![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
Tell the story of the quadruplets |
-quads in 1930s all survived -3/4 diagnosed schizo, 4th had symptoms -father had symptoms, mom was nurse -pseudonym NIMH named them n, i, m, h -Genain last name, greek for dire birth. |
|
|
For identical twins, the chance of both twins developing schizophrenia is about __%. For identical quads, the odds of all four developing schizophrenia are about ____in ___, or ___% So a further prompt question is: how did almost all 4 get schizo from the quads if the genetic probability is lower than a pair |
48 |
|
|
Schizophrenia definition |
A psychological disorder characterized by psychotic symptoms that significantly affect emotions, behavior, and mental processes and mental contents. |
|
|
DSM-5 lists schizophrenia as a single disorder vs. Schizophrenia Spectrum and Psychotic Disorders chapter conceptualization why would it be considered a spectrum? |
Research findings suggest that each variant of schizophrenia has different symptoms, causes, course of development, and, possibly, response to treatments. |
|
|
TABLE 12.1 • DSM-5 Diagnostic Criteria for Schizophrenia |
- |
|
|
The criteria for schizophrenia in DSM-5 fall into two clusters: |
positive symptoms, which consist of delusions and hallucinations and disorganized speech and behavior; and
negative symptoms, which consist of the absence or reduction of normal mental processes, mental contents, feelings, or behaviors, including speech, emotional expressiveness, and/or movement. remember it as if its like classical/operant conditioning, i.e. pos applies, neg removes |
|
|
Positive symptoms-def |
Symptoms of schizophrenia that are characterized by thepresence of abnormal or distorted mental processes, mental contents, or behaviors.
hallucinations (distortions of perception), delusions (distortions of thought), disorganized speech, and disorganized behavior. |
|
|
Hallucinations most common in schizophrenics? why? |
Sensations that are so vivid that the perceived objects or events seem real, although they are not. Hallucinations can occur in any of the five senses.
auditory hallucinations—specifically, hearing voices—are the most common type experienced by people with schizophrenia difficulty distinguishing between verbal information that is internally generated and verbal information that is externally generated . People with schizophrenia are also more likely to (mis)attribute their own internal conversations to another person |
|
|
Delusions + themes x4 |
Persistent false beliefs that are held despite evidence that the beliefs are incorrect or exaggerate reality.
Persecutory delusions involve the theme of being persecuted by others. delusions of control revolve around the belief that the person is being controlled by other people (or aliens), who literally put thoughts into his or her head, called thought insertion grandiose delusions- believing oneself to be significantly more powerful, knowledgeable, or capable than is actually the case referential delusions: the belief that external events have special meaning for the person. |
|
|
Disorganized Speech x2types |
s. One type of disorganized speech is word salad, which is a random stream of seemingly unconnected words. For example, a patient might say something like, “Pots dog small is tabled.” Another type of disorganized speech involves many neologisms, or words that the patient makes up: That’s wish-bell. Double vision. It’s like walking across a person’s eye and reflecting personality. |
|
|
grossly disorganized or abnormal psychomotor behavior; definition x1type |
The term psychomotor refers to intentional movements, and in this case such behavior is so unfocused and disconnected from a goal that the person cannot successfully accomplish a basic task, or the behavior is inappropriate in the situation. catatonia (also referred to as catatonic behavior), which occurs when a person does not respond to the environment or remains in an odd posture or position, with rigid muscles, for hours |
|

wtf is she doing |
catatonia |
|
|
Negative symptoms definition
x4 types |
Symptoms of schizophrenia that are characterized by the absence or reduction of normal mental processes, mental contents, or behaviors. diminished emotional expression and avolition. Alogia— anhedonia, asociality |
|
|
diminished emotional expression (sometimes referred to as ___________), |
flat affect - occurs when a person does not display a large range of emotion, sometimes speaking robotically and seeming emotionally neutral. Such people may not express or convey much information through their facial expressions, body language, tone of voice, and they tend to refrain from making eye contact |
|
|
Avolition |
A negative symptom of schizophrenia marked by difficulty initiating or following through with activities.
|
|
|
Alogia— |
speaking less than do most other people. A person with alogia will take a while to muster the mental effort necessary to respond to a question.
|
|
|
Anhedonia—
|
a diminished ability to experience pleasure (see Chapter 5).
|
|
|
Asociality—
|
disinterest in social interactions.
|
|
|
Specific cognitive deficits are found in________, ____________, ___________, and they arise in most people with schizophrenia. examples?? |
attention, -- distinguishing relevant from irrelevant stimuli working memory, People with schizophrenia do not organize information effectively, which indicates that their working memories are impaired. executive functioning--difficulty performing household chores that required multiple steps,.. messes up general functioning |
|
|
cognitive deficit onset? course? |
do not necessarily make their first appearance at the same time that the positive and negative symptoms of schizophrenia first emerge often persist after the positive and negative symptoms improve tho |
|
|
Limitations of DSM-5 Criteria x2 |
specific criteria -Absence of Focus on Cognitive Deficits and of the grouping of positive and negative symptoms (Fauman, 2006; Green, 2001). |
|
|
DSM-5 set of positive symptoms includes disorganized speech and grossly disorganized psychomotor behavior (see TABLE 12.1), research suggests that these two symptoms together form an important cluster, independent of hallucinations and delusions. Example?? why? |
This cluster apparently reflects specific types of underlying cognitive deficits, which clearly contribute to disorganized thinking. For instance, cognitive deficits can cause thoughts to skip from one topic to another, topics that are related to each other only tangentially if at all. (This process is referred to as a loosening of associations.) THUS disorganized speech arises from disorganized thinking. dsm5 does not take into account cognition |
|
|
other factors of underlying cognitive deficits?? x4, think about the current symptoms and how they might be related to cognition. |
The disorganized behavior, asociality, and poor social skills, and perhaps avolition, all are indicators of underlying cognitive deficits |
|
|
Deficit/Nondeficit Subtypes why are there deficits?? |
deficit subtype, a patient must have severe neurocognitive deficits in attention, memory, and executive functioning, as well as the positive and negative symptoms that are manifestations of these deficits, such as disorganized speech and grossly disorganized psychomotor behavior. neuroimaging results show that people with the deficit subtype of schizophrenia (but not those who have the nondeficit subtype) have abnormalities in their “white matter tracts”—sets of axons that connect neurons (Voineskos et al., 2013). (They are white because they are covered with the fatty insulator substance myelin.) nondeficit subtype, a patient must have positive symptoms, such as hallucinations and delusions, in conjunction with relatively intact cognitive functioning. |
|
|
Psychotic mania is distinguished from schizophrenia by... |
the presence of other symptoms of mania—such as pressured speech or little need for sleep.
|
|
|
depression vs. neg symptoms of schizo |
In general, people with schizophrenia but not depression do not have other symptoms of depression, such as changes in weight or sleep or feelings of worthlessness and inappropriate guilt (American Psychiatric Association, 2013). Of course, people with schizophrenia may develop comorbid disorders, such as depression. |
|
|
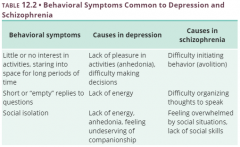
Table 12.2 depression similar behavior symptoms?? x2 cause in depression? x3 cause in schizo? x2 |
|
|
|
substance-related disorders & schizo?? |
substance-related disorders can lead to delusions persecutory delusions that arise from chronic use of stimulants. Substances (and withdrawal from them) can also induce hallucinations, such as the tactile hallucinations that can arise with cocaine use (e.g., the feeling that bugs are crawling over a person’s arms). formication |
|
|
4 other psychotic disorders outside schizophrenia?? |
Schizophreniform
\ Brief psychotic disorder / Schizoaffective disorder / delusional disorder |
|
|
Schizophreniformdisorder. |
A psychotic disorder characterized by symptoms that meet all the criteria for schizophrenia except that the symptoms have been present for only 1–6 months, and daily functioning may or may not have declined over that period of time
-" 'having the form of'" ->> suffix iform |
|
|
Brief psychotic disorder
|
A psychotic disorder characterized by the sudden onset of positive or disorganized symptoms that last between 1 day and 1 month and are followed by full recovery. For this diagnosis, no negative symptoms should be present during the episode he or she also has an increased risk of suicide during the episode. Once recovered, people who had this disorder have a good prognosis for full recovery |
|
|
Schizoaffective disorder |
A psychotic disorder characterized by the presence of both schizophrenia and a depressive or manic episode. |
|
|
delusional disorder x5 types |
psychotic disorder characterized by the presence of delusions that have persisted for more than 1 month. ONLY delusion. Erotomanic. The belief that another person is in love with the patient. This delusion usually focuses on romantic or spiritual union rather than sexual attraction. Grandiose. The belief that the patient has a great (but unrecognized) ability, talent, or achievement. Persecutory. The belief that the patient is being spied on, drugged, harassed, or otherwise conspired against. Somatic. The false belief that something is wrong with the body (such as insects on the skin) and these delusions are not considered a symptom of another psychological disorder, such as obsessive-compulsive disorder (Chapter 7) or body dysmorphic disorder (Chapter 7). Jealous. The belief that the patient’s romantic partner is unfaithful. This belief is based on tiny amounts of “evidence,” such as the partner’s arriving home a few minutes late. |
|

who are these 2 skids?, |
https://en.wikipedia.org/wiki/Brian_David_Mitchell delusional disorder One extremely unusual and rare presentation of delusional symptoms involves a shared delusion among two or more people (sometimes referred to as folie à deux, which is French for “paired madness”) The person who had the disorder at the outset is referred to as the primary person and is usually diagnosed with schizophrenia or delusional disorder. Th |
|
|
schizotypal personality disorder |
A person with schizotypal personality disorder may have very few if any close friends, may feel that he or she doesn’t fit in, and may experience social anxiety. Schizotypal personality disorder, unlike schizophrenia, does not involve psychotic symptoms. |
|
|
Attenuated psychosis syndrome |
is a diagnosis that was proposed for inclusion in DSM-5 but that did not make it in. This condition is defined by “attenuated” (that is, reduced or weakened) psychotic symptoms of psychosis. For example, rather than paranoid delusions, someone may be generally mistrustful, and rather than hearing voices, someone may hear rumblings or murmurs. used to signal, ...psychotic risk syndrome is another name for it |
|
|
prevalence of schizophrenia? how many are homeless? hospital? jail? live independently? |
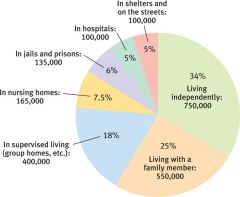
1% 5% 5% 6% 34% |
|
|
comorbidity, how many have another disorder? 3most common? **** |
90% Mood disorders. Approximately 50% of people with schizophrenia also have some type of mood disorder, most commonly depression (Buckley et al., 2009; Sands & Harrow, 1999). As noted earlier, according to DSM-5, some of these people may haveschizoaffective disorder. Anxiety disorder. Almost half of people with schizophrenia also have panic attacks (Goodwin et al., 2002) and anxiety disorders (Cosoff & Hafner, 1998). Substance use disorders. Up to 60% of people with schizophrenia have a substance abuse problem that is not related to tobacco (Swartz et al., 2006). Moreover, 90% of those with schizophrenia smoke cigarettes (Regier et al., 1990), and they tend to inhale more deeply than do other smokers (Tidey et al., 2005) |
|
|
Describe Schizophrenias course |
Typically, schizophrenia develops in phases. In the premorbid phase, before symptoms develop, some people may display personality characteristics or cognitive deficits that later evolve into negative symptoms the prodromal phase, which is between the onset of symptoms and the time when the minimum criteria for a disorder are met. In the active phase, a person has full-blown positive (and possibly negative) symptoms that meet the criteria for the disorder. If the positive symptoms have subsided but negative symptoms persist, the full criteria for schizophrenia are no longer met; the person can be said to be in the residual phase, which indicates that there is a residue of (negative) symptoms but the pronounced positive symptoms have faded away. premorbid-acting weird prodromal-symptoms onset active phase- full blown residual phase- no pos symptoms, residue from neg |
|
|
Schizophrenias Gender Differences |
men 1.4 ratio to women +men earlier onset -women have fewer neg and more mood symptoms -less likely to have substance abuse problems or to exhibit suicidal or violent behavior (Seeman, 2000). -Moreover, women generally function at higher levels before their illness develops. |
|
|
Culture x2 |
First, across various countries, schizophrenia is more common among people in urban areas and lower socioeconomic classes than among people in rural areas and higher socioeconomic classes -Blacks are twice as likely as Whites or Latinos to be diagnosed with schizophrenia Second, people with schizophrenia in non-Western countries are generally better able to function i.e. collectivism |
|
|
Prognosis of schizophrenia?? |
In general, the long-term prognosis for schizophrenia follows the rule of thirds: one third of patients improve significantly; one third basically stay the same, having episodic relapses and some permanent deficits in functioning, but are able to hold a “sheltered” job—a job designed for people with mild to moderate disabilities; and one third become chronically and severely disabled by their illness. |
|
|
TABLE 12.6 • Factors Associated With a Better Prognosis for People With Schizophrenia
Elyn Saks=example |
People with schizophrenia who significantly improve often have one or more of the following characteristics: They functioned at a relatively high level before their first episode. The symptoms had a sudden onset. They developed symptoms later in life. They have a family history of mood disorders, not schizophrenia. They have symptoms of paranoia or the nondeficit subtype, with relatively good cognitive functioning. They have fewer negative symptoms. They are aware of their symptoms and recognize that the symptoms are caused by an illness. They are women. |
|
|
suicide & schizophrenia |
10-15% kill themselves paranoia symptoms=more |
|
|
describe patients at risk for committing suicide are |
patients at risk for committing suicide are those who are most likely to be aware of their symptoms: They have relatively few negative symptoms but pronounced positive symptoms;they tend to be highly intelligent, have career goals, are aware of their deterioration, and have a pattern of relapsing and then getting better, with many episodes; and—like other people who die by suicide—they are more likely to be male than female |
|
|
Violence and schizo? victims of violence? statistic |
Risk factors associated with violent behavior include being male, having comorbid substance abuse, not taking medication, and has engaged in criminal behavior or having had psychopathic tendencies before schizophrenia developed 20% |
|
|
victims of violence?? @risk factors |
Those who were more disorganized and functioned less well were more likely to have been victimized (Chapple et al., 2004), perhaps because their impaired functioning made them easier “marks” for perpetrators. |
|
|
what brain structures are involved with schizophrenics?? |
- |
|
|
The most striking example of a structural abnormality in the brains of people with schizophrenia is ... |
enlarged ventricles, which are cavities in the center of the brain that are filled with cerebrospinal fluid
people who later develop schizophrenia have brains that are smaller than normal even before they develop the disorder. research suggests that schizophrenia causes parts of the brain to shrink |
|
|
frontal lobe hypothesis |
Research results suggest that an excess of such pruning takes place during adolescence for people who develop schizophrenia: Too many of the neural connections in the frontal lobes are eliminated, which may account for some of the neurocognitive deficits that typically accompany this disorder |
|
|
Impaired Temporal Lobe and Thalamus? cause? implications ? |
Enlarged ventricles are associated with decreased size of the temporal lobes. The thalamus, which transmits sensory information to other parts of the brain, also appears to be smaller and to function abnormally in people with schizophrenia temporal lobes process auditory information, some aspects of language, and visual recognition (Levitan et al., 1999; Sanfilipo et al., 2002). Abnormal functioning of the temporal lobes may underlie some positive symptoms, notably auditory hallucinations, Abnormal functioning of the thalamus is associated with difficulties in focusing attention, in distinguishing relevant from irrelevant stimuli, and in particular types of memory difficulties, |
|
|
Abnormal Hippocampus? |
smaller in people with schizophrenia and their first-degree relatives (parents and siblings) than in control participants (Seidman et al., 2002; |
|
|
Interactions Among Brain Areas hypothesis |
Some researchers propose that schizophrenia arises from disrupted interactions among the frontal lobes, the thalamus, and the cerebellum— According to this theory, the thalamus fails to screen out sensory information, which overwhelms subsequent processing—and thus the form and content of the person’s thoughts become confused. |
|
|
Possible Causes of Brain Abnormalities x3 |
maternal malnourishment -- during pregnancy, particularly during the first trimester maternal illness during the 6th month of pregnancy. 2nd trimester -oxygen deprivation, |
|
|
maternal illness during the 6th month of pregnancy. why???
|
During fetal development, neurons travel to their final destination in the brain and establish connections with other neurons (in a process called cell migration). If the mother catches the flu or another viral infection in the second trimester, this may disrupt cell migration in the developing fetus’s brain, which causes some neurons to fall short of their intended destinations. Because the neurons are not properly positioned, they form different connections than they would have formed if they had been in the correct locations—leading to abnormal neural communication (Brown, Begg, et al., 2004; Green, 2001; McGlashan & Hoffman, 2000). In general, an immune challenge to the developing fetus in turn can affect brain development (Meyer, 2013; Watanabe et al., 2010). ill-migration-2nd tri- wrong location - abnormal communication |
|
|
Biological marker . x3 examples |
A neurological, bodily, or behavioral characteristic that distinguishes people with a psychological disorder (or a first-degree relative with the disorder) from those without the disorder
smooth pursuit eye movements sensory gating involuntary movements-- |
|
|
smooth pursuit eye movements
|
difficulty maintaining smooth, continuous eye movements when tracking a light as it moves across the visual field; |
|
|
sensory gating
|
which is assessed as follows: Participants hear two clicks, one immediately after the other. Normally, the brain responds less strongly to the second click than to the first. However, people with schizophrenia and their first-degree relatives don’t show the normal large drop in the brain’s response to the second click. This has been interpreted as a manifestation of the difficulties that people with schizophrenia can have in filtering out unimportant stimuli. |
|
|
involuntary movements-- how was it discovered? evident @ what ages?? doing what ? |
watching home movies of children later diagnosed such as writhing or excessive movements of the tongue, lips, or arms. This tendency for involuntary movement was particularly evident from birth to age 2 but could be seen even through adolescence in people who later developed the disorder (Walker et al., 1994). Moreover, those who displayed more severe movements of this type later developed more severe symptoms of schizophrenia (Neumann & Walker, 1996). |
|
|
Schizophrenia is likely to involve a complex interplay of many brain systems, neurotransmitters, and hormones. |
Dopamine, Serotonin and Glutamate, Stress and Cortisol, |
|
|
dopamine hypothesis proof? |
proposes that an overproduction of dopamine or an increase in the number or sensitivity of dopamine receptors is responsible for schizophrenia.
According to this hypothesis, the excess dopamine or extra sensitivity to this neurotransmitter triggers a flood of unrelated thoughts, feelings, and perceptions. Delusions are then attempts to organize these disconnected events into a coherent, understandable experience neuroimaging studies of people with schizophrenia have found abnormally low numbers of dopamine receptors in their frontal lobes (Okubo et al., 1997), as well as increased production of dopamine in the striatum (parts of the basal ganglia that produce dopamine; |
|
|
Medications that affect __________ levels can decrease both positive and negative symptoms in people with schizophrenia. |
serotonin |
|
|
glutamate? |
Studies have found unusually high levels of glutamate in people with schizophrenia, particularly in the frontal lobe (Abbott & Bustillo, 2006; van Elst et al., 2005); such an excess of glutamate may disrupt the timing of neural activation in the frontal lobe, which in turn may impair cognitive activities |
|
|
Stress and Cortisol |
children who are at risk for developing schizophrenia react more strongly to stress, and their baseline levels of cortisol are higher than those of other children . Even after adolescence, people with schizophrenia have higher levels of stress-related hormones, including cortisol The relationship between cortisol and schizophrenia is supported by research indicating that anti-inflammatory medications (such as aspirin or other types of drugs referred to as COX-2 inhibitors), which indirectly reduce the levels of cortisol, reduce the symptoms of schizophrenia |
|
|
Effects of Estrogen proof? x2 |
estrogen protection hypothesis According to this hypothesis, the hormone estrogen, which is present at higher levels in women than in men, protects against symptoms of schizophrenia via its effects on serotonin and dopamine. This protection may explain why women typically develop the disorder later in life than do men. Evidence for the estrogen protection hypothesis comes from two sources. One is the finding that women with schizophrenia who had higher levels of estrogen also had better cognitive functioning (Hoff et al., 2001). The other is the finding that constant doses of estrogen provided by a skin patch (in addition to antipsychotic medication) reduced the positive symptoms of women with severe schizophrenia more than did antipsychotic medication without supplementary estrogen |
|
|
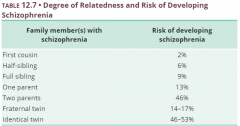
Genetics? |
More than 85% of people who have one parent or one sibling (who is not a twin) with the disorder do not go on to develop it themselves ... 15% do. Kinda wording it differently than any other description of mhd's. The more genes a person shares with a relative who has schizophrenia, the higher the risk |
|
|
Table 12.7 First cousin Half-sibling Full sibling One parent Two parents Fraternal twin Identical twin |
|
|
|
what if 1 schizo twin has kids vs. the other twin having kids? whats the probability? |
same for both, based on predisposition of genetics. Both share the same predisposed genetics, 1 just developed it by chance. |
|
|
adoption study |
the children whose biological mothers had schizophrenia and whose adoptive families were dysfunctional were much more likely to develop schizophrenia than were the children whose biological mothers had schizophrenia but whose adoptive families were not dysfunctional. |
|
|
cognitive problems psychological traits x2 |
difficulties with attention.—specifically in being able to focus on relevant stimuli and ignore irrelevant stimuli—occur even when the person is taking medication and isn’t psychotic
often don’t realize that they are having unusual experiences or behaving abnormally; this inability is referred to as a lack of insight. |
|
|
neg consequences of lack of insight |
Thus, they are unaware of their disorder or the specific problems it creates for themselves and others (Amador & Gorman, 1998) and see no need for treatment |
|
|
Theory of mind
|
A theory about other people’s mental states (their beliefs, desires, and feelings) that allows a person to predict how other people will react in a given situation. |
|
|
Stressful Environments |
children born to a parent with schizophrenia are more likely to develop schizophrenia as adults if they were raised in an institution than if they were raised by the parent with schizophrenia (Mednick et al., 1998). |
|
|
High expressed emotion (high EE) ethnic differences??? |
A family interaction style characterized by hostility, unnecessary criticism, or emotional overinvolvement.
for example, by frequently criticizing or nagging the patient to change his or her behavior Researchers have also discovered ethnic differences in how patients perceive critical and intrusive family behaviors. Among Black American families, for instance, behaviors by family members that focus on problem solving are associated with a better outcome for the person with schizophrenia, perhaps because such behaviors are interpreted as reflecting caring and concern (Rosenfarb et al., 2006). Thus, what is important is not the family behavior in and of itself but how such behavior is perceived and interpreted by family members. |
|
|
Immigration ... specifically who? |
This higher rate of schizophrenia among immigrants occurs among people who have left a wide range of countries and among people who find new homes in a range of European countries. In fact, one meta-analysis found that being an immigrant was the second largest risk factor for schizophrenia, after a family history of this disorder may arise from the stresses of immigration, socioeconomic disadvantage, and racism Researchers have sought to rule out potential confounds such as illness or nutrition, and have found that such factors do not explain the higher risk of schizophrenia among immigrants. |
|
|
Economic Factors two possible explanations for this association |
A disproportionately large number of people with schizophrenia live in urban areas and among lower economic classes social selection and social causation |
|
|
Social selection hypothesis |
The hypothesis that people who are mentally ill “drift” to a lower socioeconomic level because of their impairments; also referred to as social drift.
|
|
|
Social causation hypothesis |
The hypothesis that the daily stressors of urban life, especially as experienced by people in a lower socioeconomic class, trigger mental illness in those who are vulnerable
|
|
|
Cultural Factors: Recovery in Different Countries |
Collectivist cultures may more readily help people with schizophrenia be a part of the community at whatever level is possible. And in fact, people with schizophrenia in collectivist cultures, such as those of Japan, Hong Kong, and Singapore, have a more favorable course and prognosis than people with schizophrenia in individualist cultures such as the United States |
|
|
The collectivist characteristics of a culture may help a patient to recover for several reasons. Consider that people in collectivist countries may: |
--be more tolerant of people with schizophrenia and therefore less likely to be critical, hostile, and controlling toward them. --elevate the importance of community and, in so doing, provide a social norm that creates more support for people with schizophrenia and their families. -- have higher expectations of people with schizophrenia—believing that such people can play a functional role in society—and these expectations become a self-fulfilling prophecy |
|
|
treatment steps |
STEP 1: When the patient is actively psychotic, first reduce the positive symptoms. STEP 2: Reduce the negative symptoms. STEP 3: Improve neurocognitive functioning. STEP 4: Reduce the person’s disability and increase his or her ability to function in the world. |
|
|
At present, interventions targeting neurological factors generally focus on.... |
reducing positive and negative symptoms
+cognitive |
|
|
Medication x2 types |
Traditional Antipsychotics |
|
|
Traditional Antipsychotics purpose? mechanism? side effects? effectiveness? how long till it activates? |
Thorazine (chlorpromazine) and other similar antipsychotics are dopamine antagonists, which effectively block the action of dopamine positive symptoms—hallucinations and delusions—diminish in approximately 75–80% of people traditional antipsychotics quickly sedate patients; above and beyond such sedation, psychotic symptoms start to improve anywhere from 5 days to 6 weeks after the patient begins to take the medication tardive dyskinesia Other side effects of traditional antipsychotics include tremors, weight gain, and a sense of physical restlessness. |
|
|
tardive dyskinesia ? |
An enduring side effect of traditional antipsychotic medications that produces involuntary lip smacking and odd facial contortions as well as other movement-related symptoms. |
|
|
Atypical Antipsychotics mechanism? side effects? |
(also referred to as second-generation antipsychotics) affect dopamine and serotonin. Examples of atypical antipsychotics include Risperdal (risperidone), Zyprexa (olanzapine), and Seroquel (quetiapine). Side effects include changes in metabolism that cause significant weight gain and increased risk of heart problems In addition, atypical antipsychotics, like traditional antipsychotics, sometimes cause tardive dyskinesia |
|
|
problems with patients taking meds? why? |
noncompliance. Many people who stop taking their medication—whether in consultation with their doctor or not—cite significant unpleasant side effects as the main reason |
|
|
Discontinuing Medication |
patients stop taking their medication (up to two thirds in one study; Lieberman et al., 2005), When people with schizophrenia discontinue their medication, they are more likely to relapse One study found that among those who were stable for over 1 year and then stopped taking their medication, 78% had symptoms return within 1 year after that, and 96% had symptoms return after 2 years ( |
|
|
ECT and TMS |
ECT may reduce symptoms, but its effects are short lived; furthermore, “maintenance” ECT—that is, regular although less frequent treatments—may be necessary for long-term improvement TMS) appears to decrease hallucinations, at least in the short term |
|
|
Treatments for schizophrenia that target psychological factors address three of the four general treatment steps
|
; they (1) reduce psychotic symptoms through cognitive-behavior therapy (CBT); (2) reduce negative symptoms of schizophrenia through CBT; and (3) improve neurocognitive functioning (and quality of life) through psychoeducation and motivational enhancement |
|
|
Cognitive-Behavior Therapy x4 |
learn to distinguish hallucinatory voices from people actually speaking, highlight the importance of taking effective medications, address issues that interfere with compliance, and develop more effective coping strategies. When a therapist uses CBT to address problems arising from delusions, he or she does not try to challenge the delusions themselves but instead tries to help the patient move forward in life, despite these beliefs. |
|
|
Treating Comorbid Substance Abuse?? |
Motivational Enhancement patients who receive motivational enhancement therapy develop their own goals, and then clinicians help them meet those goals. |
|
|
Targeting Social Factors in Treating Schizophrenia |
Family Education and Therapy Group Therapy: Social Skills Training Inpatient Treatment Community-Based Interventions |
|
|
Treatments that target social factors address three of the four general treatment steps: |
They identify early warning signs of positive and negative symptoms through family education and therapy; when necessary, such treatments involve hospitalizing people who cannot care for themselves or are at high risk of harming themselves or others.
|
|
|
Family Education and Therapy |
Psychoeducation for family members can provide practical information about the illness and its consequences, how to recognize early signs of relapse, how to recognize side effects of medications, and how to manage crises that may arise family-based treatments may provide emotional support for family members (Dixon et al., 2000). Moreover, family therapy can create more adaptive family interaction patterns i.e. Family therapy can also help high EE families |
|
|
Group Therapy: Social Skills Training goals ? how? cognitive techniques vs. behavior? |
Social skills training usually occurs in a group setting, and its goals include learning to “read” other people’s behaviors, learning what behaviors are expected in particular situations, and responding to others in a more adaptive way. Social skills training teaches these skills by breaking complex social behaviors into their components: maintaining eye contact when speaking to others, taking turns speaking, learning to adjust how loudly or softly to speak in different situations, and learning how to behave when meeting someone new. The leader and members of a group take turns role-playing these different elements of social interaction. cognitive techniques focus on group members’ irrational beliefs about themselves, their knowledge of social conventions, the beliefs that underlie their interactions with other people, and their ideas about what others may think |
|
|
Inpatient Treatment |
. A short-term hospital stay may be required when someone is having an acute schizophrenic episode or is suicidal or violent. The goal is to reduce symptoms and stabilize the patient. Long-term hospitalization may occur only when treatments have not significantly reduced symptoms and the patient needs full-time intensive care. |
|
|
. Community care |
(also known asassertive community treatment) programs allow mental health staff to visit patients in their homes at any time of the day or night (Mueser, Bond, et al., 1998). Patients who receive such community care report greater satisfaction with their care; however, such treatment may not necessarily lead to better outcomes
|
|
|
Residential Settings |
well enough not to need hospitalization but are still sufficiently impaired that they cannot live independently or with family members. Alternative housing for such people includes a variety of supervised residential settings. Some of these patients live in highly supervised housing, in which a small number of people live with a staff member. Residents take turns shopping for and making meals. They also have household chores and attend house meetings to work out the normal annoyances of group living halfway house for schizos |
|
|
Vocational Rehabilitation |
assist injured workers to return to work as soon as possible. |
|
|
supported employment programs |
, which place people in regular work settings and provide an onsite job coach to help them adjust to the demands of the job itself and the social interactions involved in having a job
. Examples of supported employment jobs might include work in a warehouse, packaging items for shipment or restocking items in an office or a store |
|
|
sheltered employment, |
working in settings that are specifically designed for people with emotional or intellectual problems who cannot hold a regular job. For example, people in such programs may work in a hospital coffee shop or create craft items that are sold in shops.
|
|
|
What predicts how well a patient with schizophrenia can live and work in the world? |
Researchers have found that a person’s ability to live and perhaps work outside a hospital is associated with a specific cognitive function: his or her ability to use working memory (
|