![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back
|
Sagittal axis |
Z. Plane: Frontal Motion: abd/ad Rotation: abd/ ad Translation: A/P |
|
|
Frontal axis
|
X. Plane: Sagittal Motion: flex/ext Rotation: flex/ext Translation: M/L |
|
|
Vertical axis |
Y. Plane: Transverse Motion: internal/external rotation Rotation: int/ext rotation Translation: Inferior/Superior |
|
|
Rotation |
Angular, goniometer, degrees. Motion about an axis, |
|
|
Translation |
Linear motion, all parts move in parallel and in same direction. Used to get mov't back. Motion along an axis |
|
|
+Rz |
Right side bend |
|
|
-Rz |
Left side bend |
|
|
+Ry |
Left rotation |
|
|
-Ry |
Right rotation |
|
|
+Rx |
flexion |
|
|
-Rx |
extension |
|
|
+Tx |
Left lateral glide |
|
|
-Tx |
Right lateral glide |
|
|
+Ty |
Superior glide |
|
|
-Ty |
Inferior glide |
|
|
+Tz |
Moving posterior to anterior |
|
|
-Tz |
Moving anterior to posterior |
|
|
Frontal plane |
Axis: Sagittal, Z. Motion/Rotation: abd/add Translation: A/P |
|
|
Sagittal Plane |
Axis: Frontal, X. Motion/rotation: flexion/extension. Translation: M/L |
|
|
Transverse plane |
Axis: Vertical, Y. Motion/rotation: int/ext rotation Translation: Inferior/Superior |
|
|
Degrees of freedom |
# directions allowed at a joint. Up to 3 in rotation and 3 in translation. Every joint will have 6, it will just vary how many are voluntary or involuntary. GH 3 involuntary 3 voluntary PID 1 voluntary 5 involuntary |
|
|
Arthrokinematics |
motion that occurs b/n joint surfaces. Roll, slide, glide. Look at distal on proximal. |
|
|
Roll |
Tire on ground, many points coming into contact with many new points. Always follows bone motion. Flexing the shoulder (superior) roll of humerus is superior |
|
|
Slide |
Skid, 1 point coming into contact with multiple points |
|
|
Spin |
1 point on 1 point |
|
|
Accessory mov'ts |
joint play, passive slight mov'ts |
|
|
Convex on concave |
Roll and glide are in opp directions. Shoulder is an example |
|
|
Concave on convex |
Roll and glide are in the sAme direction. Elbow |
|
|
Closed pack position |
maximal tension, cannot use traction to pull out, avoid testing strength here, easy to hide a weal prime mover |
|
|
loose packed position |
any other position, least amount of stress, decreased pain, there may be some joints where there are positions that are the loosest. |
|
|
kinetics |
describes effects of forces on the body. |
|
|
types of forces |
Tension, compression, bending, shear, torsion, combined |
|
|
Stress |
force, internal |
|
|
Strain |
length of stretch |
|
|
Non linear region |
Toe region, neutral zone. Removing the wave from the tissue, does not take much force |
|
|
Elastic deformation |
range the tissue will return to original length. Elastic zone |
|
|
Plastic deformation |
Plastic zone. area where there is damage, does not return. Laxity, Microdamage first. If damage the subsequent toe region will be larger, yield point still equal |
|
|
Creep |
progressive strain over time in viscoelastic material. |
|
|
Internal forces |
within, muscle contraction or passive strethc |
|
|
External forces |
Gravity of physical contact |
|
|
Torque |
force x moment arm, usually causes rotation |
|
|
Moment arm |
perpendicular distance from axis of rotation and the force. Internal and external |
|
|
Joint reaction force |
created b/n surfaces of joint, = to diff b/n muscle F and external F |
|
|
Concentric |
muscle shortening |
|
|
Eccentric |
muscle lengthening. can only happen with gravity |
|
|
1st class lever |
Axis is in the center, forces are on either side. the mechanical advatage can be >1, <1, or =1. Forces usually act in the same linear direction but produce torques in the opp |
|
|
2nd class lever |
Axis is at the end, the external force is closer to the axis and the internal force is farther away. MA>1 IMA>EMA. With the MA being >1 the system is able to balance with an interanal force LESS than the external one. Going up on tip toes, designed for power |
|
|
3rd class lever |
Axis is at the end, the internal force is closer and the external force is farther away. MA<1, IMA |
|
|
Mechanical advantage |
IMA/EMA |
|
|
Force couple
|
2 or mor muscles simutaneously produce forces in different linear direction, although the resulting torques act in the same rotary direction. Like 2 hands on the steering wheel. |
|
|
Kinematics |
branch of mechanics that describes the motion of the body w/o regard to torques and forces |
|
|
Fibrous joints |
Suture, gomphosis - fibrous CT for both. Syndesmosis- interosseous ligament |
|
|
Cartilaginous joints |
Synchondrosis (primary), hyaline cartilage, temporary and permanent. Symphysis (secondary)- fibrocartilage in the form of a disc |
|
|
Diarthrosis joints |
Uniaxial- hinge, pivot. Biaxial- saddle, condyloid. Triplanar- ball and socket, plane |
|
|
Classification of joints based on shape |
Ovoid, saddle, and plane |
|
|
Ovoid joint shape |
one surface is convex and the other is concave |
|
|
Saddle joint shape |
each joint surface is concave and convex |
|
|
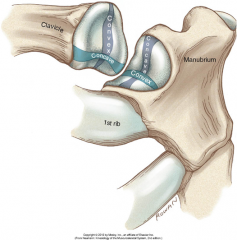
Clavicle shape |
convex medially, concave laterally |
|
|
Head of humerus angle |
angle of inclination is 135 degrees, and 30 degrees of retroversion |
|
|
Sternocalvicular joint mov'ts |
Elevation (convex on concave, sup roll, inf glide of c on s) Depression (inf roll, sup glide) Sagittal axis. Protraction (cave on vex, c on s, roll/slide post) Retraction (roll/slide ant) Vertical axis. Post/Ant rotation (spin), frontal axis. Post rot= inf part of c faces ant |
|
|
Ligaments of the SC |
Anterior and posterior sternoclavicular ligaments, interclavicular ligament, costoclavicular ligament |
|
|
Anterior and posterior sternoclavicular ligament |
Criss cross as a whole, limit elevation. Ant limits retraction, post limits protraction |
|
|
Interclavicular ligaments |
limits depression |
|
|
Costoclavicular ligament |
limits elevation to 25 degrees |
|
|
Acromioclavicular mov't |
no arthrokinematic motion. Mov't of AC is mov't of scap at acromial end of scap. Sagittal axis- upward rot (inf angle lat, glenoid point up) downward rot (medial, down). Vertical axis- IR (medial border goes post) ER (goes ant) Frontal axis- ant tilt (inf ang post) post tilt (ant) |
|
|
AC ligaments
|
Superior and inferior acromioclavicular ligaments, Coracoclavicular ligaments (trapezoid, conoid)
|
|
|
Superior and inferior acromioclavicular ligaments |
stabilize SC |
|
|
Coracoclavicular ligaments |
trapezoid, conoid. really important. extracapsular
|
|
|
shoulder separation |
occurs at AC, dislocation, but not called that |
|
|
scapular plane |
35 degrees ant to frontal plane |
|
|
scaption |
movement in the scapular plane |
|
|
Scapulothoracic joint |
not a true joint, moves in scaption. 2:1 GH:ST degrees of mov't. upward rotation 180, 120 from GH, 60 from ST- 25 from CS and 35 from AC. All mov't are cooperation b/n AC and SC. |
|
|
Glenohumeral joint mov'ts |
Frontal axis- flex/ext (spin) Sagittal axis- abd, add (abd sup roll inf glide, add inf roll sup glide) w/o inf glide, only 22 Vertical axis- IR, ER (IR roll ant glide post, ER roll post, glide ant) |
|
|
Coracoacromial arch |
subacromion space 10mm. Subacromial bursa, supraspinatus tendon, LHBB, superior shoulder capsule floor, superior part of humerus head |
|
|
rotator interval |
no muscle b/n supra and sub. LHBB, coracohumeral, superior GL, common site for ant dislocations |
|
|
ligaments of GH |
superior glenohumeral ligament, middle glenohumeral ligament, inferior glenohumeral ligament, Coracohumeral ligament
|
|
|
Coracohumeral ligament |
Coracoid to greater tubercle, blends w/ superior capsule and supra tendon. Limits add, inferior translation, ER. |
|
|
Superior glenohumeral ligament |
Supraglenoid tubercle to anatomical neck above the lesser tubercle. Limits add, inferior and A/P translations, ER |
|
|
Middle glenohumeral ligament
|
Supraglenoid tubercle and anterior/superior glenoid to medial to lesser tubercle and anatomical neck, Limits ER and ant translation
|
|
|
Inferior glenohumeral ligament |
Runs from 4pm on the anterior glenoid to 8pm on the posterior glenoid and that inserts on the anterior/inferior margins of the anatomical neck of the humerus. Axillary pouch b/n bands connects. All fibers limit abd, ant limits ER especially @ 90abd and ant translation. Post limits IR especially @ 90abd and post translation |
|
|
Scapula resting position |
0 upward rotation, 10 ant tilt, 35 IR |
|
|
SC rest position and in 180 abd/scaption/flex |
0 elevation/depression 0 retraction/protraction 0 post rot. 25 elevation, 15 retraction, 25 post rot |
|
|
ST rest position and in 180 abd/scaption/flex |
0 upward rotation, 10 ant tilt, 35 IR. 60 upward rotation (25 SC, 35 AC), 10 post tilt, 25 IR |
|
|
GH in rest position and in 180 abd/scaption/flex
|
0 abd/add, 0 flex/ext 0 IR/ER. 120 abd, 120 flex, 45 ER usually accompanies abd |
|
|
AC rest position and in 180 abd/scaption/flex
|
0 upward rotation, 10 ant tilt, 35 IR. 35 upward rotation, 10 post tilt, 25 IR |
|
|
SC elevation |
25. sagittal axis, frontal plane. Upper trapezius |
|
|
SC retraction |
15. vertical axis, transverse plane. Middle Trapezius |
|
|
SC posterior rotation |
25. frontal axis, sagittal plane. 3 things must happen: 1. upper rotation of the scapula by the serratus antetior, upper and lower trapezius 2. tension of the coracohumeral ligament 3. posterior rotation of clavicle |
|
|
ST upward rotation |
60. upper and lower trapezius, serratus anterior. sagittal axis, frontal plane |
|
|
ST post tilt |
20. serratus anterior. Frontal axis, sagittal plane |
|
|
ST ER |
10. serratus anterior. vertical axis, transverse plane |
|
|
GH abd |
120. Supraspinatus- rolls head superiorly. Deltoid. Subscapularis, inrfrapsinatus, teres minor- inferior glide. sagittal axis, frontal plane |
|
|
GH flexion |
120. Supraspinatus- rolls head superior. Deltoid. Subscapularis, infraspinatus, teres minor- inferior glide. frontal axis, sagittal plane |
|
|
GH ER |
45. Posterior deltoid, infraspinatus, teres minor (roll), Tight posterior capsule cause ant glide, subscapularis and MGHL cause the anterior glide. vertical axis, transverse plane |
|
|
AC upward rotation
|
35. upper and lower trapezius, serratus anterior, Sagittal axis, frontal plane |
|
|
AC posterior tilt |
20. serratus anterior. frontal axis, sagittal plane |
|
|
AC ER |
10. serratus anterior. vertical axis, transverse plane |
|
|
Accessory nerve |
Trapezius |
|
|
Lower subscapular nerve |
Subscapularis and teres major |
|
|
Suprascapular nerve |
Supraspinatus and infraspinatus |
|
|
Thoracodorsal nerve |
Latissimus dorsi |
|
|
Axillary nerve |
Deltoid and there's minor |
|
|
Dorsal scapular nerve |
Levator scapulae and rhomboids |
|
|
Long thoracic nerve |
Serratus anterior |
|
|
Musculocutaneous |
Biceps and coracobrachialis |
|
|
Medial pectoral nerve |
Pec major and minor |
|
|
Lateral pectoral nerve |
Pec major |
|
|
Nerve to subclavius |
Subclavius |
|
|
Radial nerve |
Triceps |
|
|
Upper subscapular nerve |
Subscapularis |
|
|
suprascapular notch |
the suprascapular nerve runs through here. Superior transverse scapular ligament goes over it. Swelling here leads to loss of abd and ER |
|
|
spinoglenoud notch |
where the suprascapular nerve runs as it goes around the spine to the infrspinatus m. swelling here leads to loss of ER |
|
|
contractions and force |
highest in fast eccentric, sloe eccentric, isometric, slow con, fast con |
|
|
glenoid faces |
4 degrees superiorly and 35 degrees anterio-lateral |
|
|
humerus faces |
medial, superior, posterior |
|
|
Subclavius |
Depression of clavicle and scapula |
|
|
Pectoralis minor |
Depression, protraction, downward rotation, IR, anterior tilt |
|
|
Serratus anterior |
Protraction(mid to low fibers w/ IR), UR, ER, posterior tilt |
|
|
Trapezius |
Superior- elevate, retract, UR. Middle- retract (stabilizes against protraction in scaption) Inferior- depression, retraction, UR |
|
|
Rhomboids |
elevate, retract, downwardly rotate |
|
|
Latissimus dorsi |
depression of scapula, ext, add, IR of arm |
|
|
Levator scapulae |
elevation, retraction, downward rotation |
|
|
static locking/static stability |
Superior capsular structures provide a slight upward rotation of the humerus, w/o it will translate inferiorly and creep leading to instability and impingement. Superior capsular ligament, coracohumeral ligament, tend of supraspinatus. Compression force. Superior GHL, coracohumeral |
|
|
centralization |
keeping a point on the humerus centralized in the fossa. w/o glide off of fossa. Critical for abd/add and IR/ER. Importance of capsule. Too tight anteriorly- humeral head too far posteriorly. Too tight posteriorly- too far anteriorly (more common) |
|
|
GH IR |
anterior roll- subscapularis, pec major, lats, teres major, ant deltoid. Tight ant capsule leads to glide posteriorly. Posterior inferior GHL |
|
|
wheelchair/ crutch walking |
the lats, lower traps, and pec minor act in reverse to instead elevate the thorax to fixed arms |
|
|
GH strength |
extensors, adductors, flexors, abductors; IR, ER |
|
|
grade 1 shoulder separation |
sprain of the S/I AC ligaments- no visible separation, just pain and tenderness, early plastic zone |
|
|
Grade 2 shoulder separation |
tear of S/I AC ligaments and sprain of the coracoracoclavicular, visible superior separation, higher |
|
|
grade 3 shoulder separation |
tear of S/I AC ligaments and coracoclavicular ligaments, superior separation |
|
|
grade 4 should separtaion |
Grade 3. tear of S/I AC ligaments and coracoclavicular ligaments, posterior separation |
|
|
grade 5 shoulder separation |
grade 3. tear of S/I AC ligaments and coracoclavicular ligaments, significant superior separation |
|
|
grade 6 superior shoulder separation |
grade 3. tear of S/I AC ligaments and coracoclavicular ligaments, inferior separation |
|
|
SLAP lesion |
superior labrum anterior posterior. Sx. Impingement of LHBB |
|
|
Bankart lesion |
tear of anterior inferior glenoid labrum due to anterior shoulder dislocation |
|
|
parts of a synovial joint |
synovial fluid, membrane, articular cartilage, joint capsule, ligaments, blood vessels, sensory nerves. Innervated except cartilage and fluid |
|
|
stability of the GH joint |
Active and passive mechanisms. Active- RC muscles and others. Passive- restraint from capsule, ligaments, labrum, tendons.. mechanical support from ST posture.. negative intracapsular pressure |
|
|
mov't in scapular plane |
Puts GT into the high part of the subacromial arch and puts the supraspinatus into a straight pull, increases force |
|
|
upper trap paralysis |
superior subluxation of SC, depressed clavicle, looses static locking |
|
|
oreintation of the clavicle to the frontal plane
|
20 degrees posterior
|
|
|
Infrapsinatus and Teres minor |
ext, add, ER |
|
|
Subscapularis and teres major
|
ext, add, IR
|
|
|
Biceps brachii |
LH- fl SH- fl, add, IR |
|
|
Coracobrachialis |
fl, add, IR |