![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
111 Cards in this Set
- Front
- Back
|
what questions should you ask during a skin history? |
- previous history of skin disease (allergies, hives, psoriasis, eczema), - change in pigmentation - change in a mole - excessive dryness or moisture - pruritus - excessive brusing: is it r/t injury? - rash or lesion - medications - hair loss - change in nails - environmental or occupational hazards - self care behaviors - previous family hx |
|
|
how do you determine how long a patient has had an itch, rash, skin injury, ect? |
ask the patient specifically what time the skin condition started because it will give you a better idea of how many hours (or days) it's been. |
|
|
how do you describe a skin lesion? |
- distribution/location: what part of the body? - configuration: christmas tree, circular, angular - color - morphology: shape it's in - symmetry: uniform, multiform, polygonal (many different sides) - size: in cm, width x height - borders: demarcated, raised, ill defined - surrounding tissue: induration, erythema, flaking, scaling. Determine if the tissue is hard, feel if underneath it is indurated. Measure if erythema around edges, 3 cm around it |
|
|
induration |
hardened mass or formation |
|
|
morbiliform |

macular lesions that are red, usualy 2- 10 mm in diameter. Looks like measles |
|
|
papulosquamous |
condition that presents with both papules and scales |
|
|
coalesce |
grouped together (ie herpes) |
|
|
exantham |
wide spread rash associated with a virus |
|
|
erythroderma |
body is very red, widespread |
|
|
scarletinform |
ie macular rash |
|
|
confluent |
a rash that runs together |
|
|
distrubtion or location |
- acral - dermatonal - extensor - flexor - flexural (intertriginous) - follicular - generalized - herpetiform - photosensitive - pressure area - seborrhoeic - symmetrical - truncal - unilateral |
|
|
acral |
distal parts of limb |
|
|
dermatonal |
rash that appears along a dermatome |
|
|
extensor flexor |

remember that flexors are where the folds of skin meet |
|
|
flexural (intertriginous) |
bt the fingers |
|
|
follicular |
in the hair follicle |
|
|
seborrhoeic |
rash appears in those areas of skin wth large amount of grease (sebaceous) glands like the scalp and the nose |
|
|
think of the linear configuration. give an example or two |

contact dermititis, poision ivy. remember that it's the oil from the leaves that causes rash |
|
|
nummular |

think coin shaped |
|
|
target |

found in erythema multiform, skin rxn that can occur asa reaction to antibiotics |
|
|
gyrate |

lacy rash ex: fifths disease |
|
|
annular |

doesn't have to be circular |
|
|
satellite lesions |

redness, yeast rash in candida in folds in flexor but could be in groin |
|
|
carotenaemia |

excess of beta carotene |
|
|
where does jaundice start? |
in the eyes |
|
|
hyperpigmentation hypopigmentation
|
more color than usual less color than usual |
|
|
leukoderma |
vitiligo, localized loss of pigmentation of the skin that could occur after any number of inflammatory skin conditions, burns, etc |
|
|
infarcts |
a small, localized area of dead tissue resulting from failure of blood supply |
|
|
violaceous |
descriptor meaning "violet" |
|
|
macule |

- a circumscribed, flat, nonpalpable, change in skin color - up to 1 cm example: frckles, fat nevi, hypopigmentation tinea, versicolor, petechiae, measles, scarletina rash associate with strep infection |
|
|
patch |
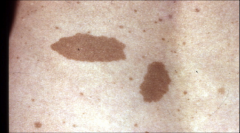
- a macule larger than 1 cm example: senile lentigo (liver spots), mongolian spot, vitiligo, cafe au lait spot |
|
|
papule |

- a palpable, elevated, circumscribed, solid mass - caused by superficial thickening in the epidermis - up to 1.0 cm example: elevated nevus, lichen planus, wart, molluscum, bug bite |
|
|
plaque |

- a falt, elevated surface - larger than 0.5 cm - often formed by coalescence of papules - example: psoriasis, lichen planus, xanthoma, xanthelasma |
|
|
psoriasis |

- common chronic inflammatory papulosquamos disease of unknown etiology - common presentation is red, sharply defined, scaly papules that coalesce to form stable round to oval plaques - scale is adherent, silvery, white - may have nail and or joint disease |
|
|
nodule |

- a solid, elevated, firm or soft mass less than 1-2 cm - may be firmer and extend deeper into the dermis than a papule example: fibroma, intradermal nevi |
|
|
nevi |
mole common aquired nevi occur after 6 months of age increase in number in children and adolescent peak at 30 and then regress
|
|
|
tumor |

- a solid, elevated firm or soft mass larger than 1-2 cms - extending deeper into the dermis - benign or malignant - lipoma, hemangioma |
|
|
hemangioma |
vascular tumor around birth |
|
|
wheals/ uticaria/ hives |
- superficial, raised, erythematous, transient lesion with somewhat irregular borders due to localized edema - multiple wheals/hives can coalesce to cause an intensely puritic lesion - fluid is held diffusely in the tissues example: allergic reaction, bug bite, strep |
|
|
vesicles |

- a circumscribed, superficial, elevated cavity - contains free fluid - clear fluid flows if wall ruptured - up to 1 cm in size example: herpes simplex, chicken pox, contact dermatitis, herpes zoster |
|
|
bulla |

- similar to vesciular lesions but usually larger than 1 cm - filled with serous fluid - can be caused from bug bite or bullous pemphigus |
|
|
pustule |

- purulent vesicle - filled with neutrophils and may be white or yellow - not all pustules are infected example: acne infections can be inflammatory, s. aureus |
|
|
burrow |

- a minute, slightly raised tunnel in the epidermis, commonly found on the finger webs and the fingers - burrowing will usually end with a papule, vesicle or pustule - burrowing is found in scabies - scabes is rarely found on the face ex in infants and the elderly. - make sure to check bt the fingers |
|
|
secondary lesions |
primary lesions got worse and became secondary lesions |
|
|
lichenification |

constant rubbing or scratching |
|
|
crusting |

may be yellow or black plasma that exudes |
|
|
distrophy |

abnormal formation of the skin |
|
|
excoriation |
skin abrasion due to scratching |
|
|
scale |

a thin flake of dead exfliating epidermis |
|
|
fissure |

thin crack within epidermis or epithelium and is due to excessive dryness crack within epidermis or epithelium |
|
|
ulcer |

you already know about pressure ulcers |
|
|
erosion |

slightly depressed areas of skin where epidermis has been lost erosion, partial thickness |
|
|
hypertrophy (keloid) |

hypertrophy, excessive growth of dense fibrous tissue that usually develops after healing of a skin injury - tissue extends the borders of the original wound and does nto regress spontaneously
hypertrophic scars are red, itchy, raised fibrous lesions that do not expand beyond boundaires of the initial injury |
|
|
granduloma |

chronic inflammation, usually in response to infection |
|
|
petechia |
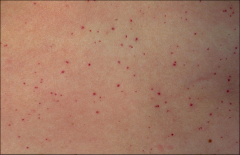
- small 1-3 mm deep red or reddish purple macules - rounded sometimes irregular in shape - indicates blood outside of the vessels -petechia do not blanch someone has redness, take a piece of glass to see through. if it blanches then it's erythema. no blanching >> intravascular |
|
|
pupura/ecchymosis |

- a larger macule or papule of blood in the skin - purpurae- from 0.5 - 1 cm - ecchymoses: more than 1 cm if found on exam it may be benign resulting from trauma or pathological |
|
|
meningoccol infection |

- presents as sudden onset of fever, rash and signs of meningeal inflammation - time from onset to sepsis can be less than 24 hours - kernig sign - brudzinski sign - worrisome signs on presentation are leg pain, cold hands and feet, abrnomal skin color such as pallor indicating onset of sepsis |
|
|
henoch-schonlein purpura |
- IgA vasculitis - 90% of cases are in kids (why in this class?) - self limiting - tetrad of clinical manifestations: palpable purpura, arthritis/arthralgia, abdominal pain, renal disease |
|
|
hypersensitivity vasculitis |
- age > 16 years - use of a possible offending drug in temporal relation to the symptoms - palpable purpura maculopapular rash - biopsy of skin lesion showing neutrophils |
|
|
immune thrombocytopenia purpura |
- isolated thrombocytopenia - precedental viral illness - development of self- reactive antibodies - petechiae, purpura and easy bruising are expected - epistaxis, gingival bleeding and menorrhagia are common
|
|
|
atopic dermatitis |
more localized and lichenified, similar distribution as childhood or primarily on the hands and feet
thickened skin, increased skin markings, hyperpigmentation |
|
|
nummular dermatitis |
- puritic patches of eczematous dermatitis - evidence of papules, scaling and slight crusting - 1-50 lesions - etiology unknown - each tends to be circular or "coin shaped" measuring 2-10 cm - usually trunk and lower extremities - head is spared - differential dx: tinea corporis |
|
|
seborrheic dermatitis |
- erythemic, scaly plaques w/ some puritius - margins not as sharply demarcated as seen in psoriasis - dandruff of scalp, mild form of serborrheic dermatitis |
|
|
allergic contact dermatitis |
- delayed- type hypersensitivity reaction caused by skin contact with allergen - poison ivy, sumac and oak are most common causes of allergic contact dermatitis - characterized by vesicles, edema, redness and often pruritus - usually in a linear presentation |
|
|
stasis dermatitis |
- ecxematous dermatitis of the legs - associated with edema, varicosed/ dilated veins and hyperpigmentation - dry, fissured, erythematous skin - edema, brown discoloration, erosion or ulceration is common |
|
|
rosacea |
- chronic and relapsing inflammatory skin disorder - involves the central face - occurs in adults 30-60 years of age - facial erythema, telengictasias and inflammatory skin lesions - triggers - no cure, treatment focused on symptom suppression |
|
|
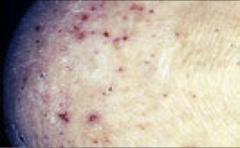
acne vulgaris |
has open and closed comodones |
|
|
imetigo |
- s. aureus and strep are usual culprits - causes superficial vesciles or pustules which cause erosions resulting in golden- yellow crusts - highly contagious tx with antibiotic |
|
|
celluitis |
- acute, diffuse spreading edematous, supprative inflammation of the dermis and subcuttaneous tissue - usual gram + organism like staph or strep - mode of infection may be pre-exisiting, lesion, bug bite or shot - warm, hard, tender to palpation |
|
|
folliculitis |
- upper portion of hair follicle - follicular papule, pustule, erosion or crusting - usually gram + organism - predisposing factor: shaving hairy regions loofah w/ antibiotic soap
1 mm perifollicular red papule or pustule areas of sweat or abrasions tx: tetracycline or erythromycin, 500 mg 2x/day |
|
|
hot tub folliculitus |
multiple follicular pustules on trunk appear days after going in a hot tub, causative organism is P. aeruginosa, lesions resolve spontanelously in a week |
|
|
furuncle (boil) |
deep dermal or subq, red swollen and painful mass that drains through multiple openings
about 1 cm tender red papule or fluctant nodule areas of sweat and abrasion deep, tender, painful, any hair bearing site sites of high friction and sweating most typical 1. incise and curettage 2. dicloxicillin 250 mg 4x/day for 10 days |
|
|
carbuncle |
deep, tender, firm subcutaneious erythematous papules enlarge to deep nodules - several cm diameter red plaque - nape of neck 1. incise and curettage or excise 2. dicloxicillin 250 mg 4x/day for 10+ days or rampin for 10+ days |
|
|
syphilis |
- secondary syphilis occurs 2-6 months after primary - presence of papulosquamous rash usually on the trunk, palms and soles
|
|
|
rashes that can be on palms |
infectious enterovirus ie coxsackie syphyilis rocky mountain fever
noninfectious: atopic dermatitis, contact dermatitis, drug eruption, erythema multiforme, palmar and plantar keroderma, psoriasis, tinea
|
|
|
tinea or dermophytosis |

- dermatophytes are fungi capable of infecting skin, nail and hair - tinea is used for dermophytosis and is modified according to the anatomic site of infection |
|
|
name the location tinea pedis tinea crurus tinea manuum tinea corporis tinea facialis tinea capitis |
dermatophytes are fungi capable of infecting skin, nail and hair tinea pedis - athlete's foot bt toes tinea crurus- jock itch tinea manuum- creases on the palm can be red tinea corporis- ringworm tinea facialis - face tinea capitis - hair |
|
|
tinea corporis |
ring worm - puritic circular or oval erythematous scaling patch or plaque - spread centrifugally - central clearing follows - borders well delineated and red - multiple lesions may run together - differential dx nummular eczema
|
|
|
tinea versicolor pityrasis versicolor |

caused by yeasted called malassezia - numerous small, circular, white, scaling papules on the upper trunk - may involve the upper arms, neck and abdomen - lesions are hypopigmented in tanned skin and pink or salmon colored in untanned skin |
|
|
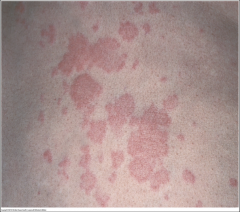
pytoriasis rosea |

often confused with syphilis - usually occurs b/w the ages of 10-30 - self limited rash that is preceded by a "herald patch" - differential dx: secondary syphilis due to similar truncal presentation, age, papulosquamous lesions - rash has a christmas tree distribution - hyperpigmented rash in dark skinned individual -differential dx: syphillis |
|
|
molluscum contagiosum |
- self limited viral infection, poxvirus - characterized by skin colored papules that are often umbilicated (having a small impression like a naval) - occuring in children and sexually active adults - it is transmitted skin to skin contact |
|
|
varicella/ chicken pox |
- incubation 15 days after exposure - prodrom fever, malaise, pharyngitis, loss of appetite - 24 hours later, vesicular rash - rash puritic, successive crops over several days - usually starts on trunk - new vescile formation usually stops after 4 days
vesicles are at different stages of healing - fully crusted by day 6 |
|
|
varicella/shingles/ herpes zoster |
vaccinate at age 60 - erythematous papules that quickly develop into grouped vesciles or bullae - 3-4 days become pustular or hemorrhagic - crusting 7-10 days - follows usaally one dermatome and does not cross the midline - acute pain can lead to chronic pain can have chronic nerve pain |
|
|
acanthosis nigricans |
increased insulin, may not be diabetic yet - hyperpigmented, velvety plaque on the skin - intertiginous sites such as neck, axilla are common - can be acquired due to insulin resistance or inherited with familar acanthosis nigricans |
|
|
erythema multiforme |

- acute, immune - mediated condition - distinctive target-like lesions - multiforme, describes the myriad clinical manifestation that may be observed - target lesions: dusky central area or blister, dark red inflammatory zone, surrounded by a pale ring of edema and arythematous halo
extreme is stephen johnson's syndrome |
|
|
erythema migrans |

80% lyme disease tick bite, bullseye well demarkated line any place with increased exposure to lyme you just treat with lyme doesn't have to be where the person was bitten |
|
|
lichen planus |
uncommon but its presence puts pt at increased risk for oral cancer - lichen plantus (LP) is a chronic inflammatory disorder that affects the skin, oral cavity and genitalia - skin: flat, topped polygonal papules - occasionally puritic - etiology unknown: felt tobe immunological response - self limiting - may persist for months or years |
|
|
acrochordon/ skin tags |
- soft, skin colored or tan or brown, - round, oval or pedunculated, - usually in intertiginous areas of neck and eyelids |
|
|
seborrheic keratosis |
- hereditary lesions, do not appear until age 30 - surface may be smooth, velvety or verrucous - lesions are usually papules or plaques
|
|
|
premalignant skin lesions actinic keratosis scalp? |
- single or multiple discrete, dry, rough adherent scaly lesions occur on habitutally exposed skin - may develop into squamous cell carcinoma more in white people than black people slowly related to sun exposed adults that are burned on the nose, tips of ears |
|
|
squamous cell carcinoma |
variety of clinical presentations fair skinned adults >60 can metastasize tend to grow thick, pink patch, plaque, irregular and it bleeds |
|
|
basel cell carcinoma |

- most common type of skin cancer - locally invasive, aggressive destructive lesion - rises from the basal layer of the epidermis - limited capacity to metastasize remove it |
|
|
melanoma |
aggressive, spreads to any organ in the body in contrast to skin cancers
four types |
|
|
four types of melanoma |
- superficial - most common - nodular - lentigo - acral lentiginous |
|
|
signs of malignant melanoma |
A - asymmetry in shape: one half unlike the other half B- border is irregular: edges irreguarly scalloped C- color: mottled-- haphazard display of color; shades of brown, black, gray, red and white D- diameter: unususally large, greater than the tip of a pencil eraser (6.0 mm) E- evolving (elevation): change in size, shape, surface, shdades of color or symptoms |
|
|
nail assessment |
- shape contour - consistence - color |
|
|
hair - inspect and palpate |
1. color 2. texture 3. distribution 4. lesions
also if it's groomed, clean |
|
|
androgenetic alopecia |
balding for women, it's balding around the hair line |
|
|
alopecia areata |
usually starts at childhood and is genetic - is a chronic inflammatory disordert hat causes non- scarring hair loss - rapid onset in a sharply defined, usually round or oval area - the loss may be diffuse, patchy or band-like at the margins of the scalp - autoimmune and can be associated with thyroiditis and vitiligo |
|
|
tinea capitis |
- round, scaling patches of alopecia - hairs are broken off - usually a fungal infection - differs fro alopecia areata in that the hair follicle is still present - mimics seborrheic dermatitis |
|
|
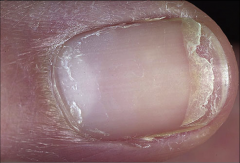
beau's line |

could be from an injury or scarlet fever |
|
|
melanonychia |

can occur with dark skin or r/t subangula melanoma |
|
|
cracked nails |
could be a symptom of hypothyroidism r/t yellowing or thickening think tinnea |
|
|
terry nails |

decrease in vascularity and increase of connective tissue frequently occurs with hyperthyroidism |
|
|
paronychia |
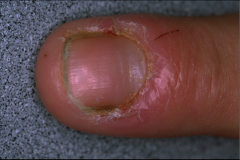
- acute: bacterial infection of the proximal and laternal nail fold - rapid onset of pain and swelling - pus accumulates behind cuticle - chronic irritant exposure topical antibiotic |
|
|
pitting |
- incidence of nail involvement in psoriasis varies 10-59% nail involvement may be only sign can be r/t reiter's syndrome sarcoidosis, alopecia areata
|
|
|
tic behavior |
ridges from pushing back on cuticle, anxiety disorder |
|
|
oncychomycosis |

- fungal infection of the finger or toenail plate - many species of fungus, tends to be a dermatophyte - nail surface is soft, dry and powdery and can easily be scraped away - nail bed is raised |
|
|
derm assessment questions for the elderly |
what changes have you noticed in your skin the last few years? Any delay in wound healing? Any change in feet, toenails? Any bunions? Is it possible to wear shoes? Do you experience frequent falls? Any history of diabetes, peripheral vascular disease? What do you do to care for your skin? |
|
|
what do you see in the elderly? |
- more wrinkling - senile purpura - dry skin (xerosis) - senile lentigines (liver spots) |