone GI effects |
PROemetic |
|
|
metoclopramide and ondansetron |
|
|
|
give packed RBCs |
Hct below 30 |
|
|
give FFP |
active bleeding and plt under 50K (unless DIC) |
|
|
variceal bleed tx |
|
|
|
gi bleed tx |
PPI |
|
|
IV doesn't cross bowel wall |
give oral |
|
|
chronic pancreatit |
|
|
|
primary biliary cirrosis |
|
|
|
recurrent pyogenic cholangitis, sclerosing cholangit, and chronic liver dz |
|
|
|
ETEC enterotoxic ecoli |
|
|
|
ulc colit tx |
|
|
|
budd chiari |
|
|
|
peritoneal carcinomatosis |
ascites from ovarian CA |
|
|
PPI better than H2 |
helps prevent recurrence of peptic strictures from GERD |
|
|
vit B12 needs for absorption |
panc enzymes |
|
|
most accurate test for chronic pancreatit |
secretin release
|
|
|
rotor |
|
|
|
dubin johnson |
|
|
|
gilbert |
|
|
|
hemolysis raises |
LDH and UNconj bili |
|
|
ascending cholangitis |
IV resusc, abx, sphincterotomy in 72 hours |
|
|
wilson's |
|
|
|
osler weber rendu |
hereditary (AD) hemorragic telengiactasia - epistaxis, anemia |
|
|
up alk phos and bili, but nml LFTs |
primary biliary cirrosis |
|
|
fever abd pain, AMS, ascites in liver pt |
|
|
|
GERD w no red flags |
lifestyle before PPI |
|
|
crigler najar |
UNconj hyperbili |
|
|
PPIs up serum gastrin by |
supressing gastic acid secretion, so d/c PPIs before serum gastrin test |
|
|
down LES pressure and down peristalsis |
scleroderma |
|
|
UP LES pressure and down peristalsis |
achalasia |
|
|
panc damage consequences |
|
|
|
most hepatocellular carci assoc w cirrosis |
hemorragic ascites and trabecular cells of varying size/shape |
|
|
ascites + fever = paracentesis |
|
|
|
acalculous cholecystit |
|
|
|
defuroxamine |
for hemosiderosis from repeat blood transfusions |
|
|
hemochromatos |
|
|
|
GGTP up in |
binge drinking |
|
|
both HepB and C assoc w |
cirrosis, liver cancer, PAN |
|
|
panc adenocarci presentat |
|
|
|
IFN sideff |
arthralgias, thrombocyto, leuopenia, depress |
|
|
ribavirin sideff |
anemia (also bocephevir) |
|
|
adefovir sideff |
renal dysfx |
|
|
telapevir sideff |
rash |
|
|
total Ca down |
w albumin, but ionized nml in liver dz |
|
|
if suspect cholecystit, but US equivocal |
do HIDA scan aka cholesintigraphy |
|
|
mooth-margin ulcer |
benign |
|
|
yprochlorperazine |
antiemetic |
|
|
biliary colic w/o stones |
sphincter of oddi dysfx - tx w ERCP w manomtry |
|
|
vibrio and giardia |
watery nonbloody diarrhea |
|
|
bloody diarrhea |
|
|
|
schizophrenia neuroimaging |
enlarged lateral cerebral ventricles |
|
|
pleural effusion, ARDS, ileus, ren fail are complicats of |
pancreatit |
|
|
precocious puberty and postmenopausal bleed in elderly |
granulosa cell tumor making excessive estrogen |
|
|
vaccines in preemies |
given to chronologic age, except hep B when they're over 2kg |
|
|
any penetrating wound below 4th intercostal (nipple) |
|
|
|
compare two means |
|
|
|
CF pneumonia in adults vs kids |
|
|
|
fluphenazine |
typical antipsychotic - causes hypothermia |
|
|
RA pts at risk for |
osteopenia, osteoporos, bone fractures - optimize calcium and exercise |
|
|
trihexyphenydil |
|
|
|
Afib caused by |
ectopic foci in pulmonary veins |
|
|
esinos in pee |
acute interstitial nephritis |
|
|
dysmorphic RBC in pee |
glomerulonephritis |
|
|
hyaline casts in pee |
dehydration - protien concentrates |
|
|
brown granular casts in pee |
acute tubular necrosis = dead cells |
|
|
broad waxy casts in pee |
chronic dz |
|
|
prerenal kidney injury |
|
|
|
acute AKI signs |
|
|
|
sodium and water in prerenal kidney injury |
|
|
|
sodium and water in intrinsic acute tubular necrosis |
|
|
|
pOOOontine myelinOOOlysis |
|
|
|
brain EEEdEEEma |
from fixing hypEEEEErnatremia too fast |
|
|
hypercalciuria tx |
|
|
|
GI ischemia/infarction presents with which disturbance |
anion gap met acid - tx w fluids and abx |
|
|
colcichine vs allopurinol |
|
|
|
contrast media vs drugs nephrotox |
|
|
|
tumor lysis syndrome causes AKI |
in 2 days - from hyperuricemia from DNA breakdown - tx w rasburicase |
|
|
oxalate crystals can come from |
bowel resection |
|
|
FSGS |
|
|
|
IBU and NSAIDS renal tox |
|
|
|
rhabdo |
|
|
|
acute tubular necrosis tx |
|
|
|
ototoxic |
furosemide and genta (aminoglycoside) |
|
|
hepatoreanal labs looks like |
|
|
|
pyelonephrit tx |
amp/gent and fluoroquins |
|
|
excessive loops can cause |
met alk - switch to acetazolamide |
|
|
nephrotic |
|
|
|
muscle cramps if missed dialysis |
hyperkalemia - wekaness, paralysis, resp fail, arrythmia, peak T, wide QRS, loss of P |
|
|
hypOkalemia |
U wave and small ST depress, flat T wave, AV block |
|
|
RTA 1 and 2 |
hypOkalemia |
|
|
RTA4 |
|
|
|
eosinos in pee |
|
|
|
TTTubular = acuTTE, TToxin |
|
|
|
glomerular |
|
|
|
goodpasture |
|
|
|
igA/Berger |
|
|
|
amyloidos tx |
melphalan and prednisone |
|
|
nephrotic can look like maltese crosses. causes include |
|
|
|
HTN, metalk, up Na, down K |
|
|
|
gaucher |
|
|
|
RTA2 assoc w |
|
|
|
papillary necrosis in sickle cell |
hematuria, polyuria, nocturia |
|
|
what to supplement in ren fail |
calcium |
|
|
high volume nocturia with dilute urine |
|
|
|
cardiogenic shock |
|
|
|
noncardiogenic pulm edema |
up CO, low or nml PCWP |
|
|
reprefusion after arterio-occlusive ischemia over 4-6 hrs can lead to |
intrecellular and interstitial edema - soft tissue swelling - compartment syndrome |
|
|
breast milk jaundice vs failure |
|
|
|
vision assessment for kids |
every wellchild visit |
|
|
lead buildings year |
before 1978 |
|
|
elevated serum DHEAS |
androgen producing adrenal tumor - virilization |
|
|
WPW + Afib tx |
procainamide and cardioversion |
|
|
what to avoid in WPW |
betas, CCBs, digox, adenosine - because increase conductance through accessory pathway |
|
|
oxytocin produced and realeased |
produced in hypothalamus, released from posterior pituitary (also ADH) |
|
|
hormones deficient in Sheehan's |
anterior pituitary - GH, LH, FSH, TSH, ACTH, prolactin |
|
|
mediastinal tumor locations |
|
|
|
hypertrophic cardiomyopathy (not HOCM) |
|
|
|
valsalva and abrupt standing |
decrease preload, like nitorglycerin |
|
|
hand grip, squatting, leg raise |
|
|
|
MMR for HIV |
|
|
|
lupus nephritis management |
depends on how advanced - do renal biopsy first |
|
|
low back pain under 40 yo worse at night and no improvement w rest but yes improve w activity |
inflammatory - aklylosing spondylitis - apophyseal joint arthritis |
|
|
unilateral varicocele that does not empty when recumbent |
RCC (renal cell carci) - obstructs venous flow - do CT scan |
|
|
HGSIL during pregnancy |
often regress spontaneously - manage conservatively |
|
|
migraine tx |
|
|
|
ACE mechanism |
extracellular enzyme blockage |
|
|
statin mech |
inhibition of intracell sythesis pathway |
|
|
palpable breast mass under and over 30 |
under = US, over = US and mammogram, even if probably benign |
|
|
thrmobocytopenia, eczema, recurrent bacterial infexns |
wiskott aldrich = x linked - decreased plt production |
|
|
cor pulmonale |
|
|
|
progressive periph edema, ascites, elevated JVP, pericardial (iddast) knock, pericard calcificats on CXR |
constrictive pericardit - causes Right HF |
|
|
herniated disk |
|
|
|
vertebral compression fracture |
|
|
|
CML tx |
tyrosine kinase inhibitors - inhibit abl BCR/ABL (9,22 philly) |
|
|
tx of MALT lymphoma w no mets |
eradicate h pylori - omeprazole, clarithro, amoxi |
|
|
removing potassium from body vs shiftin into cells |
|
|
|
bowel ischemia |
decreased bowel sounds, disproportionate pain, metabolic acidosis |
|
|
horizontal nystagmus, cerebellar ataxia, confusion |
phenytoin toxicity |
|
|
tremor, hyperreflexia, ataxia, seizures |
lithium tox |
|
|
slurred speech, unsteady gait, drowsiness, w/o respi depress of pupil constrict |
benzos |
|
|
recurrent respi infects - sinusit, otit media, pna btw 6-18 months |
|
|
|
decreased leuk alk phos |
|
|
|
high leuk alk phos |
polycythemia and leukemid rxn of infxn - functionally active cells |
|
|
stress (hairline) fracture |
of metatarsals - rest and analgesia and hard soled shoe |
|
|
prolonged QT should avoid and use |
avoid electolyte abl and potassium channel blockers, but should USE beta blockers w pacemaker to prevent cardiac arrest |
|
|
pts w cirrosis need |
|
|
|
hypovelemic shock |
|
|
|
hyper vs hyponatremia |
hyper = loss of free H20. hypo = in relation to body volume, nnot just salt |
|
|
addison |
|
|
|
hyponatremia tx based on sympts not # |
|
|
|
recurrent UTI stones |
struvites = ammonium+mg+phosphate |
|
|
SLE assoc w RTA1 |
|
|
|
testic cancer markers |
hcg, AFP, LDH - must resect whole - orchiectomy |
|
|
HTN in chronic ren fail dt |
erythropoetin |
|
|
refractry hypokalemia |
dt hypomg |
|
|
ketorolac |
|
|
|
HTN crisis |
labetalol/nitroprusside, but don't lower to nml or will cause stroke- lower 25% |
|
|
Tdt vaccine |
|
|
|
Tdt vaccine plus tetanus immune globulin |
dirty or severe wound and unclear vaccination status |
|
|
noninvasive, high sens and spec for aneuploidy test at 10 wks |
cell-free fetal DNA |
|
|
malnourished, dehydrated preggo |
|
|
|
caput caccudaneum vs cephalohematoma |
|
|
|
increase venous return (preload) |
leg raise, squat, supine position, handgrip. all but handgrip increase regular murmur, but handgrip makes AS murmur betterc |
|
|
capacitance vessels |
|
|
|
hypercalcemia of malignancy tx |
bisphosphonates - zoledronic acid, pamidronate, also agressive hydration |
|
|
target sign on ultrasound |
itussuception - reduce with air or water contrast enema |
|
|
phototoxic drug eruption |
tetracyclines (doxy) |
|
|
pancytopenia in SLE |
concurrent peripheral immune mediated destruction of all 3 lines |
|
|
hemi-neglect |
right parietal cortex (nondominant) - causing ignoring of left (opposite) side |
|
|
graft vs host |
|
|
|
confirm IUFD with |
real time ultrasonography |
|
|
mc bacterial rhinosinusitis |
s pneum and h influ |
|
|
ethanol vs methanol poisoning |
both cause anion gap acidosis and increased osmolar gap, but methanol damages eyes and ethylene glycol damages kidneys |
|
|
complication of late and post term pregnancy |
oligohydramnios |
|
|
insensitive hypopigmented skin patch |
leprosy - dx w skin biopsy |
|
|
rubella spares palms and soles, unlike |
|
|
|
nephrotic synd assoc w hodkin's lymphoma |
MCD |
|
|
eaton lambert synd |
|
|
|
diabetic neuropathy bladder effect |
overflow incintinence - urine leaks for overdistended bladder |
|
|
urge incontinence caused by |
|
|
|
AKI vs loops disturbances |
|
|
|
complement deficiency |
gonococcl and meningococcal infections - s pneum and h influ |
|
|
t cell defic (such as digeorge) puts at tisk of |
viral and fungal infexns |
|
|
adenosine deaminase defic |
SCID - deficiency of both B and T - so bacteria, fungi, and viruses |
|
|
B cell defic |
recurrent infections after 6 months, like sinopulmonary. lack of IgA = giardia |
|
|
pronator drift sensitive and specific for |
UMN damage |
|
|
upward drift and dysmetria |
cerebellar fx |
|
|
anticuagulation for renal insuffic (glomerular filtration rate under 30 ml/min/1.73 |
unfractionated heparin |
|
|
hip dysplasia dx
|
US under 6 months, xray 4-6 mo
|
|
|
pneumomediastinum and subq emphysemia |
thracheobronchial rupture - can also cause persistent pneumothorax |
|
|
spleen vs panc injury in blunt abd trauma |
spleen injury seen right away, panc can be missed and present later w cyst or retroperitoneal abscess |
|
|
kid torticollis |
get cervical spine xray to r/o cervical spine fract/dislocat |
|
|
bacillary angiomatosis |
|
|
|
precicious puberty - nml bone age =isolated telarche/adrenarche, but if bone age advanced - check |
|
|
|
involved in metabolism of homocyteine |
vit B6, folate, B12 - will lower it |
|
|
pruritic elevated serpingious =progressive creeping, red brown skin lesion from sand contact |
cutaneous larva bigrans - dog and cat hookworm |
|
|
relative risk |
|
|
|
BV vs trich |
|
|
|
pna in CF kids |
staph aureus. p ereug is in ADULTS |
|
|
isolated unilateral motor weakness |
internal capsule |
|
|
MS tx
|
|
|
|
methotrexate sideff |
|
|
|
elevated PCWP |
suspect myocardial dysfx dt cardiac contusion - do echo |
|
|
male teen w epistaxis and a localized mass w bony erosion |
angiofibroma |
|
|
renal artery stenosis presents w |
syst-diast abdominal bruit w HTN and atheroscleros |
|
|
ptosis with down and out gaze and nml light/accommodation |
CNIII diabetic mononerupathy dt ischemic damage - affect somatic, not parasympathetic nerve fibers |
|
|
unstable pt w abd trauma |
fuilds and abd US - if blood on US = laparotomy |
|
|
single loud second heart sound
|
|
|
|
osteosarcoma |
|
|
|
HIV pt w AMS, EBV DNA in CSF, and solitary weakly ring-enhancing periventricular mass on MRI |
|
|
|
cortical and subcortical atrophy and 2ndary ventric enlargement |
AIDS dementia complex |
|
|
prim vs 2nd hyperparathyroid |
|
|
|
cystinuria |
|
|
|
hypoxemia induces |
erithropoetin prduction - leads to polycythemia like in OSA |
|
|
eczema herpeticum |
primary herpes simplex virus infection on top of atopic dermatitis - umbilicated vesikles over erythematous skin - acyclovir |
|
|
exudative pharyngitis w tender anterior cervical LAD and no sniffles (viral) |
strep pharyngit - dx by troat culture and tx w penicillin or amoxicillin |
|
|
screening for women over 65 |
one-time DEXA scan for osteoporosis - (serum Ca and Phosph nml) |
|
|
waxing/waning LFTS |
|
|
|
aspirin reduces risk of early recurrent stroke but |
does not improve neuro sequela of stroke that has already occurred - need fibrinolytics for that |
|
|
chlamydia tx |
single shot of azithro or 7 days of doxy |
|
|
homocysteinuria |
|
|
|
pansyst murmur loudest at left lower sternal border and diastolic rumble at apex |
dt increased flow across mitral valve - VSD |
|
|
hard unilateral nontender solitary lymph nodes in head or neck
|
squamous cell carci of head/neck |
|
|
correlation coefficinet "r" |
shows strength and direction (pos, neg) of linear assoc btw 2 variables, but does not mean causality |
|
|
broca's (expressive) aphasia location |
|
|
|
wernike (receptive) aphasia location |
|
|
|
hypoxia in pts w pna dt |
alveolar and interstit inflammat = v/q mismatch = increase of A-a gradient |