Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
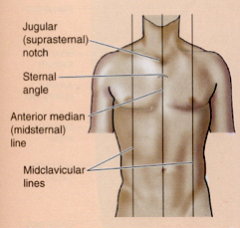
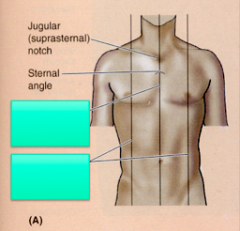
Anterior Median (midsternal) Line- vertical line through sternum in mid-saggital plane
Midclavicular Lines (MCLs)- vertical through midpoints of the clavicles, parallel to median line |
|
|
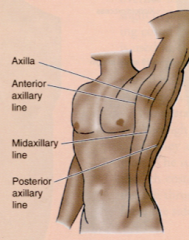
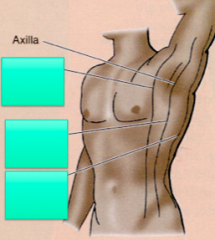
Anterior axillary line- vertical line along anterior axillary fold (formed by pec major)
Mid Axillary Line- vertical line through apex of axilla Posterior axillary line- vertical line though posterior axillary fold (formed by latissimus dorsi and teres major) |
|
|
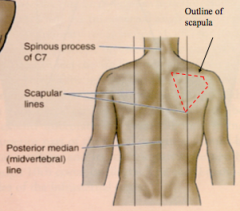
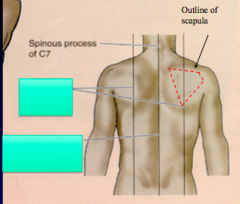
Posterior median (mispinal or midvertebral) line- vertical line through spinous process of vertebrae in mid-saggital plane
Scapular lines- vertical lines that pass through inferior angles of the scapula, line is parallel to the posterior median line |
|
|
Thoracic Wall
|
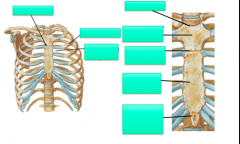
Bones of the thoracic wall- ribs, thoracic vertebrae and sternum
Function- protect thoracic content (heart, lung, blood vessels, esophagus) |
|
|
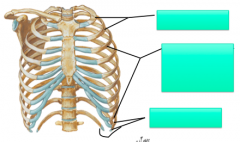
True Ribs
|
1-7, attach "directly" to sternum
|
|
|
False Ribs
|
8-10, attach "indirectly" to sternum
|
|
|
Floating Ribs
|
11-12, do not attach to the sternum
|
|
|
|
|
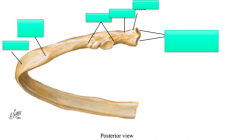
|
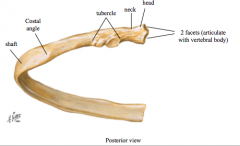
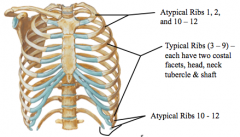
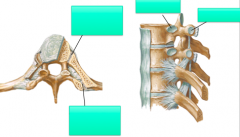
Head- has two facets, Neck, Tubercle (articulates with transverse proces), shaft (thin flat, curves)
Costal angle- MC site of rib fracture, weakest point of rib |
|
|
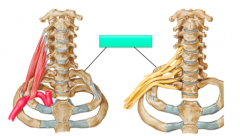
Cervical Rib
|
|
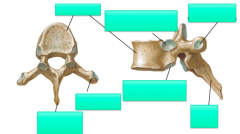
|
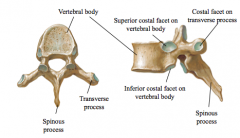
1. costal facets along vertebral bodies (2 on each side except lower 3 thoracic vertebrae)
2. costal facets along transverse processes (except lower 2-3 thoracic vertebrae |
|
|
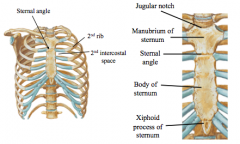
3 segments: manubrium, body and zyphoid process
manubrium- jugular (supersternal) notch, articulations iwth clavicle and 1st rib Body- articulates with the manubrium, forms the sternal angle (bifurcation of trachea/carina, beginning and ending of aortic arch, palpation of sternal angle is location for 2nd rib) Xiphoid Process- might be cartiliginous or ossified, site of subcostal (infrasternal) angle |
|
|
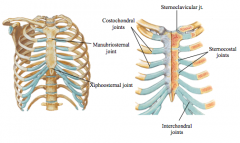
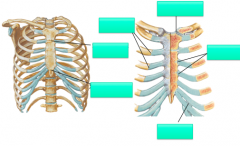
Major-
costochondral joints, sternocostal (articulation between costal cartilage and sternum), sternoclavicular joint (contains disc- critical for shoulder girdle function) Minor: Interchondral joints (articulation between costal cartilage of lower ribs) Manubriosternal joint ("sternal angle") Xiphosternal (junction of xiphoid and sternum) Intervertebral joints of thoracic spine |
|
|
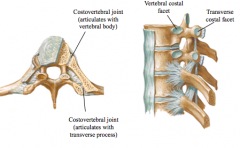
Major joint-
includes articulation with vertebral (and TP where appropriate) |
|
|
Movements of Thoracic Wall
|
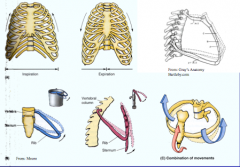
inspiration- increase in AP and transverse diameter of rib cage d/t bucket handle motion of ribs
|
|
|
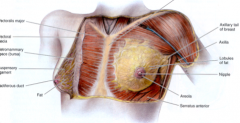
Male- clinical landmark, nipple lies at 4th intercostal space (betw 4 &5)
Female- Circular base extends from sternum to MAL (mid-axillary line), ribes 2-6 Glandular (approx 15-20 lobes drain into ducts) and adipose tissue Axillary tail of brests- extends along inferior border of pec towards the axilla Understanding of the anatomy is critical for optimal clinical exam of potential cancer (upper inner, lower inner, lower outer, upper outer Lymph drainage- approx 75% drains into axillary lymph nodes then back to the axillary drainage system, lymphadema of upper extremity is potential secondary complication following surgery for breast CA |
|
|
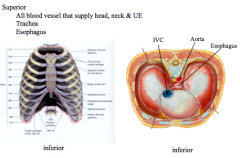
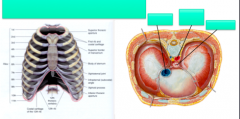
Superior aperture- contains esophagus, trachea, nerves & blood vessels that supply the head, neck and UE
Inferior aperture- allows the esophagus, IVC and aorta to pass inferior |
|

|
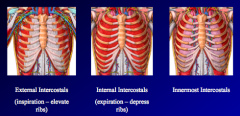
External- inspiration, internal- expiration, innermost- ?elevate, not completely understood
|
|
|
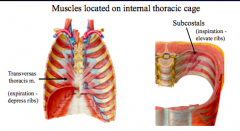
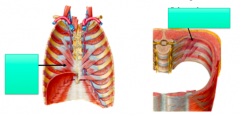
Transversus thoracis- expiration (depresses ribs), located along internal ribs, located on internal anterior thoracic cage
Subcostal Muscles- inspiration (elevate ribs), located on internal portion of the ribs, located on internal posterior thoracic cage |
|
|
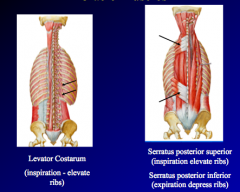
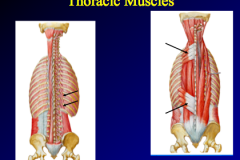
Levator costarum- inspiration (elevate the ribs), attach to ribs and transverse processes of C7-T11, located on external posterior thoracic carriage
Serratus posteiror superior-inspiration (elevates ribs) Serratus posterior inferior- expiration (depresses ribs) |
|
|
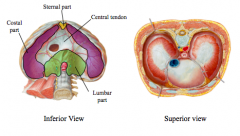
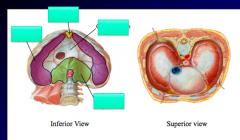
Diaphragm- innervated by phrenic nerve (C3-5) provides motor and sensory components of diaphragm
major muscle of inspiration, contraction will flatten diaphragm- increasing thoracic volume (pressure changes cause increase of air into the lungs) central tendon regions- sternal, costal, lumbar Right is higher than left /c of liver |
|
|
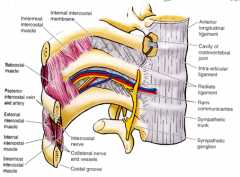
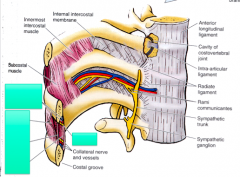
contains 3 layers of muscles (external, internal, innermost)
Neuro bundle (intercostal vein, artery, nerve) Nerve gives off lateral and anterior cutaneous branches Herpes zoster/shingles is common in thoracic region (dominant virus in single segmental nerve will become active, painful, red, vesicular lesion in dermatone pattern, shingles is not limited to thoraic region - will see head/face and LE) |
|
|
Mechanics of breathing
|
Inspiration- rest=diaphragm, exercise= diaphragm + external intercostals, extreme exercise= above + accessory muscles (SCM and scalens) pecs also- pts with COPD can have this type of breathing pattern
Expiration- rest= elastic recoil of lungs, exercise=recruit the internal intercostals + abdominal mm (rectus abdominis, int/ext oblique) |
|
|
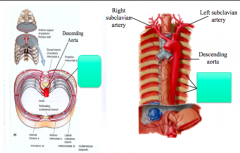
Arterial Blood Supply of Thorax
|
Descending Aorta- provides blood to segmental branches known as posterior intercostal arteries
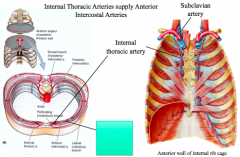
Subclavain Arteries- provide blood to R/L internal thoracic arteries (descend along anterior wall of internal rib cage), anterior intercostal arteries |
|
|
Posterior Intercostal Arteries
travel anteriorly between ribs- along with intercostals vein and intercostals nerve |
|
|
Anterior Intercostal arteries
(originate from internal, travel between ribs and anastomose with posterior intercostal arteries) |
|
|
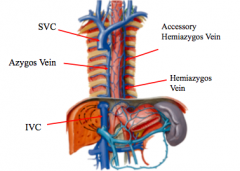
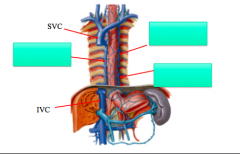
Azygous vein- right posterior internal rib cage, drains into SVC
Hemiazygous and accessory hemizygous veins- located on left posterior internal rib cage, hemiazygous drains, drain segmental portions of thorax |
|
|
Thoracic Cavity and Viscera
|
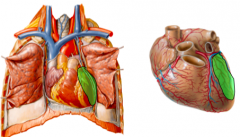
3 compartments- 2 pulmonary cavities (contain lungs and pleura), mediastinum (contains heart, great vessels, trachea, esophagus, thymus and lymph nodes)
|
|
|
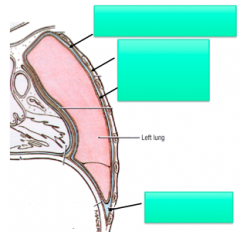
Pleurae
|
each lung is invested by pleural sac
2 layers of continuous, thin, serous membranes- layers are "enfolded" on each other during embryonic development Clinical- pneumothorax- air enters pleural cavity, partial or complete collapse of lung pleural effusion- abnormal accumulation of fluid from pathology within pleural cavity, potential compression of lung Hemothorax- blood accumulates in pleural cavity, potential compression of lung Pleuritis- inflammation of pulmonary pleura, lung sounds "friction rub" |
|
|
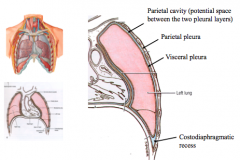
Parietal Cavity- potential space between the two pleural layers, libricated by serous pleural fluid, allows layers to glide smoothly
Parietal Pleura- lines the thoracic wall and diaphragm Visceral pleura- invests the lungs Costodiaphragmatic recess- pleural recesses that can accumulate fluid with various conditions, lateral and posterior removed via thorencentesis (hypodermic needle inserted through intercostal space) |
|
|
Costomediastinal recess- smaller pleural recesses located posterior to sternum
|
|
|
Ventilation
|
mechanical movement of air in/out of lungs, inspiration- increase in volume of thorax creates negative pressure in lungs/pleural cavity causes air to be sucked in
measure by spirometry- static lung volumes (TLC, TV, IRC), dynamic (FEV1, Ve) |
|
|
Respiration
|
gas exchange that occurs in lungs (at alveolar/capillaries) and throughout the body (at target tissue/capillaries)
Pulse Ox- measures arterial oxygen saturation, ideal 96-100% |
|
|
Hilum of Lungs
|
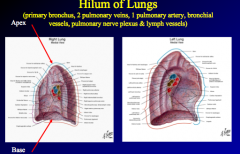
root of each lung (site where the lung becomes covered by visceral pleura), opaque on film
primary bronchus, 2 pulmonary veins (superior and inferior), 1 pulmonary artery (eventually supply pulmonary capillaries for gas exchange), bronchial vessels (supply the lung tissue and pleura), pulmonary nerve plexus (autonomic nerves and sensory nerves), lymph vessels |
|
|
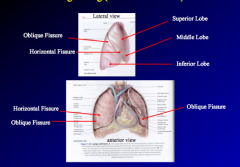
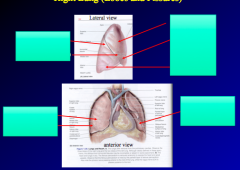
3 lobes separated by oblique fissure and horizontal fissure
superior, middle and inferior lobe right lung eventually divides into 10 bronchopulmonary segments (2- superior, 3- middle, 5- inferior) |
|
|
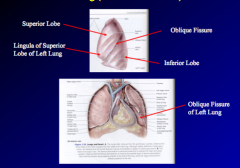
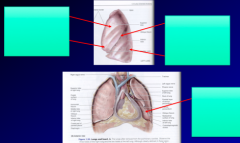
Left lung- 2 lobes separated by oblique fissure, superior and inferior lobes
Lingula- similar to middle lobe of right lung, placement due to heart Left lung eventually divides into 10 bronchopulmonary sgements (5 superior, 5 inferior) |
|
|
Bronchial Tree
|

trachea- bifurcates at carina
R/L primary bronchi (enter the hilum) divide into lobar bronchi (secondary) further divide into segmental bronchi- supply 10 bronchopulmonary segments continue to divide into 20-25 generations of smaller divisions of bronchioles, eventually end as terminal bronchiole (no gas exchange) terminal bronchioles become respiratory bronchioles which supply alveoli (gas exchange) |
|
|
Pulmonary Embolism (PE)
|
obstruction of pulmonary arterial blood flow
embolus may travel from periphery (classically the veins of the legs) back to right side of the heart right side of heart pumps it through the pulmonary trunk to pulmonary artery and gradually into smaller diameter vessels where it will eventually obstruct blood flow obviously a large embolus could be disastrous- acute respiratory distres/failure, potential for death |
|
|
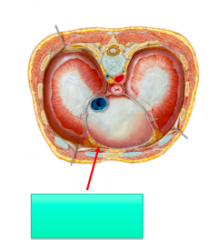
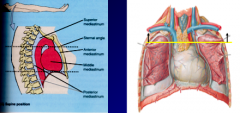
Mediastinum
|
Region between pleural cavities
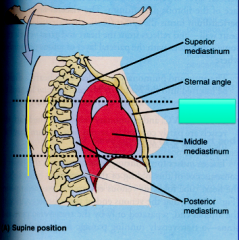
borders- superior (superior thoracic aperture), inferior (diaphragm), anterior (sternum and costal cartilages), posterior (thoracic vertebrae) |
|
|
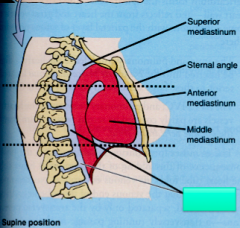
Superior Division of Mediastinum- thymus in children (remnants in adults), arch of aorta, great vessels, trachea, esophagus
|
|
|
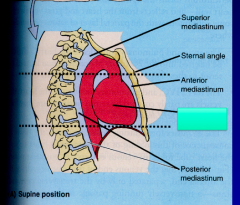
Anterior inferior mediastinum- internal thoracic vessels, fat, few lymph nodes
|
|
|
Middle Inferior Division of mediastinum- pericardium, heart, roots of great vessels
|
|
|
Posterior inferior division- esophagus, descending (thoracic) aorta, thoracic duct, lymph nodes
|
|
|
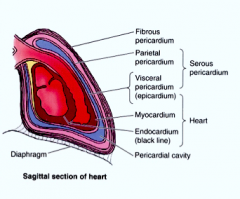
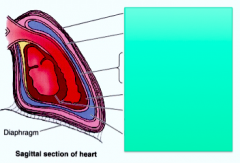
Pericardium- double walled, fibroserous sac
Outside sac- fibrous pericardium attaches to diaphragm via pericardiacophrenic ligament, attaches to sternum via sternopericardial ligament Inside sac- serous pericardium, similar to pleura of lungs, heart invests in on the serous pericardium forming two layers (parietal and visceral- becomes the outer layer of the heart/epicardium), pericardial cavity- potential space between parietal and visceral layers, smooth fluid allows heart to move freely within pericardial sac Heart- epicardium (visceral serous pericardium), myocardium (smooth muscle), endocardium (thin, smooth endothelial layer that lines the heart and valves) |
|
|
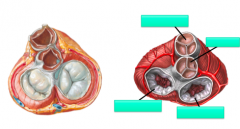
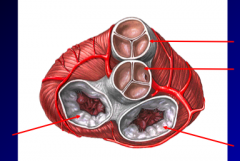
Fibrous Skeleton- four fibrous rings surounding orfices of valves
provides attachments for myocardium of atria and ventricles, provide attachment for cardiac valves, provide electrical insulation between atria and ventricles |
|
|
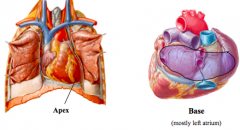
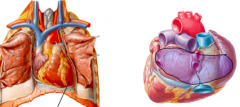
Apex- formed by tipof left ventricle, located between left ribs 5 and 6, just medial to midclavicular line
clincally- might be visible in some patients (apical impulse), sometimes helpful to have pt on left side to visualize/plapate, obesity, pregnancy, excessive muscular development, abnormalities, etc, if location is lateral to midclavicular line, may suggest displacement or cardiac enlargement Base- posterior side of heart as it sits in vivo, formed by the left atrium (technically some right atrium included) |
|
|
Right Border of Heart
|
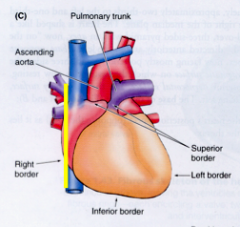
right atrium, extending between SVC and IVC
|
|
|
Left border of heart
|
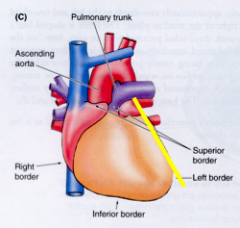
primarily left ventricle and some left atrium
|
|
|
Inferior Border
|
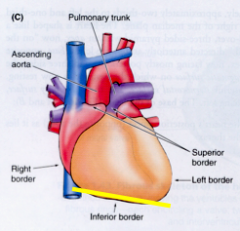
primarily right ventricle and some left ventricle
|
|
|
Superior border
|
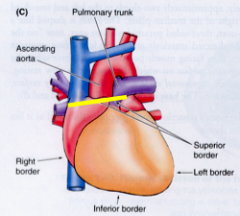
junction where great vessels enter and leave the heart
|
|
|
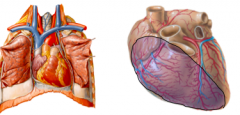
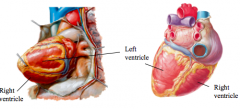
Sternocostal (anterior) surface- mostly right ventrical
clinical- the right ventricle can be examined along the left sternal border (3-5 intercostal spaces) |
|
|
Diaphragmatic/Inferior Surface
mostly left ventricle and partially right ventricle |
|
|
Pulmonary (left) surface- mostly left ventricle
|
|
|
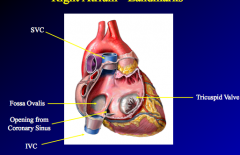
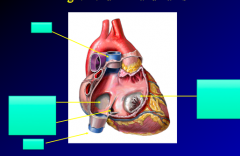
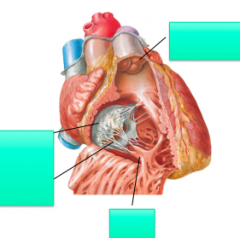
Right Atrium
SVC/IVC openings, opening coronary sinus, fossa ovalis (closed off at birth), tricuspid valve |
|
|
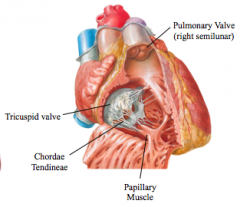
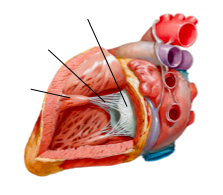
Right Ventricle- tricuspid valve, papillary muscle/chordae tendinae, pulmonary valve
|
|
|
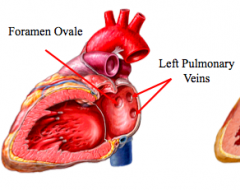
Left Atrium- foramen ovale, 4 opening sof pulmonary veins
|
|
|
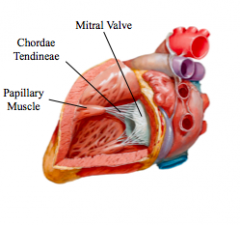
Left ventricle- bicuspid valve, papillary muscle/chordae tendonae, aortic valve
|
|
|
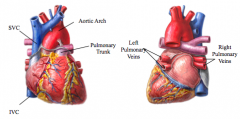
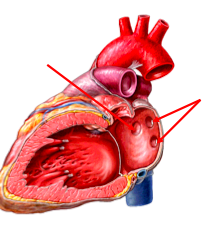
Great Vessels-
SVC- returns blood back to right atrium from areas superior to diaphragm (except from heart and lungs) IVC- returns blood back to the right atrium from areas inferior the diaphragm Pulmonary Trunk- sends oxygenated blood from right ventricle to lungs Right/left pulmonary veins- returns oxygenated blood back to the left atrium from the lungs Aorta- sends blood to body from left ventricle, branches of the aortic arch include - left CCA, L subclavian artery, brachiocephalic trunk (RCCA, R subclavian) |
|
|
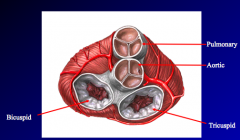
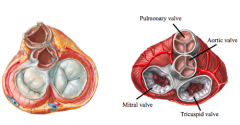
Tricuspid Valve (right AV)- located between right atrium and right ventricle, chordae tendinae and papillary muscles anchor cusps of valve, clinical- auscultate along left sternal border at 5th or 4th intercostal spaces
Pulmonary valve (right semilunar valve)- located between the right ventricle and pulmonary trunk, auscultate along the laft 2nd intercostal spaces Bicuspid valve (left AV valve)- located between left atrium and left ventricle, chordae tendinae and papillary muscles anchor cusps of valve, auscultate along apex (5th intercostal space medial to midclavicular line) Aortic valve (left semilunar)- located between left ventricle and aorta, coronary arteries plug into it, auscultate along right 2nd intercostal space |
|
|
Coronary Arteries
|
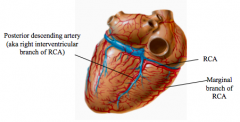
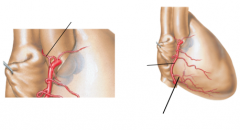
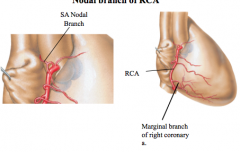
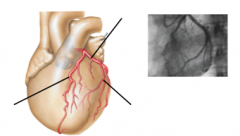
arise from base of aorta- backflow from aortic pressure creates blood flow through coronary arteries
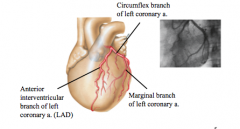
RCA- supplies right atrium and ventricle, nodal branches supply SA and AV nodes, marginal branch of RCA is portion that supplies right ventricle, posterior interventricular artery (right posterior descending) LCA- divides into anterior interventricular artery (LAD) (supplies R/L ventricles and marjority of interventricular septum), circumflex artery (behaves like RCA, supplies atrium and ventricle) marginal branch (supplies left ventricle) |
|
|
|
|
|
|
|
|
|
|
|
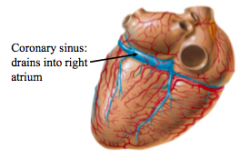
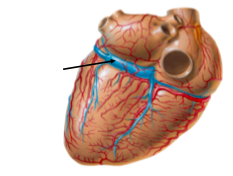
Cardiac Veins- most of the cardiac veins drain into the coronary sinus, coronary drains directly into the right atrium, great, middle, small cardiac veins and oblique vein of the left atrium all empty into coronary sinus, anterior cardiac vein and smallest cardiac veins empty directly into right atrium
|