![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
79 Cards in this Set
- Front
- Back
|
Parenteral Routes |
any route other than gastrointestinal tract (most common form is injection) 1. Systemic Effect 2. Local Effect |
|
|
Systemic Effects |
those affecting the body as a whole (the entire system) Goal: distribute the medication through the circulatory system to the area requiring treatment |
|
|
Parenteral routes with Systemic Effects include |
1. Sublingual or buccal 2. Transcutaneous (transdermal) 3. Inhalations 4. Injections |
|
|
Local Effects |
limited to one particular part (location) of the body with very little, if any, effect on the rest of the body |
|
|
Medications in this category include |
1. Medications applied to skin for skin conditions (topical medications) 2. Drugs applied to the mucous membranes to treat the specific tissues 3. Medications instilled in the eyes for eye conditions 4. Medications instilled in the ears for ear conditions |
|
|
Sublingual Administration |
medication is placed under the tongue drug is absorbed directly into the circulation through the numerous blood vessels located in the mucosa of this area (More Common Route than Buccal) |
|
|
Buccal Administration |
medication is placed in the pouch of between the cheek and the gum at the back of the mouth |
|
|
Sublingual and Buccal Administration advantages |
- medications absorbed in this way are unaffected by stomach, intestines, or liver. - rapid, used frequently when a quick response is required. Ex: nitroglycerin to treat acute angina pectoris - constricted coronary blood vessels are usually dilated within a few minutes bringing quick relief from pain. |
|
|
Transcutaneous or Transdermal Systems |
deliver the medication to the body by absorption through the skin - absorption is slower, not effective in treatment of acute angina attacks Other methods: using a patch impregnated with particular medication applied to skin |
|
|
nitroglycerin (Nitro-Dur) patch |
patch is sometimes left in place for 72 h daily treats chronic angina |
|
|
Scopolamine (Transderm-Scop) |
patch is placed behind the ear and left in place up to 72 h as necessary to prevent motion sickness |
|
|
Fentanyl (Duragesic) |
applied on skin and changed every 72 h in management of chronic pain in patients requiring opiate analgesia |
|
|
Patient education on sublingual or buccal route |
1. hold the tablet in place with mouth closed until medication is absorbed 2. do not swallow the medication 3. Do not drink or take food until medication is completely absorbed |
|
|
Patient Education on applying transcutaneous systems of administration with nitroglycerin ointment |
1.squeeze prescribed amount of ointment onto dose-measuring application paper (Appli-Ruler), give tube slight twist to cut off ointment when reach correct marking 2. Do not touch ointment, wear gloves 3. fold Appli-Ruler lengthwise with ointment 4. flatten folded paper 5. Rotate sites for application, do not shave, clean dry free of irritation 6. wash hands 7. report and record any skin changes or complaints of headache |
|
|
Inhalation route |
used for chronic pulmonary conditions such as Asthma - patients may self-administer with MDI (metered-dose inhaler), DPI (dry-powder inhaler), or SVN (small-volume nebulizer), - physician may prescribe inhaled medication to be administered by trained personnel (respiratory therapists) |
|
|
Advantages of Inhalation Route |
1. Rapid action of the drug, with local effects within the respiratory tract 2. Potent drugs may be given in small amounts, minimizing the side effects 3. Convenience and comfort of the patient |
|
|
Disadvantages of Inhalation Therapy Route |
1. Requires cooperation of the patient in proper breathing techniques for effectiveness 2. Adverse systemic side effects may results rapidly because of extensive absorption capacity of lungs 3. Improperly administered, or too frequently administered, inhalations can lead to irritation of trachea or bronchi or bronchospasm 4. Asthmatic and chronic obstructive pulmonary disease (COPD) patients sometimes become dependent on an SVN, DPI, or MDI 5. If not cleaned properly the SVN can be a source of infection |
|
|
Transdermal Drug Delivery (dermal patches) used for |
prevention of angina pectoris prevention of motion sickness other patches available for analgesia estrogen replacement smoking cessation |
|
|
Metered-Dose Inhaler (MDI) |
deliver a measured (metered) dose via a propellant within a canister - portable and easy to use but proper administration by the patient is essential for effectiveness - spacer: may be added to act as a reservoir for aerosol, allow patient to first depress the canister then inhale |
|
|
Note |
use bronchodilator first then steroid if both are to be given at same time |
|
|
Important |
If using inhaled steroid (Asmanex, Flovent, Pulmicort or QVAR) rinse mouth out with mouthwash or water after using inhaler to reduce risk of developing oral fungal infection = Thrush |
|
|
Small-Volume nebulizer (SVN) |
Devices that create a fine mist of a drug solution using a gas source (aerosolization) usually a small air compressor in home care setting - aerosol is then inhaled via a mouthpiece or mask patient instructed to inhale slowly and deeply, perform short breath hold, exhale slowly. |
|
|
Possible adverse side effects and desired effects |
palpitations tremor nervousness dizziness headache nausea dry mouth irritated throat hoarseness coughing - notify physician if medication seem ineffective or if adverse side effects |
|
|
Dry-powder inhalers (DPIs) |
devices that deliver a drug in powder form into the lung with no propellant or external power source - patient must generate a sufficient inspiratory flow rate for the powder to aerosolize properly, DPIs are used for prophylactic treatment and not for acute breathing problems |
|
|
Advantages of DPIs |
it is small and relatively easy to use eliminates timing of inspiration technique problems encountered with an MDI - can be used in very cold environments (where propellants may not work as effective) |
|
|
Disadvantages of DPIs |
fewer drugs are available in powder form and patient must be able to generate a significant effort for proper drug delivery. |
|
|
Patient education on how to use DPI inhaler |
1. sit upright or stand 2. break dry powder capsule 3. remove upper dentures if loose 4. exhale slowly and completely 5. place mouthpiece between lips, forming a seal 6. Breathe in FAST and DEEP 7. Hold your breath for at least 5-10 sec 8. Exhale slowly through pursed lips` |
|
|
Intermittent Positive Pressure Breathing (IPPB) |
combines administration of an aerosol with a mechanical breather to assist patients who are unable to take a deep breath on their own - may be ordered by the physician - health care personnel (respiratory therapists or nurses are trained in the use of this equipment) |
|
|
cautions with IPPB therapy |
1. monitor vital signs closely, watching for a sudden drop in blood pressure, tachycardia and decreased or shallow respirations 2. observe for nausea or distended abdomen 3. watch for tremors or dizziness 4. assure the patient that coughing after the treatment is to be expected 5. record effectiveness of therapy and any side effects observed or reported by the patient |
|
|
Injections: Syringes has 3 parts |
1. Barrel: outer, hollow cylinder that holds the medication. Contains calibrations for measuring the quantity of medication 2. Plunger: inner, solid rod that fits snugly into the cylinder. Pulling back on the plunger allows solution to be drawn into the syringe. pushing forward on plunger ejects solution or air from syringe. 3. Tip: portion that holds the needle. larger syringes contain metal attachment at tip = Luer-Lok (locks needle in place) |
|
|
Needles: |
Hub: the flared end that fits on tip of syringe Shaft: long, hollow tube embedded in the hub |
|
|
Longer needles used for |
intramuscular (into muscle) injections * length of needle depends on size of patients shorter needles for children and thin adults, |
|
|
Gauge |
is the size of the lumen, or hole, through the needle or diameter of shaft - numbered in reverse order (thinner needle with smaller diameter = larger number) |
|
|
Size of gauge is determined by |
site of injection and viscosity of the solution (blood and oil require a thicker gauge needle) |
|
|
The 3 main types of syringes are used for injections - type used is determined by the medication and dosage |
1. Standard Syringe: 2. Tuberculin (TB) syringe 3. Insulin Syringe |
|
|
Standard Syringe |
Standard Syringe: used most frequently for subcutaneous or intramuscular injections, calibrated or marked in cubic centimeters (most commonly used is 3 mL or 2.5 mL) |
|
|
Tuberculin (TB) syringe |
Tuberculin (TB) syringe: used for intradermal injections of very small amounts of a substance (testing for tuberculosis or for allergies)- TB syringe also used for subcutaneous injections when small amount of medication (less than 1mL ordered) |
|
|
Insulin Syringe |
used only for injection of insulin and calibrated in units Standard Insulin Syringe size commonly used: U-100 = 100 units of insulin = 1 mL (count each calibration on one side as two units) Lo- Dose Insulin Syringes 50 unites and 30 units = counts as one unit. ALL INSULIN DOSAGES SHOULD BE DOUBLE-CHECKED BY 2 CAREGIVERS BEFORE ADMINISTRATION |
|
|
Drawing up Medications |
1. Wash hands 2. Assemble equipment 3. Check order using Six Rights of Medication Administration 4. If contained in Vial, remove protective cap. Wipe rubber diaphragm on top with alcohol wipe. 5. Seat needle securely on syringe by pressing firmly downward on top of the needle cover. Pull needle cover straight off. 6. Draw air into syringe equal to amount of solution you will be withdrawing from vial. insert needle into center of rubber and inject air into vial. Syringe fill proper level with solution no bubbles are present 7. Needle must be recapped carefully to maintain sterility and prevent needle sticks 8. If med is contained in an ampule, hold tip with alcohol wipe to protect your fingers and break open along the scored marking at neck |
|
|
Intradermal injections |
Are usually administered into the skin (epidermis) on the inner surface of the lower arm. (10-15 degrees) - a small amount (0.1 - 0.2 mL) is injected so close to the surface that a wheal or bubble is formed by the skin expanding. - using TB syringe 26 or 27 gauge, 3/8 inch needle |
|
|
Subcutaneous injection |
administered into fatty tissues on upper outer arm, front of the thigh, abdomen, or upper back tissue is pinched, and needle is held at 45-degree angle |
|
|
Intramuscular injections |
administered deep into large muscles (5 recommended site) 1. Dorsogluteal 2. Ventrogluteal 3. Deltoid 4. Vastuslateralis 5. Rectus femoris |
|
|
Dorsogluteal |
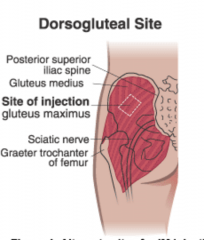
Upper outer quadrant of the buttock (preferred site for adults) |
|
|
Ventrogluteal |

Above and to the outside of the buttock area, on the hip |
|
|
Deltoid |
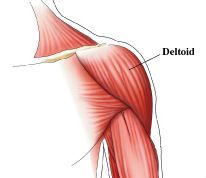
Upper outer arm above the axilla |
|
|
Vastuslateralis |

Front of the thigh toward the outside of the leg |
|
|
Rectus femoris |
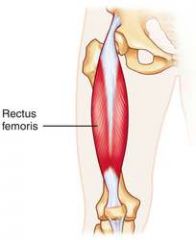
Front of the thigh toward the midline of the leg |
|
|
Advantages intramuscular route has two advantages over subcutaneous route |
1. a larger amount of solution can be administered (up to 3 mL or a max of 1 mL in children) 2. Absorption is more rapid because the muscle tissue is more vascular (i.e. contains many blood vessels) |
|
|
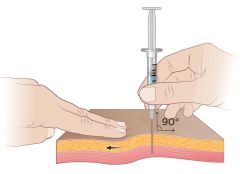
Length of needle varies with size of patient - needle must be long enough to go through the subcutaneous tissue into the muscle |
child or very thin, emaciated adult = 1 inch most adults = 1.5 inch obese person = 2 inch
*needle is inserted at a 90 degree angle with skin spread taut |
|
|
Follow these steps in selecting the site |
Dorsogluteal Site Ventrogluteal site |
|
|
Dorsogluteal Site for IM injection |
most commonly used for adults, but not for children under 3 years old -position patient flat on stomach (prone) with toes pointed inward or on the side with upper leg flexed. Two bony prominences = posterior superior iliac spine and greater trochanter of femur - injection given above and to outside of the line, high enough to avoid the sciatic nerve and major blood vessels |
|
|
Ventrogluteal Site for IM injection |
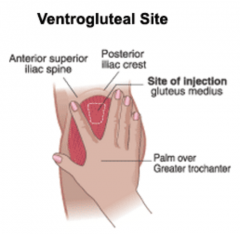
Can be used for all patients - position patient on back or side - identify site by placing palm of hand on patient's greater trochanter. place index finger on anterior superior iliac spin and the middle finger on iliac crest. Injection is made into the center of the V formed between the index and middle finger |
|
|
Deltoid Site |
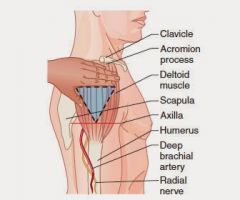
Seldom used because the muscle is smaller and is close to radial nerve - max solution used is 1 mL, shorter needle (1 inch is used) - caution: must avoid clavicle, humerus, acromium, brachial vein and artery and radial nerve - draw line across arm at level of armpit - injection is made above this line and below the acromium on the outer aspect of the arm |
|
|
Vastus Lateralis site |
located on anterior lateral thigh, preferred for infants (muscle is most developed for children under 3 years old) - identify the mid portion on side of thigh by measuring one hand breadth above the knee and one hand breadth below the greater trochanter (area between is site of injection) |
|
|
Rectus Femoris Site |
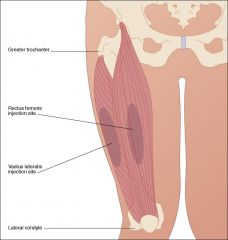
located just medial to the vastuslaterals, but does not cross the midline. - preferred site for self-injection because of accessibility - located in the same way as vastuslateralis - if muscle not developed, injection at site may be painful. |
|
|
Z- Track method injection |
used for injections that are irritating to the tissue, such as iron dextran, hydroxyzine, or cefazolin = dorsogluteal is the site for this type of intramuscular injection 1. skin and subcutaneous tissue pulled to one side and held there 2. needle is placed in muscle 3. Z-track sealed when tissue released inject at 90 degrees |
|
|
Subcutaneous Injection |
25 gauge |
|
|
Intravenous Injections |
19-21 gauge 1.5 inch needle |
|
|
Allergy Testing (intradermal) |
26 or 27 gauge, 3/8 inch needle |
|
|
Intramuscular Injection |
18 gauge |
|
|
What equipment is used for injections? |
Syringes: barrel, plunger, tip Needles: hub, shaft, tip |
|
|
Chapter 10 |
Poison Control |
|
|
Poison |
a substance taken into the body by ingestion, inhalation, injection or absorption that interferes with normal physiological functions |
|
|
Most common type of poisoning |
ingestion or swallowing (highest risk: children 1-5 years old) |
|
|
Best policy if poisoning is suspected |
contact Poison Control Center directly 1-800-222-1222 or through an emergency care facility |
|
|
In early 2004, the American Academy of Pediatrics (AAP) |
issued a policy statement on poison treatment in the home - recommended against keeping ipecac in home, and dispose safely. outcomes failed to justify its effectiveness adverse effects such as persistent vomiting could interfere with treatment - widespread abuse by people with anorexia and bulimia |
|
|
Emetic |
agent that induces vomiting (ex: ipecac syrup) |
|
|
Antidotes |
substances that neutralizes poison or toxic chemicals |
|
|
Symptomatic treatment for poisoning by inhalation |
fresh air oxygen CPR if indicated |
|
|
incomplete combustion of fires can produce |
carbon monoxide - poisoning can quickly rob tissues of vital oxygen and high-percentage oxygen therapy (hyperbaric oxygen) or even under pressure. |
|
|
Treatment for external poisoning of the eye |
flushed from skin for 20 minutes or eyes for 30 mins with a continuous stream of water |
|
|
What to do after? |
Patient should be transported to an emergency care facility for further treatment as required (may require administration of anecdote) |
|
|
Treatment for poisoning by insect sting |
treat by cleansing the area immediately removing the stinger and applying an icepack to the site of the sting - if patient is allergic, watch closely for possible anaphylactic reaction - CPR and administration of epinephrine and corticosteroids may be required |
|
|
For snakebites |
do not apply ice or apply a tourniquet to a snakebite - venom is very irritating and may cause sloughing of the tissues - keep patient quiet to slow circulation transport to emergency facility for antivenom injection |
|
|
Most common sources for poisoning in children under six are |
cosmetics and personal care products |
|
|
Poisoning in older adults |
overdoses of medication can result in toxicity, with symptoms of confusion, dizziness, weakness, lethargy, ataxia, tremors, or cardiac irregularities. |
|
|
Toxic reactions from medications taken by older adults can possible result from |
1. slower metabolism, impaired circulation, decreased excretion, causing medication to remain in body longer and build up dangerous levels 2. Wrong dosage caused by impaired vision or poor memory 3. Interactions when many different medications are taken and OTC or herbal remedies are self-administered with inadequate supervision |
|
|
4 different ways Poisons can be taken into the body |
Ingestion Inhalation External poison of skin or eyes Sting and Snakebite |
|
|
Gastric lavage is contraindicated when patient has ingested |
corrosive substances (mineral acids or caustic alkalis,- carbolic acid, ammonia, drain cleaners, oven cleaners, dishwasher detergent) volatile petroleum products (gasoline, kerosene, lighter fluid and benzene) convulsants (strychnine, or iodine) |