![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
153 Cards in this Set
- Front
- Back
|
abdominal pain, N/V in an elderly woman w/diabetes 1st step? |
ECG |
|
|
MI Lab Tests 1. Sensitive for new MI 2. Sensitive for re-occlusion < 10 days from a previous MI |
Tropoin CK-MB |
|
|
Ischemic chest pain w/exertion Normal EKG Next step? |
Exercise stress test |
|
|
Most common cause of cardiac arrest in MI |
Reentrant ventricular arrhythmias |
|
|
ECG in Inferior MI Block vessel? |
ST elevations in II, II, and AVF RCA or LCX |
|
|
ECG of anterior MI
Blocked vessel? |
ST elevation in VI-6
LAD |
|
|
RCA supplies what? And what consequences? |
1. Right Ventricle - RV dysfunction causes hypotension 2. AV node - dysfunction causes AV block 3. Hypotension & AV block causes bradycardia |
|
|
Cocaine Toxicity 1. Symptoms 2. Treatment |
1. Psychomoter agitation, dilated pupils, hypertension, acute MI, atrophic nasal mucosa 2. Benzodiazapine D/N give B-Blocker! |
|
|
Eccentric hypertrophy Example |
From chronic volume overload aortic regurg |
|
|
Dyspnea w/Increase pro-BNP Another sign? |
Congestive Heart Failure S3 heard sound |
|
|
Mechanical complications of MI Timeline? |
Free wall rupture of L. ventricle Mitral regurge 2/2 papillary muscle rupture Left Intraventricular septum rupture 3-7 days after MI when the infarcted myocardium is softest |
|
|
Ventricular remodeling post MI can be lessened by what? |
ACE inhibitor B-Blocker |
|
|
Lidocaine increases risk of what in MI? |
Asystole |
|
|
Pulseless electrical activity after MI Suspect what? |
Free wall rupture |
|
|
Strongest influence on long-term prognosis in STEMI |
Time that passes before restoration of coronary blood flow |
|
|
What lab value parallels the severity of heart failure? 1. Why? 2. Treatment |
Hyponatremia Decreased perfusion at baroreceptors and renal arterioles --> Increased ADH, increased renin and increased norepinephrine --> Decreased Na+ Fluid restriction, ACE Inhibitor, loop diuretics |
|
|
Persistent ST-elevation post MI w/deep Q waves in same leads 1. Timeline 2. Dx how? |
Ventricular aneurysm Late --> months Dx: Echo |
|
|
Right ventricular MI 1. Tx w/what 2. Avoid what |
IV fluids to increase Preload Avoid nitrates and diuretics which decreases Preload |
|
|
What drugs to hold 48 hrs before stress testing? |
B-Blockers, Ca2+ Channel blockers, Nitrates |
|
|
Common cause of non-cardiac chest pain (besides musculoskeletal) |
Esophageal disorder (GERD) |
|
|
Chest pain that is reproducible w/palpatation |
musculoskeletal pain (costochondritis) |
|
|
What drug to prevent cardiovascular disease in a diabetic patient? Start when? |
Statin >= 40 yrs old |
|
|
Statins
1. Inhibits what
2. Side effects |
Intracellular HMG-COA Reductase Inhibitor
Hepatic dysfunction
Muscle weakness/tenderness (Rhabdo which can cause renal failure) |
|
|
Stop what drug in pt w/increased creatine phosphokinase? |
Statins Rhabdo --> renal failure |
|
|
What drug to give after unstable angina, NSTEMI, and PCI w/stent? |
Clopidogrel (anti-ADP platelet inhibitor) P2Y12 inhibitor |
|
|
Nitroglycerin pain relief mechanism |
Dilation of capacitance vessels (veins) dilation of veins --> decreased ventricular preload --> decreases O2 req nitroglycerin also decreases afterload by dilating arteries but this is less significant in pain relief |
|
|
Substernal discomfort, left-sided neck pain, diaphoresis, and dyspnea 1. Associated physical finding? |
acute coronary syndrome (MI)
1. S4 heart sound 2/2 stiffening of L. ventricle - S4 is normal in healthy older adults |
|
|
Digoxin Use |
Systolic heart failure afib /a flutter |
|
|
Nausea, vomiting, diarrhea, vision changes, and arrhythmia Next step |
Digoxin toxicity Check drug levels |
|
|
What meds d/n improve survival in pts w/CHF? |
Digoxin & loop diuretics (furosemide) |
|
|
MI w/bibasilar crackles halfway up the lung fields Treatment? |
Acute pulmonary edema diuretics (furosemide) |
|
|
Heart failure after traumatic thigh injury Cause and mechanism |
AV fistula Increased preload, decreased SVR --> Increased CO --> heart failure |
|
|
Concentric Hypertrophy Examples? |
From chronic pressure overload aortic stenosis, hypertension |
|
|
Pounding heart sensation and widened pulse pressure, water hammer pulse
1. Common causes (3)
2. Murmur? |
aortic regurg
1. Rheumatic heart disease Aortic root dilation (Marfans/syphilis) Bicuspid aortic valve
2. Diastolic decrecendo |
|
|
Treatment for viral pericarditus |
NSAIDS (aspirin, naproxen, ibuprofen, indomethacin) and/or colchicine |
|
|
Most common cause of mitral regurg |
mitral valve prolapse from myxomatous degeneration |
|
|
Side effect of dihydrophyridine Ca-channel blockers Most common drug in this group? |
peripheral edema Amlodipine |
|
|
Mid-diastolic murmur w/opening snap |
mitral stenosis |
|
|
Indicators for surgery in pt w/aortic stenosis |
SAD: Syncope, angina, dyspnea |
|
|
Marfan syndrome 1. genetics/mutation 2. Heart and lung issues |
1. Autosomal dominant, Fibrillin-1 2. Aortic dissection, aortic root dilation --> aortic regurg, mitral valve prolapse Spontaneous pneumothorax |
|
|
Decrescendo early diastolic murmur Cause in a young pt |
aortic regurg bicuspid aortic valve |
|
|
acute mitral regurg increases what? |
L. atrial and ventricular filling pressure |
|
|
Blowing holosystolic murmur best heard over the apex with radiation to the axilla |
mitral regurg |
|
|
Systolic murmur at lower sternal boarder that increases with inspiration Common in? |
Tricuspid regurg IV drug users |
|
|
What murmurs should always be investigated and how |
Diastolic and continuous murmurs as well as loud systolic murmurs Echo |
|
|
Symmetric duskiness/coolness of all fingertips |
ischemia 2/2 norephinephrine-induced vasospasm |
|
|
Symptoms of infectious endocarditis |
Roth spot Osler node Joneway lesions |
|
|
New conduction abnormalities in pt w/infective endocarditis |
Perivalvular abscess |
|
|
Palpitations, left and right ventricular dilation Treatment? |
Tachycardia-mediated cardiomyopathy Rate or rhythm control |
|
|
Effect of exercise or atropine on second degree heart blocks What does the opposite? |
exercise/atropine improves type I blocks and worsens type II blocks Vagal maneuvers (carotid massage) |
|
|
Peaked T waves |
hyperkalemia |
|
|
Third-degree or complete heart block |
no conduction from atria to ventricle (p-waves are completely unrelated to QRS waves) |
|
|
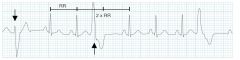
What arrhythmia is specific for digitalis toxicity? |
paroxysmal atrial tachycardia with AV block (2:1) |
|
|
Common causes of exertional syncope |
Ventricular tachycardia L. ventricular outflow obstruction (aortic stenosis) |
|
|
Constrictive pericardities 1. Symptoms 2. Jugular venous pressure tracing shows what 3. What heart sound? 4. Finding on x-ray 5. Causes |
1. Decreased CO leading to dyspnea w/exertion Venous overload (Increased JVP, ascites, edema, etc) 2. Sharp x and y descent 3. Pericardial knock (after S2) 4. Calcification around the heart 5. Virus, surgery/radiation, TB (China, India, Africa) |
|
Treatment if stable or unstable |
Ventricular Tachycardia Unstable --> cardioversion Stable --> antiarrhythmic |
|
|
1. Pulseless electrical activity next step 2. V-fib or pulseless VT next step |
1. CPR & vasopressor (epinephrine) 2. Defibrillation |
|
|
Fixed splitting of S2 |
ASD |
|
|
Aortic coarctation pressure is greater in which arm? |
R > L |
|
|
Megacolon/megaesphophagus & heart disease in a pt from Latin America |
Chagas - trypanosoma Cruzi (protazoan) |
|
|
Cause of outflow obstruction in hypertrophic cardiomyopathy Murmur? Valsalva affects the murmur how? |
1. Septal hypertrophy and abnormal mitral leaflet motion 2. Harsh crescendo-decrescendo murmur after SI 3. Increase |
|
|
Mobitz type II
1. Define
2. Cause
3. Tx |
Second degree heart block: 1. Unpredictable QRS drops without P-R prolongation
2. Block in His-Purkinje system
3. Pacemaker b/c can progress to third degree block |
|
|
Patient from Cambodia w/dyspnea, cough, hemoptysis, palpitations, + irregular heart beats - Cause of palpitations? |
mitral stenosis 2/2 Rheumatic Fever mitral stenosis --> atrial dilation --> a-fib |
|
|
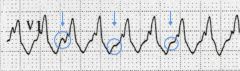
Low-voltage QRS complexes Electrical alternans (beat-to-beat variation in QRS) |
Pericardial effusion / Cardiac Tamponade |
|
|
Risk factors for premature atrial complexes? Treatment |
Tobacco Alcohol Caffeine Stress Decrease risks, Beta-blocker if symptomatic |
|
Treatment |
Premature Ventricular complexes (wide QRS > 120ms) Observation |
|
|
Cause of long-term mortality in patients w/A-fib? Treatment? |
Thromboembolism Warfarin if CHADS-VASc score is > 2 |
|
|
Anatomical cause of: 1. A-fib 2. A-flutter |
1. Pulmonary veins 2. Tricuspid annulus |
|

Paroxysmal supraventricular tachycardia (PSVT) 1. alleviating maneuvers 2. Drug that provides relief |
Abrubt increase in HR usually from AV-node reentry 1. Vagal maneuvers (Valsalva, carotid sinus massage, and immersion in cold water). This decreases conduction through the AV node 2. Adenosine |
|
|
New onset a-fib Check for what disease? If positive, what drug tx? |
Hyperthyroidism B-blocker |
|

Treatment? |
Torsades de pointes Unstable --> defibrillation Stable --> IV magnesium |
|

Next step? |
Ventricular Fibrillation Defibrillation |
|
|
Most important factors for survival in sudden cardiac arrest |
Bystander CPR Rhythm analysis D-fib |
|
|
First degree heart block 1. Define 2. Normal QRS - next step 3. Prolonged QRS - next step |
1. Delayed transmission from atrium to ventricle (increased PR duration) 2. Delay in AV node --> observation 3. Delay below the AV node --> electrophysiology testing |
|
|
Mobitz Type I 1. Alternative Name 2. Define 3. Treatment |
Wenckebach Second degree AV block: progressive prolongation of PR interval leading to QRS drops No treatment necessary |
|
|
Use dependance
1. Definition
2. What classes/drugs? |
1. Increased pharmacologic effects w/increased HR
2. Class 1C - Na+ channel blockers - flecainide & propafenone
3. Class IV - Ca2+ channel blockers - Verapimil, diltiazem |
|
|
Hepatojugular reflex Sign of what |
Push on stomach and see if JVP decreases Sign of constrictive pericarditis, restrictive cardiomyopathy or R. ventricular MI if doesn't decrease |
|
|
Non-cardiac causes of pulses of paradoxus |
Asthma & COPD |
|
|
Heart defects in Hemachromatosis |
Dilated or restrictive cardiomyopathy Conduction abnormalities |
|
|
Uremic pericarditus - serum BUN?
Treatment? |
Serum BUN > 60 mg/dL
Dialysis |
|
|
Hypotension, distended neck veins, pulses paradoxus Treatment? |
Cardiac Tamponade Pericardiocentesis |
|
|
Beck's Triad |
Hypotension Distended neck veins Muffled heart sound (-BP, + JVP) Sign of cardiac tamponade (decreased SV, CO, Preload) |
|
|
Mechanism for pulses paradoxus |
Inspiration --> intrathoracic pressure --> Increased venous return to R. ventricle --> intraventricular septum shifts towards L. ventricle --> decreased L. ventricular filling --> decreased systolic BP |
|
|
Common kind of heart failure in constrictive pericarditus Left or right? |
R heart failure |
|
|
Kussmaul's sign-define associated w/what disease? |
Lack of decrease or an increase in JVP on inspiration Constrictive Pericarditus |
|
|
Name 3 antiarrhythmic drugs |
amiodarone lidocaine procainamide |
|
|
Restrictive Cardiomyopathy 1. Signs on echo 2. Disease causes (4) 3. Which is reversible? 4. Which if proteinuria & easy bruising? |
Diastolic dysfunction, normal or thickened ventricles with normal ventricular volume 2. Amloidosis (4) Sarcoidosis Hemachromatosis (3) Reversible w/phlebotomy Scleroderma |
|
|
Bilateral basal crackles, increased JVP & pitting edema 2 wks after a cold 1. What kind of cardiomyopathy? 2. Organisms 3. Diagnose with? 4. Imaging shows what |
Acute viral myocarditus 1. Dilated cardiomyopathy 2. Coxsakievirus B, parvo B19, HHV6, adenovirus, enterovirus 3. Echo 4. Dilated ventricles + diffuse hypokinesia |
|
|
White granular patch over the buccal mucosa that can not be scraped off in an alcoholic/smoker |
Leukoplakia reactive pre-cancerous lesion from hyperplasia of the squamous epithelium |
|
|
Bone conduction that is greater than air conduction on Rinne test 1. Common cause in adults |
Conductive Hearing Loss 1. Otosclreosis |
|
|
Pt w/hypertension Get what labs? (4) |
1. Urinalysis 2. Chemistry Panel 3. Lipid Profile 4. Baseline ECG |
|
|
Complication of cardiac cath and other vascular procedures What skin finding? |
Arterioembolism (cholesterol embolism) --> causes tissue/organ ischemia Suspect in pt post vascular procedure w/renal failure, purple/painless mottling of skin (livedo reticularis), & GI symptoms |
|
|
Med of choice for acute aortic dissection |
Beta blocker |
|
|
Peripheral artery disease/claudication increases the risk for what? |
MI |
|
|
Define malignant hypertension |
Sever hypertension w/retinal hemorrhages, exudates & papilledema |
|
|
When to perform carotid endarterectomy |
> 70% stenosis |
|
|
Systolic - diastolic abdominal/periumbilical bruit |
Renal artery stenosis --> causes second degree hypertension |
|
|
Alternative to IV penicillin |
IV ceftrioxone |
|
|
Sildenafil
1. For?
2. Contraindicated with?
3. Do what in hypertensive pt? |
1. phosphodiesterase inhibitor for erectile dysfunction
2. Nitrates
3. When combined w/alpha-blocker (doxazosin, give drugs 4 hr apart to prevent hypotension |
|
|
Niacin 1. Use 2. Side-effect 3. Mechanism of 4. Treatment |
1. Treating lipid abnormalities 2. Cutaneous flushing & pruritis 3. Prostaglandin - induced vasodilation 4. Aspirin |
|
|
Target cells seen in? (2) |
Hemoglobinopathies Chronic liver disease |
|
|
Bilateral nasal discharge/obstruction and food tasting bland |
Nasal Polyp |
|
|
Ear pain in a nocturnal teeth grinder |
Temporomandibular Joint Dysfunction |
|
|
Muffled voice + uvula deviation Treatment? |
Peritonsillar abscess
Peritonsillar aspiration + IV antibiotics |
|
|
Early onset hypertension & bilateral abdominal masses 1. Diagnose how 2. Treatment |
Poly cystic Kidney Disease 1. Ultrasound 2. ACE Inhibitor |
|
|
Side effect of loop diuretics |
Ototoxicity |
|
|
Decreased/normal pulmonary capillary wedge pressure Decreased systemic vascular resistance Increased CO, increased mixed venous O2 saturation |
Septic/distributive shock |
|
|
Hypovolemic shock R. Atril Pressure Pulmonary capillary wedge pressure Cardiac output SVR Mixed venous O2 sat |
Everything is decreased except SVR increase |
|
|
What lab is a sensitive indicator of dehydration/hypovolemia |
Increased BUN/creatinine |
|
|
Dizziness, nausea, pallor, diaphoresis, abdominal pain, and general sense of warmth b4 syncope 1. Triggers 2. Diagnostic test |
Neurocardiogenic (vasovagal) Syncope 1. Emotional distress, pain, prolonged standing 2. Tilt table but most are diagnosed clinically |
|
|
Pt w/syncope and suspected structural heart disease Next step? |
Echo |
|
|
Screening for abdominal aortic aneurysm |
Smokers 65-75 y.o w/one-time abdominal ultrasound |
|
|
Hypertensive Emergency 1. Define 2. Treatment? 3. Side effect? 4. Signs/symptoms of side effect |
1. End organ failure (heart/kydney) from hypertension 2. Nitroprusside 3. Cyanide poisoning 4. AMS, seizure, coma, lactic acidosis |
|
|
Hypertension definition 1. Primary intervention 2. Secondary intervention |
> 140 mmHg systolic and/or > 90 mmHg diastolic 1. lifestyle modification - weight reduction 2. DASH diet - increased fruits/veggies, decrease low saturated/total fat |
|
|
Likely DVT Next step? |
Ultrasonography Start heperin if suspect PE but not for suspected DVT |
|
|
Abdominal Aortic Aneurysms 1. Risk factors for rupture? 2. When to operate? |
1. Size, rapid expansion/growth and smoking 2. resect if > 5.5cm, growing > 1cm/yr or causing symptoms |
|
|
Hypertension causes what kind of heart failure? |
Diastolic Stiff ventricle --> filling (diastolic) defect --> L. atrial dilation --> a. fib |
|
|
Define 1. Hypertensive urgency 2. Hypertensive emergency |
1. Severe hypertension (>180/120) w/no symptoms of end - organ failure 2. Sever hypertension w/organ failure |
|
|
Man who loses consciousness immediately after urination or a coughing fit |
Situational syncope |
|
|
Exertional Heat Stroke 1. Define 2. Complications 3. Treatment |
1. Temp > 40 C (104 F) w/encephalopathy 2. Multi-organ dysfunction 3. Rapid cooling (ice-water) |
|
|
Orthostatic Hypotension 1. Definition 2. Causes of aging |
1. 20mmHG decrease systolically or 10mmHg decrease diastolically on standing 2. Decreased baroreceptor sensitivity |
|
|
Muscle weakness, recurrent nephrolithiasis, neuropsychiatric symptoms, and hypercalcemia Most common cause? |
stones, groans, moans & psychiatric overtones = Primary Hyperparathyroidism - Usually 2/2 parathyroid adenoma |
|
|
Howell-jolly bodies seen in? |
Pts w/out a spleen |
|
|
Post MI: leg is cold/mottled Next step? |
Acute limb ischemia Echo to look for L. ventricular thrombus |
|
|
Bilateral pitting edema, varicose veins and venous ulcer Treatment? |
Venous Insufficiency Leg elevation, compression stockings and exercise |
|
|
Imaging choice for aortic dissection |
CT but transesophageal echo if abnormal creatinine (kidney disease) |
|
|
Management of ST-segment elevation myocardial infarction (STEMI) 1. When to cath? 2. What to do if can not cath? 3. Drugs? |
1. Perform percutaneous coronary intervention (PCI) w/in 12 hrs of symptom onset or 90 min of medical contact 2. Fibrinolytics if w/in 12 hrs of symptom onset 3. oxygen, aspirin, plt P2Y12 receptor blocker (clopidogrel, ticagrelor), nitroglycerin, beta blocker, and anti-coagulant (heparin) |
|
|
Amiodarone For? Side effects? |
Anti-arrhythmic --> for ventricular arrhythmias, rhythm control and ventricular systolic dysfunction hypo/hyperthyroidism hepatotoxicity Bradycardia/heart block lung/neuro/eye disturbances (corneal deposits) pulmonary fibrosis blue-gray skin |
|
|
Nocturnal, brief (15-20 min) pain in a young woman 1. Associated w/what other 2. Greatest risk factor? 3. Treatment? |
Angina (prinzmental/varient) 1. Raynauds + migraine headaches 2. smoking 3. Ca2+ channel blockers, nitrates |
|
|
Normal JVP |
< 3cm above sternal angle |
|
|
Dressler's syndrome Treatment? |
Post-mycardial pericarditus 1-6 wks after MI NSAIDS (aspirin) |
|
|
Side effects of hydrochlorothiazide 1. Metabolic side effects 2. Electrolyte abnormalities 3. Activates what disease? |
Hyperglycemia, increased LDL, increased triglycerides 2. Hypercalcemia, hyponatremia and hypokalemia 3. Gout |
|
|
5 P's after an MI 1. Define 2. Next step 3. Definitive treatment |
Limb ischemia (artery occlusion) Pain, pallor, pulselessness, parethesia, poilcilothermea Heparin Embolectomy (surgery) |
|

Irregularly irregular ECG, absent p-wave Treatment? |
A-fib If stable --> B-blocker or Ca2+ channel inhibitor If unstable --> cardioversion --> AMS, hypotension, etc |
|
|
ECG findings for preicarditus Specific ECG finding? |
Diffuse ST elevations PR depression |
|
|
Headache, increased BP, renal bruit 1. Cause in young vs old pt 2. Treatment |
Renal artery stenosis 1. young = fibromuscular dysplasia old = atherosclerosis 2. Angioplasty w/stent placement |
|
|
Scleroderma Renal Crisis What blood cells? |
Acute Renal Failure + Hypertension Schistocytes |
|
|
Imaging of choice for diagnosis and follow-up of an abdominal aneurysm |
Ultrasound |
|
|
Hypertrophic Cardiomyopathy 1. Symptoms 2. Inheritance 3. Mechanism 4. Treatment |
1. Episodes of syncope, systolic (harsh crescendo decrescendo) murmur along left sternal boarder, sudden death. 2. Autosomal dominant 3. Myocardial hypertrophy causes diastolic heart failure asymmetrical septal hypertrophy 4. B-blockers (prolongs diastole) Cardiac acting Ca2+ channel blocker (diltiazem) |
|
|
Cause of: 1. Ascending aortic aneurysms 2. Descending aortic aneurysms |
1. Cystic medial necrosis (aging) Connective tissue diseases (Marfans, Ehlers-Danlos) 2. Atherosclerosis |
|
|
Heparin-induced thrombocytopenia 1. What drug? 2. Signs/symptoms? 3. Type I vs Type II |
1. Unfractionated heparin 2. Decreased plt more than 50%, thrombosis, thrombocytopenia 3. Type I - non-immune direct effect of heparin on plts usually on day 2. No need to stop Type II - antibodies against PF4, on days 5-10, Stop med |
|
|
Suspect Hypertension second degree to kidney disease when? (4) |
1. Diffuse atherosclerosis 2. Asymmetrical kidney size 3. Recurrent flash pulmonary edema 4. Increase serum creatinine > 30% after starting ACE inhibitor |
|
|
Single photon emission CT scan 1. Used for? 2. Treatment? |
1. Evaluating CAD. Decreased perfusion = CAD, if inducible, then ischemic coronary artery disease 2. Anti-platelet (aspirin), B-blockers and lifestyle modifications to prevent MI Ca2+ channel blockers and nitrates are used if pt has hypotension or bradycardia |
|
|
Treatment for acute decompensated heart failure (3) |
oxygent, diuretics, nitrates |
|
|
Treatment for A-fib in Wolff-Parkinson-White |
Unstable --> cardioversion Stable --> rhythm control: procainamide |
|
|
Bradycardia, hypotension, wheezing, hypoglycemia, delirium, seizures and cardiogenic shock 1. Treatment - 1st & 2nd step |
B-blocker overdose Atropine + IV fluids IV glucagon |
|
|
Malignant otitis externa in old diabetic patient 1. Signs/sumptoms 2. Organism 3. Complications 4. Treatment |
1. Ear discharge granulations 2. Pseudomonas 3. Osteomyelitis of skull or nerve damage 4. Systemic antibiotics (ciprofloxacin) |
|
|
Most common benign primary cardiac tumor 1. Location 2. Symptoms 3. Complications |
Myxoma 1. Usually L. atrium 2. constitutional symptoms (fever, wt loss, etc) 3. Systemic embolization |
|
|
Peripheral artery disease (claudication)
1. Treatments |
Aspirin + statin Graded Exercise |
|
|
Treatment for pulmonary hypertension 2/2 left heart disease |
Diuretics and ACE inhibitor |
|
|
Systolic hypertension w/left ventricular hypertrophy in elderly 1. Cause 2. Treatment |
Isolated systolic hypertension (ISH) 1. Decreased elasticity aterial wall (arteries become rigit) as pt ages causing widened pulse pressure (increased systolic w/normal diastolic) 2. Thiazide, ACE inhibitor, or Ca2+ channel blocker |
|
|
3 uses for N-acetyl cysteine |
1. Dissolution of mucus 2. protection from contrast-induced renal failure 3. Acetaminophen overdose |
|
|
Vertigo, earfullness, tinnitus, hearing loss Treatment? |
Meniere's disease (inner ear) Diet modifications: no drugs/alcohol and sodium restriction |