Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
74 Cards in this Set
- Front
- Back
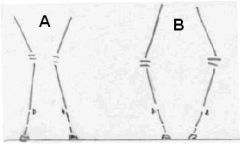
Which shows varus and which is valgus?
|
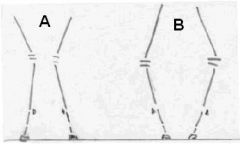
A = valgus
B = varus |
|
|
What is the common signalment for hypertrophic osteodystrophy? What is the textbook radiographic lesion?
|
3-5 mo mid to giant breed dog
Double physis |
|
|
Which of the following are acceptable hypertrophic osteodystrophy treatments?
a) NSAIDs b) Vitamin D supplementation c) Vitamin C supplementation d) Short course steroids |
a) NSAIDs
d) Short course steroids |
|
|
Subperiostal hemorrhage with ossification at the metaphyses is indicative of...
|
...hypertrophic osteodystrophy
|
|
|
What is the common signalment for panosteitis? What is the textbook radiographic lesion?
|
5-18 mo mid to giant breed dogs.
"fluffy" diaphysis around the nutrient foramen |
|
|
A 6mo Great Dane was lame on the left rear limb last week and is now lame on the right rear limb. What gives?
|
Panosteitis, my friend!
|
|
|
Necrosis of bone marrow fat around the nutrient foramen is indicative of...
|
...panosteitis
|
|
|
T or F:
With panosteitis, you should always radiograph the contracranial or contracaudal limb. |
False!
Radiograph the CONTRALATERAL limb. |
|
|
What three procedures are done when retained cartilagenous core causes angular limb deformities?
|
Ulnar ostectomy
Radial osteotomy Radial distraction osteogenesis |
|
|
Which of the following is NOT true regarding retained cartilagenous core?
a) it is a version of OCD b) occurs most often in giant breed dogs c) middle sized breeds often show no signs d) lack of oxygen causes retention of the membranous ossification site in the distal ulna |
d) lack of oxygen causes retention of the membranous ossification site in the distal ulna (should be ENDOCHONDRAL ossification)
|
|
|
What are appropriate treatments for retained cartilagenous core with no angular deformity?
|
Decrease caloric intake
Limit Ca:P ratio |
|
|
The congenital absence of digits is...
|
...ectrodactyly
|
|
|
The congenital absence of one of a pair of bones is...
|
...ectromelia
|
|
|
T or F:
Craniomandibular osteopathy is self limiting. |
True! Regresses after growth plate closure
|
|
|
"Mushrooming" at bone ends due to extra growth plates is indicative of which condition? How is this treated?
|
Multiple Cartilagenous Exostoses;
(tx: surgery to cut out the extra growth plates) |
|
|
T or F:
Idiopathic calvarial hyperostosis occurs only in bull mastiffs. |
True!
|
|
|
What is the appropriate treatment for idiopathic calvarial hyperostosis?
|
Benign neglect unless brain/eye involvement (then surgery).
|
|
|
What are the 2 kinds of dwarfism?
|
Pituitary dwarfism
Osteochondrodysplasia |
|
|
Which of the following are not associated with osteochondrodysplasia?
a) retention of puppy coat b) angular limb deformities and hemolytic anemias c) cataracts & retinal detach d) diabetes insipidus and elbow subluxation |
a) retention of puppy coat (NOPE, this is PITUITARY)
d) diabetes insipidus and elbow subluxation (DI is PITUITARY but elbow sublux is osteochondro) |
|
|
Which dogs get congenital elbow luxation?
|
Little white fluffy dogs (Maltese)
|
|
|
Which of the following are associated with congenital elbow luxation?
a) hemimelia/ectromelia b) ectrodactyly c) cataracts and retinal detachment d) Legg-Calves-Perthes Disease |
a) hemimelia/ectromelia
b) ectrodactyly |
|
|
How is congenital elbow subluxation repaired?
|
<4 mos - pins and closed reduction
>4 mos - open reduction |
|
|
Legg-Calves-Perthes Disease =
|
Necrosis of the femoral head
|
|
|
What is the signalment for Legg-Calves-Perthes Disease?
|
4-11 mo little dogs (terriers, mini poodles)
|
|
|
T or F:
Legg-Calves-Perthes Disease always carries a poor prognosis. |
False!
If there is no articular cartilage damage and the disease is realized early and sling immobilized, GOOD PROGNOSIS |
|
|
Early closure of the tibial tuberosity growth plate leads to:
a) patella baja b) patella arriba c) patella alta d) epiphysitis of the tibial tuberosity |
a) patella baja
or c) patella alta (if the tuberosity gets avulsed) |
|
|
What is weird about the distal ulnar growth plate?
|
cone shaped
|
|
|
What are causes of early physeal closure?
|
Trauma
Overnutrition |
|
|
What is the most common location for early physeal closure in the dog?
|
Distal ulna/radius
|
|
|
Which of the following would you NOT do when preventing angular limb deformities in a large breed dog?
a) Ensure the Ca:P ratio is 1.2:1 b) Switch to adult food @ 1 yr c) Delay spaying/neutering d) Prevent stressful activity until 1 yr e) Limit total caloric intake |
b) Switch to adult food @ 1 yr (should be 4 mos)
|
|
|
Which of the following are true?
a) 15% of ulnar growth is proximal and the rest is distal b) the radius can normally be longer than the ulna during growth spurts c) 60% of radial growth is proximal and the remainder is distal d) due to the conical shape of the distal ulnar physis, varus is the most common form of forelimb angular deformity |
a) 15% of ulnar growth is proximal and the rest is distal
b) the radius can normally be longer than the ulna during growth spurts Note: 60% of radius growth is DISTAL and VALGUS is the most common angular deformity |
|
|
Discrepancy of > ________ mm on an elbow radiograph = incongruity. At what age is this measured?
|
>2mm @ 8-10mos
|
|
|
What are the radiographic signs of radius/ulnar angular deformity seen in the elbow?
|
Remodeling of anconeal process
Shallow trochlear notch Dorsal displacement of coronoid procss |
|
|
What are the common radiographic signs of radius/ulnar angular deformity seen in the carpus?
|
Closed distal ulnar physis
Open distal radial growth plate Proximal location of ulnar styloid Increased angulation |
|
|
When do the radial and ulnar physes close?
|
220-250d
|
|
|
When are small breeds skeletally mature? Large breeds? Giant?
|
Small (4mos)
Large (7mos) Giant (8mos) |
|
|
Which of the following are true:
a) premature radial physeal closure results in valgus at the carpus b) inward rotation of the paw can be due to premature radial physeal closure c) cranial bowing of the radius is caused by premature distal ulnar physis closure d) asymmetrical radial physeal closure usually occurs on the medial aspect |
b) inward rotation of the paw can be due to premature radial physeal closure
c) cranial bowing of the radius is caused by premature distal ulnar physis closure Note - radial physeal closure = VARUS; asymmetrical closure is LATERAL |
|
|
Which of the following are NOT options for treating angular limb deformities before skeletal maturity?
a) calorie restriction b) diaphyseal osteotomy c) Ca:P altreation d) Ulnar physeal osteotomy |
a) calorie restriction
c) Ca:P altreation (diet won't work once the bones are crooked) |
|
|
What is the major limiting factor for distraction when doing a corrective osteotomy to correct angular limb deformity?
|
Soft tissues! (vessels, nerves, etc)
|
|
|
Which of the following are NOT true:
a) Corrective osteotomies may take 1-2 years to heal. b) The goal of corrective osteotomies is retention of pain free function. c) limb lengthening is performed at a rate of 0.5 to 1mm/day d) ex-fix is better than plating with a wedge resection |
d) ex-fix is better than plating with a wedge resection is NOT true! Plating is better (although ex-fix allows for post-op adjustment)
|
|
|
How much limb lengthening can be expected with corrective osteotomy?
|
Up to 2cm
|
|
|
T or F:
Ulnar ostectomy can resolve elbow subluxation provided no DJD has developed |
True!
|
|
|
What are the 3 types of joints and what are examples of each?
|
Synarthroses (fibrous - skull sutures)
Amphiarthroses (cartilaginous - costochondral junction) Diarthroses (synovial - stifle) |
|
|
What are the non-inflammatory categories of joint disease and which is the most common?
|
Trauma
Neoplasia Dejenerative (DJD; most common) |
|
|
T or F:
DJD = OA = rheumatoid arthritis |
False!
DJD does = OA (both are non-inflammatory). However, rheumatoid arthritis is an IMMUNOLOGICAL INFLAMMATORY process |
|
|
Which of the following characterize DJD?
a) joint pain b) osteophytes/enthesiophytes c) inflammatory response d) slow progression |
a) joint pain
b) osteophytes/enthesiophytes d) slow progression |
|
|
Which of the following ARE NOT true:
a) hyaline cartilage = 70% water, 20% collagen, and 10% proteoglycan b) Hyaluronic acid minimizes compressive forces c) Hyaluronic acid minimizes shear forces d) chondrocytes cannot replenish once they die |
a) hyaline cartilage matrix + chondrocytes
MATRIX = 70% water, 20% collagen, and 10% proteoglycan |
|
|
What molecule kills chondrocytes and/or degrades matrix?
|
MMPs (matrix metalloproteinases)
Cytokines also cause loss or cartilage |
|
|
What are the bony changes associated with DJD?
|
Osteophytes
Enthesophytes Subchondral sclerosis Eburnation |
|
|
Describe the following parameters in a normal joint.
a) protein content b) viscosity c) cell count |
a) protein content - <2.5mg/dl
b) viscosity - high c) cell count - <3000/uL (mostly lymphocytes) |
|
|
Describe the following parameters in a joint w/DJD.
a) protein content b) viscosity c) cell count |
a) protein content - <2.5mg/dl
b) viscosity - medium c) cell count - 1000-5000/uL |
|
|
Which of the following are NOT acceptable long term treatments for most types of DJD?
a) NSAIDs b) Steroids c) Weight control & exercise modification d) joint replacement |
b) Steroids - only use ONCE or if you KNOW its immune mediated
|
|
|
A genetic malformation of subchondral bone describes...
|
...osteochondrosis (+/- dissecans)
|
|
|
T or F:
OCD is often bilateral. |
True!
|
|
|
How is osteochondrosis treated?
|
STRICT exercise restriction and wait for ossification. Otherwise, arthrotomy/arthroscopy to remove free fragments.
|
|
|
OCD prognosis is good only in which joint?
|
Shoulder
|
|
|
Which of the following are NOT acceptable pharmaceutical therapies for DJD?
a) Oral NSAIDs b) IM polysulfated GAG c) IA cosequin d) IM hyaluronic acid |
c) IA cosequin (should be ORAL)
d) IM hyaluronic acid (should be IA) |
|
|
What are physical signs that can help to differentiate infectious from non-infectious inflammatory joint disease?
|
NONE! They look the same! (malaise, lameness, maybe fever, swollen joints)
|
|
|
What are causes or ruleouts for non-erosive, noninfectious inflammatory joint disease?
|
Idiopathic
Lupus Inflammation of chronic dz |
|
|
Immune mediated arthropathies are all type ______ immune response.
|
type III
|
|
|
When performing a joint tap, what tubes do you need for collection and for which tests?
|
Purple top (cytology, protein count, cell count)
Red top (culture) |
|
|
How is synovial fluid grossly evaluated?
|
Color, clarity, consistency, quantity, viscosity
|
|
|
What are the 3 major signs of SLE? How can it be diagnosed?
|
Joint dz, thrombocytopenia/leukopenia, glomerulonephritis + PLE
(dx: via ANA or Coomb's test) |
|
|
Which of the following are erosive, inflammatory arthropathies?
a) Septic arthritis b) Shar-pei fever c) SLE d) DJD |
a) Septic arthritis
|
|
|
What is a common signalment for feline progressive polyarthritis?
|
Males w/FeLV and FSV
|
|
|
What will a joint tap look like in an animal with an erosive inflammatory joint disease?
|
Cloudy, yellow-tinged fluid with lots of leukocytes.
|
|
|
T or F:
Any chronic antigenic stimulation can cause an immune mediated polyarthropathy. |
True!
|
|
|
T or F:
A few neutrophils are commonly expected in normal synovial fluid. |
False!
Treat ANY neuts with suspicion!! |
|
|
What is the most common signalment for idiopathic polyarthritis?
|
1-3 yo dog
|
|
|
What are rheumatoid factors? Which disease in dogs do these help to diagnose?
|
IgM and IgG against IgGs; pretty USELESS in dogs
|
|
|
Which of the following test helps to diagnose canine rheumatoid arthritis?
a) ANA b) Coomb's c) Rheumatoid factor |
NONE! Need good physical, joint fluid analysis (with poor mucin clot test), and synovial biopsy
|
|
|
What are appropriate medical treatments for the polyarthritides?
|
Immunosuppress (pred or maybe cyclophosphamide or azathioprine)
|
|
|
Which of the following tests can be used to distinguish infectious from non-infectious arthropathies?
a) history b) signs c) joint tap d) titers |
ALL OF THEM
a) history b) signs c) joint tap d) titers |
|
|
Which of the following tests can be used to distinguish inflammatory from non-inflammatory arthropathies?
a) history b) signs c) joint tap d) titers |
c) joint tap
|