Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
41 Cards in this Set
- Front
- Back
|
Right side valve (between atria and ventricle)
Left side valve (between atria and ventricle) What valves exit from ventricles? |
Tricuspid
Mitral (bicuspid) Pulmonary = right side (semilunar) Aortic = left side (semilunar) |
|
|
What principle do the A-V valves operate under?
If pressure is greater in ventricle than atrium, is the valve open? Does the same principle hold for the pulmonary and aortic valves? |
Pressure differences
No - close Yes |
|
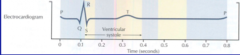
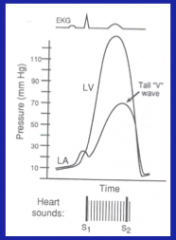
What does each letter represent?
|
P = atrial depolarization (much smaller mass than ventricle)
QRS = ventricular depolarization T = ventricular repolarization (occurs more slowly because K channels operate more slowly than the fast sodium channel) |
|
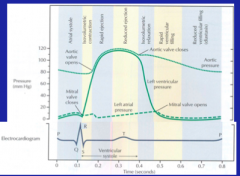
Explain the cycle.
|
1. Atrial contracts after the P wave which increases atrial pressure
2. Ventricular pressure increased do to increased ventricular volume 3. Activation of QRS leads to isovolumetric contraction --> ventricular pressure increases because both aortic and mitral valves are closed. 4. After aortic valve opens, ventricular and aortic pressures continue to increase during rapid ejection period (40% of ventricular systole) 5. Peak pressure starts declining during REDUCED rejection period 6. In ventricular systole, atria are ia diastole and are getting filled up with venous return. 7. Ventricular systole ends, aortic pressure exceeds ventricular pressure --> aortic valve closes (ISOVOLUMETRIC RELAXATION) 8. Mitral valve open again when atrial pressure exceeds ventricular pressure. |
|
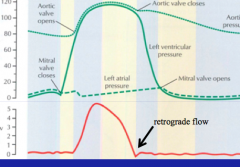
When does ascending aortic blood flow peak?
Is there any retrograde flow? Why? |
At the end of rapid ejection
For a fraction of a second due to aortic valve closure. |
|
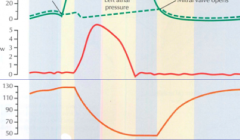
When does ventricular volume decline rapidly? When does it increase rapidly?
When does slower filling occur? |
Rapid ejection phase
Rapid ventricular filling phase Reduced ejection and filling period (diastasis) |
|
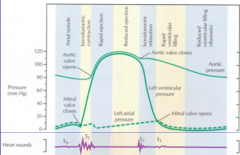
What are the first hear sounds heard?
Are they split? |
Closure of mitral and tricuspid valves
No = occur close together and heard in vibrations set in motion. |
|
|
What are the second heart sounds heard?
What is the difference between this and the first sounds? Can it be split under physiological conditions? |
Closure of the aortic and pulmonary valves
Shorter and higher in frequency Yes = deep breathing S3 vibrations from filling of ventricles in diastole (not usually heard) |
|
|
What is associated with hearing an S3?
S4? |
S3 = ventricles fill early in dilation = cardiac disease associated with ventricular overload due to heart failure or valve problems
S4 = atrial contraction association, stiffened ventricle causes vibrations (ATRIAL GALLOP). |
|
|
Describe the first heart sound.
|
FIRST HEART SOUND IS GENERATED BY OSCILLATION OF BLOOD AND VIBRATION IN VENTRICLES, FOLLOWING CLOSURE OF A-V VALVES. IT IS LOWER PITCHED, MORE INTENSE AND LONGER THAN THE SECOND SOUND
� |
|
|
Describe the second heart soung?
|
SECOND HEART SOUND IS GENERATED BY OSCILLATION OF BLOOD IN AORTA AND PULMONARY ARTERY, FOLLOWING CLOSURE OF AORTIC AND PULMONIC VALVES
� |
|
|
Describe the third heart sound.
|
THIRD HEART SOUND OCCURS DURING EARLY DIASTOLE, IT IS LOW IN PITCH AND INTENSITY IN THE NORMAL HEART. HOWEVER, DURING HEART FAILURE IT HAS INCREASED INTENSITY. IT IS GENERATED BY VIBRATION OF BLOOD DURING VENTRICULAR FILLING
� |
|
|
Describe the fourth heart sound.
|
FOURTH HEART SOUND OCCURS DURING ATRIAL CONTRACTION AND IS LOW IN INTENSITY AND PITCH
� |
|
|
What is the equation of the work of the heart?
|
Pressure times volume
|
|
|
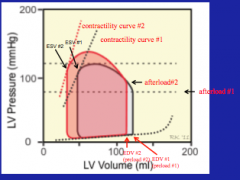
What is the Frank-Starling relationship again?
|
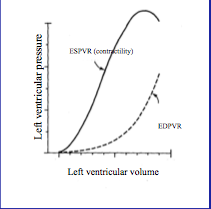
Ventricular contractability is regulated by left ventricular volume (end systolic pressure volume relationship = ESPVR) at the end of diastole
EDPVR (end diastolic pressure volume relationship) also shown. |
|
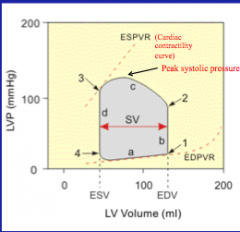
Label the parts of the graph.
|
a = ventricular filling
1 = mitral valve closes b = isovolumetric contraction 2 = afterload; aortic valve opens c = ventricular ejection 3 = aortic valve closes d = isovolumetric relaxation 4 = mitral valve opens |
|
|
What is systolic pressure?
|
Peak pressure in the AORTA, not the ventricle.
|
|
|
Peak ventricular systolic pressure
|
Systolic pressure in the ventricle
|
|
|
Diastolic pressure
|
Minimum pressure in the AORTA, not ventricle
|
|
|
End diastolic pressure
|
Pressure in ventricle just before mitral valve closes
|
|
|
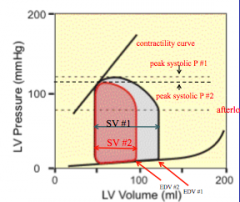
What is the effect of an increase in preload volume?
|
Increase in preload volume = similar increase in stroke volume
|
|
|
Define preload
|
Ventricular pressure at the end of diastole = determined by ventricular and diastolic volume
|
|
|
Afterload
|
Ventricular pressure during contraction. Equivalent to diastolic aortic pressure
|
|
|
Contractility
|
Strength of ventricular contraction independent or preload or after load = also known as INOTROPY
|
|
|
Stroke volume
|
Volume of blood ejected by ventricle during systole. Can be calculated as end diastolic volume minus end systolic volume.
|
|
|
Ejection fraction
|
Fraction of end diastolic volume ejected by ventricle during systole
Calculated as stroke volume divided by end diastolic volume Normal values 55%-75% |
|
|
Cardiac output
|
Volume of blood ejected by ventricle in one minute
Stroke volume * heart rate |
|
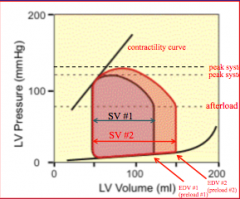
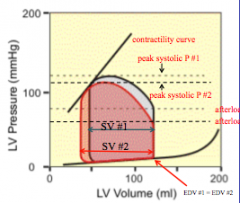
What is the effect of increasing preload?
|
Stroke volume is increased
Peak systolic pressure increased End systolic volume remains the same Arterial pressure = stroke volume*total peripheral resistance, thus there will be an increase in arterial pressure if the heart rate is held constant. |
|
What is the effect of decreasing preload?
|
Decreased stroke volume (deacrease pressure) and decreased systolic pressure.
END SYSTOLIC VOLUME IS THE SAME! |
|
|
What is the relationship between afterload and the shortening velocity?
|
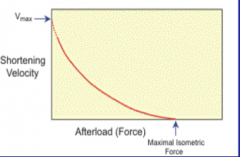
Reciprocal relationship
Increase afterload force --> decrease shortening velocity up to the maximal isometric force |
|
|
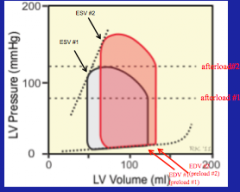
What is the effect of increasing afterload without changing preload or contractibility (inotropy).
|
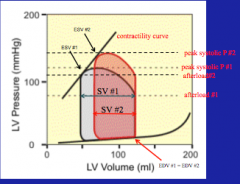
Decreased shortening velocity --> increased end systolic volume and thus decreased stroke volume
Can occur if increased aortic pressure is increased by increasing TPR Aortic pressure = TPR x Cardiac output |
|
|
What is the effect of decreasing afterload?
|
Increased stroke volume
|
|
|
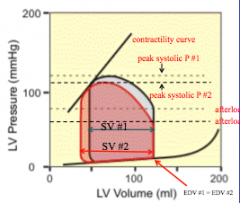
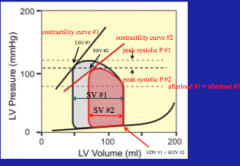
What is the effect of increasing contractility (inotropy) while keeping preload and afterload constant?
|
Increased stroke volume and increased systolic pressure (decreases end systolic volume)
Intrinsic activation of the heart = under influence of increased sympathetic activity |
|
|
What is the effect of decreasing contractility (inotropy)?
|
Decreased stroke volume and decreased systolic pressure
Influence of DECREASED sympathetic activity |
|
|
What are the compensatory changes after increasing preload at constant contractility?
|
Increase in stroke volume --> increase in afterload --> ESV
Cardiac output = stoke volume x heat rate Arterial pressure = cardiac output x TPR |
|
|
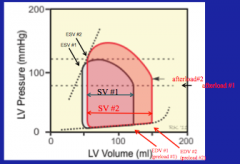
What does increasing afterload cause at constant contractility?
|
Reduction in stroke volume and increase in end systolic volume --> end diastolic volume increase because increase in systolic volume gets added to the incoming venous return.
Increase in afterload could be from an increase in TPR |
|
|
What the compensatory changes after increasing contractility (inotropy)?
|
Can be caused by an increase in sympathetic activity
Decrease in end systolic volume --> increase stroke volume --> secondary increase in afterload Secondarily decreased end diastolic volume due to decreased end systolic volume Afterload will increase due to increased stroke volume |
|
|
What is the effect of aortic stenosis on cardiac events?
|
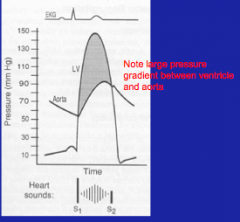
Systolic murmur due to turbulent flow into aorta
Heard in crescendo decrescendo manner Associated with high end diastolic volume and low stroke volume/ejection fraction. |
|
|
What is aortic regurgitation associated with?
|
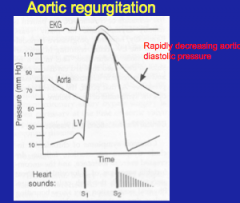
Diastolic murmur due to turbulent retrograde flow aorta into ventricle, high ventricular end diastolic volume, low effective stoke volume, and high pulse pressure, due to lowered diastolic pressure.
|
|
|
What does mitral stenosis cause?
|
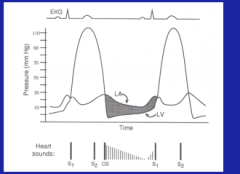
Increased left artrial pressure
Diastolic murmur due to high velocity of blood flow --> turbulence and murmur |
|
|
What does mitral regurgitation cause?
|
Atrial pressure rises during systole, due to backflow into atria --> systolic murmur due to turbulent back flow.
|