Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
|
Brain stem contains
|
- 10 cranial nerves
- cranial nuclei - medial lemniscus (gracile and cuneate tracts) - spinal lemniscus (spinothalamic tract) - corticospinal tract |
|
|
Midbrain Cranial Nuclei
|
CNIII
|
|
|
Pons Nuclei
|
CN IV, V, VI, VII, VIII
|
|
|
Medulla Nuclei
|
CN, IX, X, XI, XII
|
|
|
Damage to III
|
III – oculomotor: supplies all extrinsic eye muscles: medial, superior, and inferior rectus,
inferior oblique and levator palpebrae muscles. Damage results in diplopia (double vision), ptosis (drooping eyelid), and outward deviation of the eye. |
|
|
Damage to IV
|
IV – trochlear: supplies the superior oblique muscle. Damage results in upward deviation
of the eye and thus diplopia. |
|
|
Damage to V
|
V – trigeminal: supplies general sensory to the face (touch, proprioception, pain, heat),
the muscles of mastication as well as tensor tympani, tensor palati and digastric. Damage results in decreased sensitivity of face (possible numbness), brief attacks of pain, weakness and wasting of jaw muscles and asymmetric chewing. |
|
|
Damage to VI
|
VI – abducens: supplies the lateral rectus muscle. Damage results in inward deviation of the eye and thus diplopia.
|
|
|
Damage to VII
|
facial: supplies the muscle of facial expression, stapedius muscle, taste to the
anterior 2/3rds of the tongue and lacrimal and salivary glands. Damage results in paralysis of the facial expression muscles and loss of taste of ant 2/3rds of tongue |
|
|
Damage to VIII
|
vestibulocochlear: supplies the vestibular apparatus and the cochlear. Damage results in deafness (sometimes tinnitus) and disequilibrium
|
|
|
Damage to IX
|
IX – glossopharyngeal: supplies sensation to the palate and taste to the posterior 1/3rd of the tongue and stylopharyngeal muscle. Damage results in pain spasms in posterior pharynx and loss of taste in posterior 1/3rd of tongue.
|
|
|
Damage to X
|
X – vagus: supplies autonomics and transmits sensory information to/from the viscera and
heart, muscle of pharynx and larynx. It also supplies the muscles of the pharynx and larynx. Therefore damage results in hoarseness, poor swallowing and loss of gag reflex. |
|
|
Damage to XI
|
XI – accessory: supplies trapezius and sternocleidomastoid muscles. Damage results in
wasting in the neck with weak neck rotation - cant shrug. |
|
|
Damage to XII
|
XII – hypoglossal: supplies the intrinsic muscles of the tongue, hyoglossus, styloglossus and genioglossus muscles. Damage results in wasting of tongue and tongue deviation to side of lesion on protrusion.
|
|
|
Neural tube forms _____ vesicles to begin with called ______________. They then form the ____________ secondary.
|
3.
(1). Prosencephalon: telecephalon (cerebral hemispheres) and diencephalon (thalamus/hypothamalus); (2) Mesencephalon - forms the midbrain (3) Rhombencephalon - forms the brainstem -metencephalon (pons and cerebellum) and the myelencephalon (medulla oblongata) |
|
|
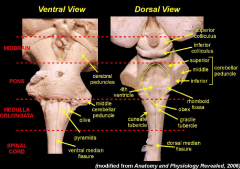
brainstem surface anatomy
|
|
|
|
Pyramids
|
• pyramids (pyr): A pair of columnar elevations on the ventral surface of the medulla, either
side of the midline. They comprise the descending motor fibres (corticospinal tracts). These fibres originate in the cerebral cortices, most of the fibres cross the midline in the lower medulla (pyramidal decussation; Px), to form the lateral corticospinal tract. Above, the pyramids are continuous with cerebral peduncle. |
|
|
Olives
|
• olives: A pair of elevations lateral to pyramids in the upper medulla, formed by the ‘olivary
nuclei’ located just below the surface. The olivary nuclei supply information regarding motor control to the cerebellum – a region concerned with coordination of movement. |
|
|
rhomboid fossa
|
• rhomboid fossa: The quadrilateral shaped floor of the 4th ventricle, on the dorsal surface of
brainstem. Sections of the brainstem which cut through the lower end of the rhomboid fossa are commonly referred to as sections of the 'open medulla'; below the level of rhomboid fossa they are referred to as 'closed medulla'. |
|
|
superior cerebellar peduncle
|
The cerebellum is attached to the brainstem by 3 pairs
of large fibre bundles called cerebellar peduncles. The cut surfaces of these peduncles are visible. The superior cerebellar peduncle mostly comprises fibres that pass from the cerebellum into the midbrain beneath the colliculi and continue to the red nucleus and thalamus. This motor outflow from the cerebellum is concerned with motor coordination |
|
|
gracile (Gr) and cuneate (Cu) tubercles
|
2 pairs of eminences on dorsal surface of
medulla, immediately below the lower margin of the 4th ventricle. The most medial pair is the gracile tubercles; the more lateral pair is the cuneate. Beneath these tubercles lie nuclei of the same name. These nuclei comprise cells which receive synapses from fibres of the dorsal column tract (gracile and cuneate tracts) just before they cross the midline. Axons originate from the gracile and cuneate nuclei cross the midline and ascend to the thalamus as the medial lemniscus. Remember that the cuneate and gracile tracts are carrying sensory information from the spinal cord up to the thalamus and cerebral cortex. What sensory information do they carry and from which side of the body? |
|
|
inferior cerebellar peduncle
|
• inferior cerebellar peduncle (icp): An indistinct bulge on the lateral aspect of the medulla,
comprising fibres which carry information about position and balance to the cerebellum. That is, spinocerebellar fibres and vestibular fibres. |
|
|
pons and middle cerebellar peduncle
|
• pons and middle cerebellar peduncle (mcp): A prominent, horizontally elongated feature
on the ventral surface of the brainstem, comprising nuclei (cells) that receive synapses from descending motor fibres (corticopontine fibres) and give rise to ‘pontocerebellar fibres’ that cross the midline (hence the lack of a midline groove at this level) and enter the cerebellum. This is the major connection between cerebral cortex and cerebellum. |
|
|
inferior colliculi
|
• inferior colliculi (IC): Pair of structures on dorsal brainstem at level of cerebral peduncles,
They are relay nuclei in the hearing pathway. |
|
|
superior colliculus
|
• superior colliculus (SC): Pair of structures on dorsal aspect of brainstem (rostral to former)
What is their role in vision? |
|
|
Location of sensory and motor in brainstem
|
- sensory nuceli; dorsolateral aspect
- motor nuclei; medial aspect - central canal; dorsal and lateral to form the 4th ventricle |
|
|
Migration of alar and basal plates in brainstem
|
- closed medulla; migrate in a relatively simple fashion forming the dorsal and ventral horns respectively
- open medulla and rostral; as above |
|
|
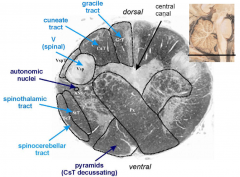
Closed Medulla Crossection; MOTOR DECUSSATION
|
|
|
|
Closed Medulla Crossection: SENSORY DECUSSATION
|
Fibres ascending in the
dorsal columns synapse on cells in nuclei of the corresponding names (CuN and GrN) and, before continuing their progress rostrally, pass ventrally and medially to cross the midline anterior to the central grey. The crossing fibres are referred to as the internal arcuate fibres (IntAr; sensory decussation). Having crossed the midline these fibres assemble together adjacent to the midline and form the medial lemniscus (ML). • The ScT and StT are still lying lateral in this region of the brainstem, although the ScT has shifted to the edge and more dorsal. • At this level, as indeed in most of the others that follow, there are broad, more central regions designated as the brainstem reticular formation (BRF). |
|
|
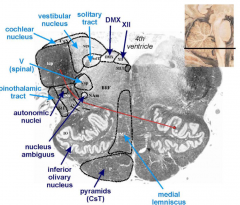
Open Medulla Crossection
|
|
|
|
Open medulla Nuclei
|

|
|
|
Pons Nuclei
|

|
|
|
Pons Crossection
|
lying more lateral to the medial lemniscus, a distinct set of auditory nuclei (Audn;
eg, trapezoid body, superior olivary, nucleus, nucleus of the lateral lemniscus) and the auditory decussation form across the midline (Audx). A distinct MLT is apparent also at this level |
|
|
Pontocerebellar Axons
|
Pontocerebellar axons (PcT) originate from the cells of the pontine nuclei; their axons cross the
midline and enter the cerebellum via middle cerebellar peduncle (mcp). The bulk of the inputs to the pontine nuclei are from the corticopontine tract. |
|
|
Caudal Midbrain
|
Just dorsal to the cp, lies the massive
substantia nigra. This nucleus is made up of 2 major subnuclei called substantia nigra pars reticulata (SNr) and substantia nigra pars compacta (SNc). SNc house the melanin rich dopaminergic cells so crucial in proper motor control. Just medial to the substantia nigra lies another group of dopaminergic cells of the ventral tegmental area (VTA). - superior cerebellar peduncle (scp). cross to the contralateral side at the level of the inferior colliculi (IC) The grey matter of the midbrain appearing dorsal to the cerebral aqueduct and periaqueductal grey is generally referred to as the tectum. - • Surrounding the mesencephalic aqueduct (MAq) lies the periaqueductal grey matter (PAG). |
|
|
Brain stem Blood Supply
|
- paired vertebral aa.
|
|
|
Vertebral aa.
|
These are branches of
the subclavian artery and ascend to the base of the skull by passing through the foramina transversaria of the cervical vertebrae. The vertebral arteries enter the cranial cavity through the foramen magnum and are found on the lateral aspect of the medulla. They pass ventrally and rostrally to unite at the caudal border of the pons, forming the basilar artery most people are left vertebral aa. dominant |
|
|
posterior inferior cerebellar artery
|
• The posterior inferior cerebellar artery (PICA) is a branch of the vertebral artery, given
off a centimeter or so below the pons. It supplies the lateral medulla (dorsolateral to the olive, including the inferior cerebellar peduncle), as well as the ventral surface of the cerebellum. Medially the brainstem is supplied directly by small branches of the vertebral artery; the territory goes at least as deep as the medial lemniscus. |
|
|
anterior inferior cerebellar artery
|
The anterior inferior cerebellar artery (AICA) is a branch of the basilar artery and
occupies the groove between the pons and the medulla; the superior cerebellar artery is also a branch of the basilar and is found towards the rostral end of the pons. The pons is supplied by the basilar artery and the anterior inferior and superior cerebellar arteries. |
|
|
Basilar aa.
|
The basilar artery ends by dividing to form the 2 posterior cerebral arteries. The posterior
cerebral arteries supply the cerebral peduncles and midbrain before passing laterally to the cerebral hemispheres |
|
|
Brainstem BS
|

stroke -85% blockage and 15% rupture
|
|
|
1) Paramedian/basal arteries in the midbrain.
|
damage to the midline
corticospinal and corticobulbar tracts, damage to the reticular formation and loss of the oculomotor nuclei. This can result in the "locked in with ocular palsy" syndrome. The patients typically have sudden onset of vomiting and may have transient loss of consciousness. There is acute onset quadriplegia (corticospinal tracts), bilateral facial paralysis (corticobulbar tracts), loss of speech (corticobulbar tracts for cranial nerve nuclei controlling larynx, pharynx, tongue and lips) and loss of voluntary eye movements (loss of oculomotor nuclei). |
|
|
2) Paramedian/basal arteries in the pons.
|
Occlusion of pontine paramedian/basal arteries also results in damage to the midline
corticospinal and corticobulbar tracts and damage to the reticular formation. The oculomotor nuclei are spared. This can result in "locked in syndrome without ocular palsy" so the patient still has voluntary eye movements. Facial muscles are paralysed due to damage to corticobulbar fibres. |
|
|
3) Superior cerebellar artery
|
Main symptoms are ipsilateral cerebellar ataxias (loss of middle and/or superior cerebellar
peduncles), nausea and vomiting, slurred speech, loss of pain and temperature over the opposite side of the body. Partial deafness, an ipsilateral Horner syndrome. |
|
|
4) Anterior inferior cerebellar artery
|
The second most common brainstem stroke involves the anterior inferior cerebellar artery. It
supplies the more anterior portions of the inferior surface of the cerebellum (e.g., the flocculus). It also supplies parts of the caudal pons. The labyrinthine or internal auditory artery usually takes its origin from AICA and supplies the inner ear. These patients present with sudden onset vertigo, vomiting and falling to one side. They have usually marked horizontal nystagmus but the characteristic features are absent sensation on one side of the face, ipsilateral facial paralysis and ipsilateral hearing loss. They also lean to the affected side when you make them sit. The ipsilateral loss of sensation in the face may easily lead one to make a misdiagnosis of Wallenberg syndrome, ie, the lateral medullary syndrome, but facial paralysis and hearing loss are not features of Wallenberg syndrome. The combination of ipsilateral hearing loss, facial paralysis and loss of facial sensation is a very typical feature of anterior inferior cerebellar artery occlusion syndrome. CN VII is at the pontomedullary junction and the anterior inferior cerebellar artery affects the anterior and inferior part of pons, so it often involves the exiting fibers of the 7th nerve (facial paralysis) and the neighbouring auditory nerve nucleus (ipsilateral hearing loss) and the chief sensory nucleus of V (absent sensation on the face including touch, pain and temperature). Damage to the inner ear may be the cause of the nystagmus and vertigo. |
|
|
5) Posterior inferior cerebellar artery
|
(i) the spinal tract and nucleus of cranial nerve V (loss of pain and temperature sensation on
the ipsilateral side of the face), (ii) nucleus ambiguus - (ipsilateral paralysis of soft palate, pharynx and larynx leading to dysphagia and dysarthria), (iii) vestibular nuclei (leading to vertigo and nystagmus - saccadic dysmetria (overshoot) or saccadic pulsion (pulling of the eye during vertical saccades toward the side of lesion). (iv) contralateral sensory deficit, the spinal lemniscus (contains the crossed spinothalamic tract) is located laterally in the medulla and is damaged by this stroke resulting in loss of pain and temperature sensation on the body below the head. Remember this odd combination of loss of pain and temperature sensation on the ipsilateral side of the head and contralateral side of the body. (v) Ipsilateral ataxia since PICA supplies part of the cerebellum. (vi) Ipsilateral Horner’s syndrome characterised by ptosis, miosis and facial anhidrosis. This is due to due to damage to the descending sympathetic fibres located close to the spinal lemniscus |
|
|
6) Vertebral artery
|
The vertebral arteries supply the lateral section of the medulla and a complete block of this
artery can also result in "Wallenberg Syndrome". The region supplied by the vertebral artery contains the spinal trigeminal nucleus, the inferior olivary nucleus, nucleus ambiguous, sympathetics, and the spinothalamic tract. As a result a blockage of this artery would result in loss of pain and temperature sensation in the ipsilateral face, ipsilateral facial pain (SpV), contralateral pain and temperature loss of the body (spinathalamic tract), ipsilateral ataxia and gait ataxia (IO), hoarseness and dysphagia (NA) and Horner's syndrome. |
|
|
7) Anterior spinal artery
|
The anterior spinal artery supplies the territory which contains the pyramidal tract, the medial
lemniscus and the hypoglossal nucleus. As a result, an occlusion of this artery would result in contralateral weakness of both the upper and lower extremities (pyramidal tract before it crosses), contralateral sensory loss, e.g. vibration, propriception (not pain and temperature), and ipsilateral tongue weakness (hypoglossal nucleus). |
|
|
Crossections Through Medulla
|
A. MEDIAL STRUCTURES:
1. hypoglossal nucleus 2. ML 3. Pyramid B. LATERAL STRUCTURES: 1. NA (CN IX, X, XI) 2. Vestibular nuclei (CNVIII) 3. Inferior cerebellar peduncle (dorsal spinocerebellar, cuneocerebellar and olivocerebellar tracts) 4. L StT (Spinal Lemniscus) 5. Spinal Trigeminal nucleus and tract of CNV |
|
|
Crossection through Pons
|
- dorsal tegmentum and ventral base
MEDIAL: 1. MLF 2. CNVI nucleus (underlies facial colliculus) 3. Genu of CNVII (underlies VII) 4. CNVI fibres 5. ML 6. CsT LATERAL 1. VII nucleus 2. VII fibres 3. Spinal trigeminal nucleus and tract 4. L StT 5. Vestibular nuclei 6. Cochlear nuclei |
|
|
Crossection through Midbrain
|
- has a drosal tectum, intermediate tegmentum and a base
- aqueduct between the tectum and tegmentum DORSAL STRUCTURES: - superior colliculi TEGMENTUM: 1. CNIII nucleus 2. MLF 3. Red nucleus 4. Substantia nigra 5. Dentatothalamic tract (crossed) 6. ML 7. Lateral StT CRUS CEREBRI; CsT in middle 3/5 - also ahs the corticobulbar tract |
|
|
Corticobulbar Fibres
|
project bilaterally to all motor cranial nerve nuceli except facial nucelus.
- the upper face orbicularis oculi and above recieves bilateral corticobulbar input - lower face only recieves contralateral corticobulbar input |
|
|
Brainstem Reticular Formation
2 main functions |
1. Arousal-mood setter (eg hangover to allow repair)
2. Autonomic Policeman: monitors and inturn influences crucial reflexes |
|
|
BRF Pathways
|
1. reticulo-spinal tract; somatic (eg pain) and visceral (eg GIT)
2. Raphe nuclei |
|
|
Raphe Nuclei
|
• LOCALE: raphe nuclei
• CONNECTIONS: all over • FUNCTIONS: - behaviour - mood (depression) - aggression (hypothalamus, amygdala, hippocampus) - pain (inhibits cells in dorsal horns) - blood flow control (causes vasconstriction at high levels and so may be the initiating fator of migraine AURA- due to hypoxia) the resulting vasodilation aggitates V1 causing headache |
|
|
BRF ACh Groups
|
• LOCALE: BRF Ach groups
• CONNECTIONS: all over • FUNCTIONS: - arousal - memory (attention) - ANS control - pain - dreamer |
|
|
BRF DA
|
• LOCALE: substantia nigra, ventral tegmental area
• CONNECTIONS: forebrain • FUNCTIONS: - behaviour regulation - focus (movements and suppresses unwanted moves, eg unable to suppress tremor in PK) - pleasure/motivation Overactivity @ cortex causes +ve Sx of schizo while uderactivity causes -ve Sx of pshyco |
|
|
BRF NA
|
• LOCALE: locus coeruleus
• CONNECTIONS: all over • FUNCTIONS: - ANS control - pleasure/motivation (cocaine and amphetamines stop reuptake of NA & DA) - blood flow control - neural plasticity - global attention (INC. sens. info inputs, preps for emergency) |