![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
107 Cards in this Set
- Front
- Back
|
overall airway anatomy |
-conducting pathway: nasal passage, mouth, pharynx, larynx -conducting zone: trachea, bronchi ,bronchioles, terminal bronchioles -transitional and respiratory zones: respiratory bronchioles, alveolar ducts, alveolar sacs |
|
|
conducting airways |
-through which air moves as it passes between the atmosphere and the lungs -contains: (upper airways) nasal passage, mouth, pharynx, larynx, (lower airways) trachea, R and L main bronchi, secondary bronchi, bronchioles -upper: ventilation, humidifies and filters air, anatomic dead space -lower: defense mechanisms (irritant reflex, mucocillary, immunity), gas exchange, anatomic dead space |
|
|
type 1 alveolar cells |
-thin squamous cells -flattened nucleus -95% of alveoli surface area -allows easy movement through for gas exchange -prevents plural effusuion |
|
|
type 2 alveolar cells |
-small cuboidal cells located at corners of alveoli -as numerous as type 1 but different cell shape so they only cover5% of surface area of alveoli -synthesis and secrete surfactant surfactant: substance that decreases surface tension in alveoli and allows for greater ease of lung inflation |
|
|
ventilation |
the movement of gases into and out of the lungs through a system of open air- ways and along a pressure gradient resulting from a change in chest volume. |
|
|
inspriration |
-air is drawn into the lungs as the respiratory muscles expand the chest cavity; -the size of the chest cavity increases, the intra- thoracic pressure becomes more negative, and air is drawn into the lungs. -pulmonary pressure is less than atmospheric pressure |
|
|
experation |
-air moves out of the lungs as the chest muscles recoil and the chest cavity becomes smaller -occurs as the elastic components of the chest wall and lung structures that were stretched dur- ing inspiration recoil, causing the size of the chest cavity to decrease and the pressure in the chest cavity to increase. -pulm pressure is greater than atmospheric pressure |
|
|
** |
-The move- meant of gases is always from the container with the greater pressure to the one with the lesser pressure -The ease with which air is moved into and out of the lung depends on the resistance of the airways, which is inversely related to the fourth power of the airway radius, and lung compliance, or the ease with which the lungs can be inflated. |
|
|
internal resperation |
** |
|
|
external respiration |
** |
|
|
lung compliance |
-the ease with which the lungs can be inflated -determined by the elastin and colla- gen fibers of the lung, its water content, and surface tension -Overstretching lung tissues, as occurs with emphysema, causes the elastic components of the lung to lose their recoil, making the lung easier to inflate but more difficult to deflate because of its inability to recoil. |
|
|
airway resistance and asthma |
Airway resistance is greatly affected by lung volumes. Resistance is less during inspiration than expiration. This is because elastic fibers connect the outside of the airways to the surrounding lung tissues. As a result, these airways are pulled open as the lungs expand during inspiration, and they become narrower as the lungs deflate during expiration (Fig. 35.15). This is one of the reasons why people with conditions that increase airway resistance, such as asthma (reactive airway), usually have less difficulty breathing during inspiration than during expiration.Airway resistance is also affected by the bronchial smooth muscle tone that controls airway diameter. The smooth muscles in the airway, from the trachea down to the terminal bronchioles, are under autonomic nervous system control. Stimulation of the parasympathetic nervous system causes bronchial constriction as well as increased mucus secretion. Sympathetic stimulation has the opposite effect. |
|
|
tital volume |
Amount of air that moves into and out of the lungs with each breath |
|
|
Inspiratory reserve volume |
Maximum amount of air that can be inhaled from the point of maximal expiration |
|
|
Expiratory reserve volume |
Maximum volume of air that can be exhaled from the resting end-expiratory level |
|
|
Residual volume |
Volume of air remaining in the lungs after maximal expiration. This volume cannot be measured with the spirometer. It is measured indirectly using methods such as the helium dilution method, the nitrogen washout tech- nique, or body plethysmography. -increase in RV for COPD |
|
|
Functional residualcpasity |
Volume of air remaining in the lungs at end-expiration (sum of RV and ERV) Sum of IRV and TV |
|
|
Inspiratory capacity |
Sum of IRV and TV |
|
|
Vital capacity |
Maximal amount of air that can be forcibly exhaled from the point of maxi- mal inspiration |
|
|
Total lung capacity |
Total amount of air that the lungs can hold. It is the sum of all the volume components after maximal inspiration. This value is about 20%-25% less in females than in males. |
|
|
ventilation |
-the flow of gases into and out of the alveoli of the lungs -Pulmonary ventilation refers to the total exchange of gases between the atmosphere and the lungs. Alveolar ventila- tion is the exchange of gases within the gas exchange portion of the lungs |
|
|
dead air space |
-air that must be moved with each breath but does not participate in gas exchange -Anatomic dead space: that contained in the conducting airways -Alveolar dead space: that contained in the respiratory portion of the lung |
|
|
Perfusion |
-the flow of blood in the adjacent pulmonary capillaries |
|
|
mismatching of ventilation and persufusion |
The gas exchange properties of the lung depend on match- ing ventilation and perfusion, ensuring that equal amounts of air and blood are entering the respiratory portion of the lungs. Both dead air space and shunt produce a mismatch- ing of ventilation and perfusion, |
|
|
diffusion |
- occurs in the respiratory portions of the lung and refers to the movement of gases across the alveolar-capillary membrane. |
|
|
oxogen transportation |
-2 forms: dissolved state (1%) and hemoglobin (99%) -As the oxygen moves out of the capillaries in response to the needs of the tissues, the hemoglobin saturation drops. -The term affin- ity refers to hemoglobin's ability to bind oxygen. Hemoglobin binds oxygen more readily when its affinity is increased and releases it more readily when its affinity is decreased -each hemoglobin molecule can bind four molecules of oxygen when it is fully saturated -After the first molecule of oxygen binds to hemo- globin, the molecule undergoes a change in shape. As a result, the second and third molecules bind more readily, and bind- ing of the fourth molecule is even easier. In a like manner, the unloading of the first molecule of oxygen enhances the unloading of the next molecule and so on. Thus, the affinity of hemoglobin for oxygen changes with hemoglobin saturation -Hemoglobin's affinity for oxygen is also influenced by pH, carbon dioxide concentration, and body temperature. It binds oxygen more readily under conditions of increased pH (alkalosis), decreased carbon dioxide concentration, and decreased body temperature, and it releases it more readily under conditions of decreased pH (acidosis), increased carbon dioxide concentration, and fever -anemia affects curve: -The S-shaped oxygen dissociation curve has a flat top portion representing binding of oxygen to hemoglobin in the lungs and a steep portion representing its release into the tissue capillaries |
|
|
Hypoxemia |
reduction in arterial blood 0 2 levels, which is considered a PaO 2 less than 95 mm Hg |
|
|
Hypercapnia |
-refers to an increase in the carbon dioxide con- tent of the arterial blood - The carbon dioxide level in the arterial blood, or PCO 2, is proportional to carbon dioxide pro- duction and inversely related to alveolar ventilation |
|
|
asthma |
-Asthma represents an acute and reversbile form of airway disease caused by narrowing of airways due to bronchospasm, inflammation, and increased airway secretions -chronic disorder of airways -eipsodes of airway hypperresonsiveness, airway obstruction, and airway inflammation -episodes are reversible (treatable but not curable) |
|
|
factors that contribute to the development of a asthma attack |
-allergens: -repeated respiratory tract infections -exercise -drugs and chem -hormonal changes and emotional upsets -airborne pollutants -gastroesophageal reflux |
|
|
FEV1 |
-Forced expiatory volume in 1 second -amount of air coming out during 1st second of forced expiration -should be 80% of lung volume -if its less than 80% it means there is an increase in RV |
|
|
classification of asthma severity |
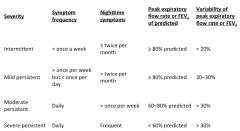
-mild intermediate -mild persistant: -moderate persistant -severe persistant |
|
|
types of asthma |
-extrinsic (atopic) asthma: triggered by exposure to allergen and subsequent immune respsonse -intrinsic (nontoxic) asthma: triggered by non immune response |
|
|
extrinsic asthma pathogenesis
|
common denominator underlying asthma is an exag- gerated hyperresponsiveness to a variety of stimuli. Airway inflammation manifested by the presence of inflammatory cells (particularly eosinophils, lymphocytes, and mast cells) and by damage to the bronchial epithelium contributes to the patho- genesis of the disease. -cells. TzH cells, on the other hand, respond to allergens and helminths (intestinal para- sites) by stimulating B cells to differentiate into IgE-producing plasma cells, produce growth factors for mast cells, and recruit and activate eosinophils. In people with allergic asthma, T-cell differentiation appears to be skewed toward a pro inflammatory TzH response. -Cytokines also have an apparent role in the chronic inflammatory response and complications of asthma. Tumor necrosis factor (TNF)-c and interleukins 4 and 5 (IL-4, IL-5) participate in the pathogenesis of bronchial asthma through their effects on the bronchial epithelial and smooth muscle cells.Z0 22 Studies suggest that TNF-a, an inflammatory cyto- kine that is stored and released from mast cells, plays a critical role in the initiation and amplification of airway inflamma- tion in persons with asthma. TNF-a is credited with increas- ing the migration and activation of inflammatory cells (i.e., eosinophils and neutrophils) and contributing to all aspects of airway remodeling, including proliferation and activation of fibroblasts, increased production of extracellular matrix gly- coproteins, and mucous cell hyperplasia, -airways. The immunological aspects of asthma including the cascade of neutrophils, eosinophils, lym- phocytes, and mast cells cause epithelial injury. This causes airway inflammation, which further increases hyperresponsive- ness and decreased airflow? 4 There are multiple mediators and cell types that cause the inflammation and airway bronchocon- striction in asthma. When mast cells are activated, the release of histamine; prostaglandin Dz; cytokines such as IL-1 to IL-5, interferon, TNF, and granulocyte-macrophage colony-stimulat- ing factor; and leukotrienes causes massive bronchoconstriction and inflammation of pulmonary vasculature endothelium. Mast cells can trigger multiple cytokine release, which causes major inflammation of the airway. The contraction of the airways and subsequent swelling leads to further airway obstruction. -Eosinophils tend to be present in airways of people with asthma and generate inflammatory enzymes and release leu- kotrienes and many pro inflammatory enzymes. -The release of leukotrienes causes more mucus secretion, which often obstructs the airway further and causes more histamine release from the mast cells. |
|
|
intrinsic asthma trigger examples and their pathogenesis |
-respiratory tract infections -exercise -cold air -bronchial irritants (tobacco smoke, chem, strong odors) -emotional upset -menses |
|
|
signs and symptoms of asthma |
-dyspnea -wheezing -chest tightness -coughing -fatigue -hypoxia and hypercapnia -moist skin -sense of panic -LOC |
|
|
asthma diagnosis |
history and physical exam -pulmonary function tests + asthma spirometry ~ provides a means for measuring FVC, FEV1, PEF, tidal volume, expiratory reserve capacity, and inspiratory reserve capacity ~ asthma: increased RV, FCR, TLC ~asthma forced expiration curve +PEF rate (L/sec) |
|
|
treatment of asthma |
-trigger identification and avoidance -medications +bronchodilators (relivers) or anti inflamitory (controlers) actions +quick relief or long term control medications The first line of treatment with any of the persistent forms of asthma includes an inflammatory con- troller drug that would include inhaled corticosteroids (ICS), mast cell stabilizers, and leukotriene modifiers. ICS are con- sidered the most effective in preventing airway inflammation and generally the drug used. |
|
|
asthma medications |
-quick relief +short acting beta 2 agonists: activating sympathetic response, broncodialation,opening airways, within minutes it works, often in inhalers +anticholiinergic agents: block parasympathetic nervous system, inhalers, nebulizers, a little but more time to work, they also persist longer than above, can work for a few hours, only use this in severe cases, often they may be proscribe together these two -long term control +corticosterioids: +long acting beta 2 agonists: +antileukotrienes: ** |
|
|
COPD characteristics |
-inflamation and fibrosis of bronchial wall and excess mucus -destruction of alveolar tissue: decrease surface area of alveoli which decreases possible gas exchange -loss of elastic fibers with in smooth mucle: needed for recoil during expiration and w/o it RV increases |
|
|
COPD risk factors |
1) smoking * 2) genetic mutation 3) asthma and airway hyperresonsiveness |
|
|
types of COPD |
-emphasema +destruction of alveolar walls and enlargement of air spaces +elastic fibers destroid -chronic bronchitis +obstruction of major and small airways +brochial wall hypertrophy +mucus hypersecretion +persistant, productive cough |
|
|
emphysema pathogenesis |
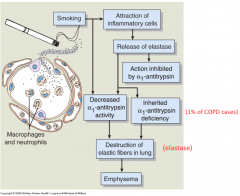
-destruction of elatic fibers --> hyperinflation - |
|
|
emphysema signs and symptoms |
-shortness of breath: to much air in lungs and can't get enough in --> feel short of breath -coughing -wheezing -barel chest: increased trapped air increases lung size -use of accessory muscles -weight loss: caused by depression or increase in co2 or decrease in activity causing muscle wasting -lack of cyanosis (pink) -rapid and shallow breathing; pursed lips (puffer) breathing |
|
|
chronic bronchitis risk factors, most common in ____ , and diagnosis criteria |
-risk factors: chronic irritation from smoking or chronic respiratory infections -most common in middle aged men -diagnosis criteria: persistent productive cough for 3 consecutive months for 2 consecutive years |
|
|
chronic bronchitis pathogenesis |
* |
|
|
chronic bronchitis signs and symptoms |
-chronic cough -suptum production -blue bloater -cyanosis (results from severe hypoxia) -right heart failure -fluid retension |
|
|
COPD treatment |
-no cure, just treatments to slow progression of diease -smoking cessation -medications +bronchodilators ~beta 2 agonists (short and long acting) ~anticholinergic drugs +corticosteriods +oxogen therapy ~ arterial pO2 <55mmhg ~goal: maintain a hemoglobin oxogen sat of at least 90% -good nutrition -pulmonary rehabilitation programs -prevent reap infections |
|
|
proliferation |
-i.e. the process of cell division, is an adaptive process for new cell growth to replace old cells or when additional cells are needed -Proliferation à normal division, normal cell growth, can be regenerating cells, some cells will not continuously regrow but fromthe stem cell phase they will do this, production of cells and the balance between new healthy cells and cell death -Cell proliferation is the process of increasing cell numbers by mitotic cell division. |
|
|
differentiation |
-the mechanism by which cells become increasingly more specialized with each mitotic division. -Differentiation à stem cell à to specific cell, cell knows what it is has a purpose and a specific life expectancy -Cell differentiation is determined by genes à genes determining cellIN cancer we loose the ability to differentiate the cell from abnormal proliferation so now in cancer we have an undifferentiated cell going through proliferation |
|
|
apoptosis |
-a form of programmed cell death -programed cell death targeting specific cells in a programed manor -A cell has been labeled for apoptosis and a macrophage goes in an gets rid of it, a cancer cell isn’t going to be marked for destruction isn’t going through these phases -cancer can evade apoptosis |
|
|
the cell cycle |
-G 1 (gap 1) occurs after the post mitosis phase when DNA synthesis stops and ribonucleic acid (RNA) and protein synthesis and cell growth take place;protein synthesis and an increase in organelle and cytoskel- etal elements. -S phase, DNA synthesis occurs, causing two separate sets of chromosomes to develop, one for each daughter cell;period of DNA synthesis and replica- tion of the chromosomes. -G 2 (gap 2) is the pre mitotic phase and is similar to G1 in that DNA synthe- sis stops, but RNA and protein synthesis continue;premitotic phase. During this phase, enzymes and other proteins needed for cell division are syn- thesized and moved to their proper sites. - The phases, G, S, and G2, are referred to as interphase -The M phase is the phase of nuclear division, or mitosis, and cytoplasmic division;formation of the mitotic spindle and cell division with formation of two daughter cells -When environmental conditions are adverse, such as nutrient or growth factor unavailability, or when cells are highly specialized, cells may leave the cell cycle, becoming mitotically quiescent, and reside in a resting state known as G O . Cells in G o may reenter the cell cycle in response to extra- cellular nutrients, growth factors, hormones, and other signals such as blood loss or tissue injury that trigger cell growth;GO is the stage after mitosis during which a cell may leave the cell cycle and either remain in a state of inactivity or reenter the cell cycle at another time. |
|
|
regulation of the cell cycle |
-cyclins are a group of proteins that control the entry and progression of cells through the cell cycle. Cyclins bind to proteins called cyclin-dependent kinases (CDKs). Kinases are enzymes that phosphorylate proteins. The CDKs phosphorylate specific target proteins and are expressed continuously during the cell cycle but in an inactive form, whereas the cyclins are synthe- sized during specific phases of the cell cycle and then degraded by ubiquitination once their task is completed? -the transition from G 2 to M is considered to be one of the most important checkpoints in the cell cycle. In addition to the synthesis and degradation of the cyclins, the cyclinCDK complexes are regulated by the binding of CDK inhibitors (CKIs). The CKIs are particularly important in regulating cell cycle checkpoints during which mistakes in DNA replication are repaired -The cyclins are a family of proteins that control entry and progression of cells through the cell cycle. They func- tion by activating proteins called CDKs. Different combina- tions of cyclins and CDKs are associated with each stage of the cell cycle. In addition to the synthesis and degradation of the cyclins, the cyclin-CDK complexes are regulated by the binding of CKIs. The CDK inhibitors are particularly important in regulating cell cycle checkpoints during which mistakes in DNA replication are repaired -G1/S: checks for DNA dammage -g2/M:checks for damaged or unduplicated dna |
|
|
neoplasia |
a new growth, not cancer just a new growth (moles are an example) |
|
|
neoplasm |
-(tumors) à oncology à abnormal proliferation à new growth nor forms a mass, now have to worry a bit -an abnormal mass of tissue in which the growth exceeds and is uncoordinated with that of the normal tissues -do not obey the laws of normal cell growth. They serve no useful purpose, they do not occur in response to an appro- priate stimulus, and they continue to grow at the expense of the host. |
|
|
benign |
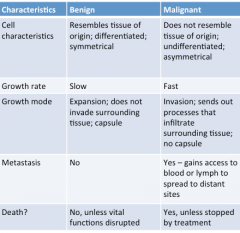
-Neoplasms that contain well-differentiated cells that are clustered together in a single mass are considered to be benign. These tumors usually do not cause death unless their location or size interferes with vital functions -The capsule is responsible for a sharp line of demarcation between the benign tumor and the adjacent tissues, a factor that facilitates surgical removal. |
|
|
malignant |
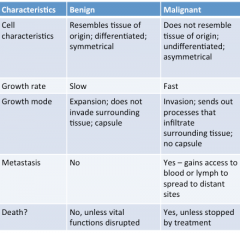
-are less well differentiated and have the ability to break loose, enter the circulatory or lymphatic system, and form secondary malignant tumors at other sites -rapid rate of growth, malignant tumors may compress blood vessels and outgrow their blood supply, causing ischemia and tissue injury. |
|
|
cancer cell characteristics |
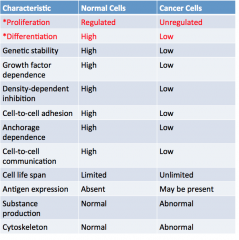
-Cancer cells are characterized by two main features--abnor- map and rapid proliferation and loss of differentiation. Loss of differentiation means that they do not exhibit normal features and properties of differentiated cells and hence are more simi- lar to embryonic cells -anaplasia describes the loss of cell differen- tiation in cancerous tissue -Both the cells and nuclei display variations in size and shape, a condi- tion referred to as pleomorphism. -Their nuclei are variable in size and bizarre in shape, their chromatin is coarse and clumped, and their nucleoli are often considerably larger than normal -Frequently, the nuclei contain an abnormal number of chromosomes (aneuploidy). The cells of undifferentiated tumors usually display greater numbers of cells in mitosis due to their high rate of proliferation. -The characteristics of altered prolif- eration and differentiation are associated with a number of other changes in cell characteristics and cell function, including genetic instability; growth factor independence; loss of cell density-dependent inhibition, cohesiveness and adhesion, and anchorage dependence; faulty cell-to- cell communication; indefinite cell life span (immortality); expression of altered tissue antigens; abnormal secretion of degradative enzymes that enable invasion and metastatic spread, or ectopic production of hormones; and abnormal cytoskeletal characteristics. |
|
|
anaplasia |
describes the loss of cell differen- tiation in cancerous tissue |
|
|
pleomorphism |
Both the cells and nuclei display variations in size and shape, a condi- tion referred to as ___ |
|
|
aneuploidy |
-Frequently, the nuclei contain an abnormal number of chromosomes -Hyerchromatic & Aneuploidy à more chromatin, abnormal number or chromosomes |
|
|
metaplasia |
cellular change, loss of differentiation |
|
|
Displaisias |
Displaisias à abnormal development of cell type, abnormally developing from what it should be developing into |
|
|
* |
Epithelial (Carcinoma) Connective (Sarcoma) Blood (Leukemia, Lymphoma, Myeloma) |
|
|
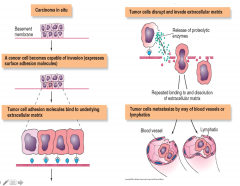
in order to metastasis |
1. have to have the ability to break loose from primary tumor2. gain access to a blood or lymphatic vessel3. if we survive the passage now we have to get out taking us to the part of the body we want to attack and we have to break out this is where we get the development of secondary tumors, very hard to no where this undifferentiated cell came from4.5.6. needs blood supply à it can take advantage or tissues blood supply if it has invaded a tissue or it can develop its own blood supply à angiogenesis form new blood vessels to support their growth7. now begin to grow -To metastasize, a cancer cell must be able to break loose from the primary tumor, invade the surrounding extracellular matrix, gain access to a blood ves- sel, survive its passage in the bloodstream, emerge from the bloodstream at a favorable location, invade the surrounding tissue, begin to grow, and establish a blood supply |
|
|
tumor growth depends on and etc |
-Adequate blood supply -Number of cells moving through cell cycle -Duration of cell cycle -Balance between cell formation and cell death -It has been shown that the cell cycle time of cancerous tissue cells is not necessarily shorter than that of normal cells. Rather, cancer cells do not die on schedule and growth factors prevent cells from exiting the cycle cell and entering the G o phase. Thus, a greater percentage of cells are actively engaged in cycling than occurs in normal tissue -As the growth fraction increases, the doubling time decreases. When normal tissues reach their adult size, equi- librium between cell birth and cell death is reached. Cancer cells, however, continue to divide until limitations in blood supply and nutrients inhibit their growth. When this happens, the doubling time for cancer cells decreases. -curve shows greatest growth rate occurs in the middle |
|
|
ways cancer can spread |
direct invasion and extension:Most cancers synthesize and secrete enzymes that break down proteins and contribute to the infiltration, invasion, and penetration of the surrounding tissues. The lack of a sharp line of demarcation separating them from the surrounding tissue makes the com- plete surgical removal of malignant tumors more difficult than removal of benign tumors -seeding of cancer cells in body cavities when a tumor sheds cells into these spaces. -metastatic spread through the blood or lymph pathways;Because metastatic tumors frequently retain many of the characteristics of the primary tumor from which they were derived, it usually is possible to determine the site of the primary tumor from the cellular characteristics of the metastatic tumor. |
|
|
angiogenesis |
develop- ment of new blood vessels |
|
|
growth fraction |
The ratio of dividing cells to resting cells in a tissue mass |
|
|
doubling time |
length of time it takes for the total mass of cells in a tumor to double. |
|
|
x rays detects a tumor when .... |
a tumor usually is undetectable until it has doubled 30 times and contains more than 1 billion (10 9) cells. At this point, it is approximately 1 cm in size. |
|
|
etiology of cancer |
1) genetic factors and molecular mechanisms;The genetic and molecular mechanisms that are involved and that characterize the transformation of normal cells to cancer cells;Genes that increase susceptibility to cancer or facilitate cancer include defects in DNA repair mechanisms, defects in growth factor signaling pathways, evasion of apoptosis, avoidance of cel- lular senescence, development of sustained angiogenesis, and metastasis and invasion. In addition, associated genetic mutations are involved that enable invasion of and survival in neighboring tissue, as well as evasion of immune detection and attack. 2) host and environmental factors;The external and more contextual factors such as age, heredity, and environmental agents that contribute to the development and progression of cancer;Among the traditional risk factors that have been linked to cancer are heredity, hormonal factors, immunologic mechanisms, and environmental agents such as chemicals, radiation, and cancer-causing viruses. More recently, there has been interest in obesity as a risk factor for cancer. both contribute complex process |
|
|
cancer associated genes |
-oncogenes -tumor supressor genes -genes that control apoptosis -dna repair genes |
|
|
oncogenes |
-protooncogenes, which are normal genes that become cancer-causing onco- genes if mutated. Protooncogenes encode for normal cell pro- teins such as growth factors, growth factor receptors, growth factor signaling molecules, and transcription factors that promote cell growth or increase growth factor-dependent signaling. -mutated protooncogenese are called ongogenese and overactivity of ______ -Oncogenes are mutated proto-oncogenes, these are important for normal cell growth, when this becomes a problem is when the protooncogene becomes mutated, if this mutation occurs within a coding region of gene, we have problems will go on to create over activity |
|
|
tumor supressor genes |
-prevent decision not passing on defective cell in no dell division side à at lease until we can sequester DNA or push it into DNA, this is until we have mutated tumor suppressor genes anything causing genes or DNA to become damages these tumor suppressor cells are just a part of your DNA make up, kinda like a surveillance system -The category associated with gene under activity com- prises the tumor suppressor genes, which, by being less active, create an environment in which cancer is promoted. -Tumor suppressor genes inhibit the prolif- eration of cells in a tumor. When this type of gene is inacti- vated, a genetic signal that normally inhibits cell proliferation is removed, thereby causing unregulated growth to begin. |
|
|
viruses as a cause of cancer |
-what regulated the cell cycle à cdk and cyclin when these two bound it caused cycle to continue à why à cyclin dependent kinase à protein that phosprplates proteinsà this action causes cycle to continueso in retro viruses they found that these viruses insert within the gene and the product within these viruses are protein kinases à this is going to continue to phosoralzie causing cell cyle to speed up -An oncogenic virus is one that can induce cancer -human papilloma virus (HPV) +cervical cancer +gardisil vaccine -hepatitis B virus (HBV) +liver cancer -Epstein-barr virus (EBV) +lymphomas, nasopharyngeal cancer -human herpes virus 8 (HHV8) +kaposi sarcoma in ppl with aids |
|
|
apoptosis as a cancer associated gene |
when looking at cell cycle remember we have ability to push cell out into apoptosis out of cycle tumor suppressor genes that are not mutated will help push it out, there are genes that help promote apopotoic pathway if any of those become mutated there can also be problems à prior to cell division is where we want to see apoptosis occurring -Because apoptosis is considered a normal cellular response to DNA damage, loss of normal apoptotic pathways may contribute to cancer by enabling DNA-damaged cells to survive. |
|
|
carcinogenesis |
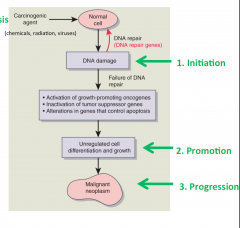
initiation, promotion, and progression (Fig. 8.14). Initiation is the first step and describes the exposure of cells to a carcinogenic agent that causes them to be vulnerable to can- cer transformation. 2 The carcinogenic agents can be chemical, physical, or biologic and produce irreversible changes in the genome of a previously normal cell. Because the effects of initiating agents are irreversible, multiple divided doses may achieve the same effects as a single exposure to the same total dose or to small amounts of highly carcinogenic substances. The cells most susceptible to mutagenic alterations are those that are actively synthesizing DNA.Promotion is the second step that allows for prolific growth of cells triggered by multiple growth factors and chemicals? Promotion is reversible if the promoter substance is removed. Cells that have been irreversibly initiated may be promoted even after long latency periods. The latency period varies with the type of agent, the dosage, and the characteris- tics of the target cells. Many chemical carcinogens are called complete carcinogens because they can initiate and promote neoplastic transformation. Progression is the last step of the process that manifests when tumor cells acquire malignant phenotypic changes that promote invasiveness, metastatic competence, autonomous growth tendencies, and increased karyotypic instability. |
|
|
SNA repair defects as an etiology for cancer |
-The DNA repair genes affect cell proliferation and survival indirectly through their ability to repair damage in protooncogenes, genes impacting apopto- sis, and tumor suppressor genes? Genetic damage may be caused by the action of chemicals, radiation, or viruses, or it may be inherited in the germ line. (ex: carciogenesis) |
|
|
hormones has host factor for causing cancer |
Hormones have received considerable research attention with respect to cancer of the breast, ovary, and endometrium in women and of the prostate and testis in men.ability of hormones to drive the cell division of a malignant phenotype. |
|
|
immune system dysfunction as as etiology for cancer |
-immune surveillance hypothesis, first proposed in 1909, postulates that the immune system plays a central role in resistance against the develop- meant of tumors -It has been suggested that the development of cancer might be associated with impairment or decline in the surveil- lance capacity of the immune system. For example, increases in cancer incidence have been observed in people with immu- no deficiency diseases and in those with organ transplants who are receiving immunosuppressant drugs. -3 Es +elimination phase: work if number of immune cells out number the transformed cells --> protection +equilibrium: number of transformed cells = number of immune cells --> some protection +escape: transformed cells outnumber immune cells --> no protection --> further stages of cancer -Virtually all of the components of the immune system have the potential for eradicating cancer cells, including T lymphocytes, B lymphocytes and antibodies, macrophages, and natural killer (NK) cells. The T-cell response is undoubt- edly one of the most important host responses for control- ling the growth of antigenic tumor cells. |
|
|
carcinogen |
- an agent capable of causing cancer. -dose dependednt -asbestos (roof, insulation): lung cancer -arsenic (insecticide): cancer of lung and skin -lead (paint): cancer of stomach, lung, blader -radon (basement): ling cencer |
|
|
life style choices that can cause cancer |
- Smokingand Tobacco Use –Tobaccocontains over 50 carcinogens –Smokingdirect cause of lung and laryngealcancer –Smokinglinked with cancers of mouth, nasal cavities, pharynx, esophagus, pancreas,liver, kidney, uterus, cervix, bladder, and blood (leukemias) –Smokelesstobacco increases cancers of mouth and esophagus -AlcoholUse –Mechanismcomplex –Associatedwith variety of cancers –Combinationof smoking and drinking: increased risk cancers of mouth, larynx, esophagus -Diet –Carcinogensin foods that are charcoal-broiled, smoked, salted, cured, pickled –Coloncancer associated with high intake of fat and red meat, low intake of dietaryfiber •Obesity: Increasedrisk colon cancer |
|
|
the hall marks of cancer |
1)oncogenes; self sufficiency in growth signaling 2) insensitivity to antigrowth signals; inactivity of suppressor genes 3) tissue invasion and metastasis 4) limitless replicative potential; imortal cells 5)sustained angiogenesis 6)evaiding apoptosis 7)deregulated metabolism 8)evading the immune system 9) unstable DNA 10) inflammation |
|
|
local signs and symptoms of cancer |
•Lump(e.g. breast cancer)•Hemorrhage(e.g. colorectal cancer)•Obstruction(e.g. cancers of lung or intestines)•Effusionin pleural, pericardial, or peritoneal cavity•Fracture(e.g. bone cancer)•Woundthat will not heal (e.g. skin cancer)•Pain(usually late) |
|
|
systemic signs and symptoms of cancer |
-cancer anorexia chachexia syndrom -fatique and sleep disturbances -anemia -paraneoplastic syndromes: addition to signs and symptoms at the sites of primary and metastatic disease, cancer can produce manifestations in sites that are not directly affected by the disease. |
|
|
cancer anorexia chachexia syndrome |
-Many cancers are associated with weight loss and wasting of body fat and muscle tissue, accompanied by profound weak- ness, anorexia, and anemia. -Although anorexia, reduced food intake, and abnormali- ties of taste are common in people with cancer and often are accentuated by treatment methods, the extent of weight loss and protein wasting cannot be explained in terms of diminished food intake alone. -The mechanisms of cancer cachexia appear to reside in a hyper metabolic state and altered nutrient metabolism that are specific to the tumor-bearing state. -***** |
|
|
anemia as a sign/symp of cancer |
It may be related to blood loss, hemolysis, impaired red blood cell production, or treatment effects. |
|
|
fatigue and sleep disturbances as a symp/sign of cancer |
It occurs both as a consequence of the cancer itself and as a side effect of cancer treatment. |
|
|
syndrome of inappropriate ADH secretion (SIADH) |

-ADH increase blood volume -lung cancer tumor secretes ADH (not pit) -causes hyponatremia (low levels of sodium) because blood is diluted and hypoosmolality -sodium is used in action potentials for neurodeficits can occur at brain and motor level -signs and sump: confusion, delirium, muscle weakness |
|
|
Lambert- Eaton syndrome |
-small cell lung cancer. -produces muscle weakness in the limbs -The altered immune response is initiated by the production of onconeural antigens (e.g., antigens normally expressed in the nervous system) by the cancer cells. The immune system, in turn, recognizes the onconeural antigens as foreign and mounts an immune response. -The anti- bodies and cytotoxic T cells are not sufficient to cause neu- rologic disease unless they cross the blood-brain barrier and react with neurons expressing the onconeural antigen. -antibodies destroy calcium channels so depolarization can not be achieved -there is a drug that prevents K exiting so neuron can now depolarize |
|
|
diagnosing cancer |
-suspicion: +signs and symp +screening -investigation +blood tests +x rays +Ct scan +endoscopy +laproscopy -definitive diagnosis +examination of cells by pathologist +tissue biopsy via needle, endoscopy, laproscopy, surgery |
|
|
cancer screening |
-breast cancer: palpation, mammogram -cervical cancer: pap smear -colorectal cancer: fecal occult blood test, colonoscopy -prostate cancer: PSA testing, palpation -skin cancer: skin checks -Screening represents a secondary prevention measure for the early recognition of cancer in an otherwise asymptomatic population? |
|
|
classifying cancer |
-grading: degree of abnormality;Grading of tumors involves the microscopic examination of cancer cells to determine their level of differ- entiation and the number of mitoses. Cancers are classified as grades I, II, III, and IV with increasing anaplasia or lack of differentiation. +grade 1-4 with 1 being cell looks well differentiated and 4 being undifferentiated -staging: egree of spread +stage 1-4 with higher number being more spread -TNM classification -It is useful in deter- mining the choice of treatment for individual people, estimat- ing prognosis, and comparing the results of different treatment regimens. |
|
|
TNM |
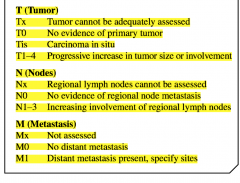
-T stands for the size and local spread of the primary tumor. - N refers to the involvement of the regional lymph nodes. -M describes the extent of the metastatic involvement. |
|
|
cancer treatment goals and types |
The goals of cancer treatment methods fall into three catego- ries: curative, control, and palliative. The most common modal- ides are surgery, radiation therapy, chemotherapy, hormonal therapy, and biotherapy. |
|
|
surgery |
-curative +complete removal of tumor +small tumors with well defined boarders -paliative +bowel obstruction +spinal cord compression +sever nerves to decrease pain -preventative +prophylatic mastectomy +removal of precancerous polyps in colon |
|
|
radiation |
-used alone or in combination with survey and/or chemo -curritive or palliative -high energy particles or waves damage or kill cancer cells -rapidly proliferating and poorly differentiated cells more likely to be killed than slowly proliferating cells of normal tissue -double stranded break need to occur to kill cells -can not distinguish between cancer cells and rapidly dividing cells in normal tissue -affects GI tract (nausea and vommiting), skin and hair cells (hair loss), bone marrow (leukocytes [infection], thrombocytes [bleeding], erythrocytes [anemia]) -Radiation can interrupt the cell cycle process, kill cells, or damage DNA in the cells? Radiation must produce double-stranded breaks in DNA to kill a cell, owing to the high capacity of cells for repairing single-stranded breaks. -3 types: external beam, brachytherapy, and unseald internal radiation sources |
|
|
external beam radiation therapy |
* |
|
|
brachytherapy |
-involves the insertion of sealed radioactive sources into a body cavity (intracavitary) or directly into body tissues (interstitial). -sealed internal radiation source -injecting radiation into organ -ex) prostate via rectom |
|
|
unsealed internal radiation source |
-injected intra- venously or administered by mouth. Iodine-131, which is given by mouth, is used in the treatment of thyroid cancer. -radioisotopes with short half life given systemically |
|
|
chemotherapy |
- Majorsystemic treatment option -Usedalone or in combination with surgery and/or radiation -Curativeor palliative -Drug(s)damage or kill cancer cells -Rapidlyproliferating and poorly differentiated cancer cells more likely to be killedthan slowly proliferating cells of normal tissue -given intravenously or orally -side effects: same as radiation |
|
|
hormone therapy |

-administration of drugs designed to disrupt the hormonal environment of cancer cells. -The theory behind the majority of hormone-based cancer treatments is to deprive the cancer cells of the hormonal sig- nals that otherwise would stimulate them to divide. -Pharmacologic methods focus largely on reducing circulating hormone levels or changing the hormone receptors so that they no longer respond to the hormone. -tamoxifen" estrogen antagonist; binds with receptor so estrogen can't bind--> estrogen no longer has affect --> great cancer tumor growth slows down - |
|
|
targeted therapy |
-drugs that interfere with specific molecules -more effective on cancer cells and less harmful to normal cells -growth signal inhibitors -angiogenesis inhibitors -apoptosis induceing inhibitors |
|
|
factors involved in the pathophysiology of asthma |
-genetic +atopy (early vs late phase) (predisposition to develop_ -enviormental +viruses +allergens +occupatioal exposure |
|
|
ANS control of airway smooth muscle |
-PNS +neuortransmitter:Ach +receptor: muscarinic receptor +causes: brochoconstriction +Smooth muscle also respondsdirectly to inflammatory mediators like histamine, which produce bronchoconstriction -SNS +neurotransmitter: Norepineprhrine (epi?) +beta 2 receptors +causes bronchodilation +beta adrenergic agonisits (albuterol) |
|
|
why frequent viral resp infections predispose people to asthma |
more likely for naive T cells to change into helper T 2 cells |