Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
470 Cards in this Set
- Front
- Back
|
Pt has defective CNS neurons, ependymal cells, oligodendroglia, astrocytes.
Where did these cells derive from? |
Neuroectoderm
|
|
|
Pt has defective Schwann cells, PNS neurons
Where did these cells derive from? |
Neural crest
|
|
|
Pt has defective Microglia, Macrophages
Where did these cells derive from? |
Mesoderm
|
|
|
You see a large cell with prominent nucleoli, Nissl substance (RER) in cell body, dendrites but NO axon. What kind of cell is it?
|
Neuron
|
|
|
This cell provides support, repair, K+ metabolism, removal of excess neurotransmitter, maintains blood-brain barrier
|
Astrocyte
|
|
|
This cell is responsible for reactive gliosis in response to injury
has GFAP |
Astrocyte
|
|
|
This cell is a CNS phagocyte, has small irregular nuclei and little cytoplasm. It is a scavenger cell of the CNS
|
Microglia
|
|
|
This cell differentiates into large phagocytic cells following tissue damage
|
Microglia
|
|
|
This cell fuses to form multinucleated giant cells in the CNS when infected by HIV
|
Microglia
|
|
|
Oligodendrocyte vs. Schwann Cell
|
Oligodendrocyte
- CNS - myelinates multiple axons Schwann cell - PNS - myelinates only 1 axon |
|
|
Pt has multiple sclerosis. What cells are destroyed?
|
Oligodendroglia
|
|
|
Predominant type of glial cell in white matter, looks like fried eggs on H&E
|
Oligodendroglia
|
|
|
Pt has Guillain-Barre syndrome and acoustic neuroma. What embryonal layer do the destroyed cells derive from?
|
Neural crest
Schwann cells |
|
|
Pt can't sense pain and temperature. What type of fiber does the damaged receptor use?
|
C-fiber
- slow, unmyelinated A-delta - fast, myelinated (Free nerve ending) |
|
|
Pt has impaired position sense and dynamic fine touch (manipulation). What type of receptor and nerve fiber is damaged?
where on the body are these found? |
Meissner's corpuscles
- Large, myelinated fibers Glabrous (hairless skin) |
|
|
Pt has impaired vibration, pressure. What type of receptor and nerve fiber is damaged?
where on the body is it found? |
Pacinian corpuscle
- large myelinated fiber deep skin ligaments joints |
|
|
Pt has impaired position sense, static touch (textures). What type of receptor and nerve fiber is damaged?
where on the body is it found? |
Merkel's disks
- large myelinated fibers hair follicles |
|
|
difference in adaptivity b/w Meissners and Merkel cells?
|
Meissner - fast adapting
Merkel - slow adapting |
|
|
Pt w/ Guillain-Barre. What layer of the peripheral nerve is the inflammatory infiltrate in?
|
Endoneurium
|
|
|
What layer of the nerve must be jointed in microsurgery for limb attachment?
|
Perineurium
|
|
|
Pt w/ anxiety. What changes would occur in his NE and 5-HT levels?
|
NE increase
5-HT decrease |
|
|
Pt w/ depression. What changes would occur in his NE and 5-HT levels?
|
NE decrease
5-HT decrease |
|
|
NE changes in
a) anxiety b) depression |
anxiety - NE increase
depression - NE decrease |
|
|
Pt w/ schizophrenia. What neurotransmitter is elevated?
|
dopamine
|
|
|
Pt w/ parkinson's. What neurotransmitter is reduced?
|
dopamine
|
|
|
changes in dopamine in
1) schizophrenia 2) parkinsons |
schizophrenia - elevated
parkinsons - reduced |
|
|
2 situations in which ACh is reduced?
1 in which it is increased |
Alzheimers
Huntingtons REM |
|
|
What is neurotransmitter is reduced in Alzheimers?
|
ACh
|
|
|
Huntington's patient. What 2 neurotransmitter defiencies are responsible for his symptoms?
|
GABA and ACh
|
|
|
What are 2 conditions in which GABA is reduced?
|
anxiety
Huntington's |
|
|
Pt lacks NE. Where is the lesion?
|
locus ceruleus
|
|
|
Pt lacks Dopamine. Where is the lesion?
|
Ventral tegmentum and SNc
|
|
|
Pt lacks 5-HT. Where is the lesion?
|
Raphe nucleus
|
|
|
Pt lacks Ach. Where is the lesion?
|
Basal nucleus of Meynert
|
|
|
Pt lacks GABA. Where is the lesion?
|
Nucleus accumbens
|
|
|
Small part of brain responsible for stress and panic
|
Locus ceruleus
|
|
|
Part of brain responsible for reward, pleasure, addiction, fear (2)
|
Nucleus accumbens and septal nucleus
|
|
|
What 3 structures form the blood-brain barrier?
|
1) Tight junctions
2) Basement membrane 3) Astrocyte processes |
|
|
defective carrier-mediated transport in blood-brain barrier. What 2 substances cannot cross?
|
glucose
amino acids |
|
|
What are 2 specialized brain regions that allow molecules in the blood to affect brain function?
|
area postrema - vomitting after chemo
OVLT - osmotic sensing |
|
|
Pt has vasogenic edema. What vasculature structure was destroyed?
|
infarct destroyed endothelial tight junctions
|
|
|
What are the functions of the Hypothalamus?
|
TAN HATS
Thirst Adenohypophysis control Neurohypophysis control Hunger Autonomic regulation Temperature regulation Sexual urges |
|
|
Inputs to the hypothalamus
|
Area postrema - vomiting signals from emetics
OVLT - senses osmolarity |
|
|
Pt peeing out a lot. What brain structure is damaged?
|
Supraoptic nucleus - makes ADH
|
|
|
Mother is pregnant but has trouble inducing contractions when she goes into labor. What brain structure is defective?
|
Paraventricular nucleus - makes oxytocin
|
|
|
Pt has no appetite. What brain area is damaged?
|
Lateral nucleus of hypothalamus
|
|
|
Pt has craniopharyngioma and can't stop eating. What's wrong?
|
damaged Ventromedial nucleus of hypothalamus - normally elicits satiety
|
|
|
What brain area is responsible for cooling and parasympathetic tone?
|
anterior hypothalamus
A/C = anterior cooling |
|
|
What brain area is responsible for heating and sympathetic tone?
|
posterior hypothalamus
|
|
|
Pt has irregular sleep cycles. What area of brain is damaged?
|
Suprachiasmatic nucleus - regulates circadian rhythm
"You need to sleep to be charismatic!" |
|
|
What 2 hypothalamic nuclei project to the posterior pituitary and what do they release there?
|
Supraoptic - ADH
PVN - oxytocin |
|
|
This part of the brain is responsible for the major relay of ascending sensory information
|
Thalamus
|
|
|
Pt can't sense pain, temperature, proprioception, or position. What part of thalamus is damaged?
|
VPL
|
|
|
pain, temperature, proprioception, or position info in thalamus
input/output |
input: spinothalamic and dorsal columns, medial lemniscus
output: primary somatosensory cortex |
|
|
Pt can't sense facial sensation or taste. What part of thalamus is damaged?
|
VPM
|
|
|
facial sensation and taste in thalamus
input/output? |
input: trigeminal and gustatory pathway
output: Primary somatosensory cortex |
|
|
Pt can't see. What part of thalamus is damaged?
|
LGN
|
|
|
Vision info in thalamus
input/output |
input: CN II
output: Calcarine sulcus |
|
|
Pt can't hear. What part of thalamus is damaged?
|
MGN
|
|
|
Auditory info in thalamus
input/output |
input: superior olive and inferior colliculus of pons
output: Auditory cortex of temporal lobe |
|
|
Thalamus pneumonics
|
Makeup goes on the face (VP-M)
Lateral = light Medial = music |
|
|
Pt has problems feeding, fleeing, fighting, feeling, and sex.
where is the lesion? |
limbic system
famous 5 F's |
|
|
structures in the limbic system (5)
|
cingulate gyrus
hippocampus fornix mammilary bodies septal nucleus |
|
|
receives contralateral cortical input via middle cerebrellar peduncle and ipsilateral proprioceptive information via inferior cerebellar peduncle
|
cerebellum
|
|
|
input nerves to cerebellum
|
climbing and mossy fibers
|
|
|
output nerves from cerebellum
|
Purkinje fibers to deep nuclei of cerebellum -> cortex via superior cerebellar peduncle
|
|
|
What are the deep nuclei of the cerebellum?
|
Dentate, Emboliform, Globose, Fastigial
"Don't Eat Greasy Food" |
|
|
Pt has trouble w/ voluntary movements of extremities.
Where in the cerebellum is the lesion? |
Lateral cerebellum
|
|
|
Pt has trouble w/ balance, truncal coordination, ataxia, tends to fall toward injured side
|
Medial cerebellum
|
|
|
which side of cortex is stimulated by cerebellar outputs?
|
contralateral
|
|
|
which part of brain is important in volutnary movements and postural adjustments?
|
basal ganglia
|
|
|
basal ganglia
input? output? |
input: cortex
output: negative feedback to cortex to modulate movement |
|
|
what 2 structures compose the striatum?
|
putamen (motor) + caudate (cognitive)
|
|
|
what 2 structures compose the lentiform?
|
putamen + globus pallidus
|
|
|
describe the excitatory pathway in the basal ganglia
|
1. SNc's dopamine binds to D1 receptors in the excitatory pathway to stimulate it
- ^ motion |
|
|
describe the inhibitory/indirect pathway in the basal ganglia
|
1. SNc's dopamine binds to D2 receptors
2. inhibit the inhibitory pathway - ^ motion *loss of dopamine in Parkinson's "disinibits" the inhibitor, preventing movement |
|
|
A-synuclein-intracellular inclusion
pathology? |
lewy bodies in parkinsons
|
|
|
depigmentation of substantia nigra pars compacta
disease? |
parkinsons
|
|
|
Tremor
Cog-wheel rigidity Akinesia Postural instability |
parkinsons
"TRAP" |
|
|
sudden wild flailing of 1 arm +/- leg
|
helmiballismus
|
|
|
hemiballismus
what area of the brain is the lesion? side? likely cause? |
contralateral
subthalamic nucleus lacunar stroke from HTN (hypertension) |
|
|
hemiballismus
what is not longer inhibited? |
loss of inhibition of thalamus through globus pallidus
|
|
|
autosomal-dominant (CAG)
trinucleotide repeat disorder neuronal death via NMDA-R binding and glutamate toxicity |
Huntington's disease
|
|
|
chorea
aggression depression dementia what part of brain is atrophied? |
strial nuclei (main inhibitors of movement)
|
|
|
huntington's
what substances are low and where in the brain? |
ACh and GABA are low in the caudate
|
|
|
sudden jerky purposeless movements
where is the lesion? what is this called? |
basal ganglia
(chorea) i.e. Huntington's |
|
|
slow writhing movements of fingers (snakelike)
where is the lesion? what is this called? |
basal ganglia
athetosis |
|
|
pt has jerks, hiccups
condition? |
myoclonus
sudden, brief muscle contractions |
|
|
pt has writers cramp
condition? |
dystonia
sustained, involuntary muscle contractions |
|
|
tremor worsens when holding posture
self-medicates w/ alcohol AD inheritance tx? |
essential/postural tremor
beta-blockers |
|
|
tremor most noticed distally
condition? seen commonly in what disease? |
resting tremor
pin-rolling tremor in parkinsons |
|
|
slow zigzag motion when pointing toward a target
conditon? associated with dysfunction in what part of brain? |
intention tremor
cerebellum |
|
|
defective speech
what area of brain? |
broca's area
|
|
|
defective comprehension
what area of brain? |
associated auditory cortex (Wernicke's area)
|
|
|
Near what part of the brain is Hescl's gyrus located?
|
primary auditory cortex
|
|
|
lower extremity defecit in sensation and movement
what brain vessel is involved? (what is the name of the tool used to answer this) |
anterior cerebral artery
(based on a homonculus) |
|
|
hyperorality
hypersexuality disinhibited behavior where in the brain is the lesion? |
Amygdala (bilateral)
Kluver-Bucy syndrome |
|
|
Disinhibition
deficits in concentration, orientation, and judgement reemergence of primitive reflexes where in the brain is the lesion? |
Frontal lobe
|
|
|
agnosia of the contralateral side of the world
where in the brain is the lesion? |
right parietal lobe
spatial neglect syndrome |
|
|
reduced leved of arousal and wakefullness (i.e. coma)
|
reticular activating system (midbrain)
|
|
|
confusion, opthalmoplegia, ataxia
memory loss, confabulation, personality changes where in the brain is the lesion? |
Mammillary bodies (bilateral)
Wernicke-Korsakoff syndrome |
|
|
tremor at rest, chorea, athetosis
where in the brain is the lesion? |
Basal ganglia
|
|
|
intention tremor
limb ataxia where in the brain is the lesion? what side? |
cerebellum
ipsilateral defects (cerebellum -> SCP -> contralateral cortex -> corticospinal decussation -> ipsilateral) |
|
|
truncal ataxia
dysarthria (poor articulation) where in the brain is the lesion? |
cerebellar vermis
|
|
|
contralateral hemiballismus
where in the brain is the lesion? |
subthalamic nucleus
|
|
|
can't make new memories
where in the brain is the lesion? |
hippocampus
anterograde amnesia |
|
|
eyes look away from side of lesion
where in the brain is the lesion? |
Paramedian Pontine Reticular Formation (PPRF)
|
|
|
eyes look toward lesion
where in the brain is the lesion? |
frontal eye fields
|
|
|
acute paralysis
dysarthria dysphagia diplopia loss of consciousness cause? |
rapid correction of hyponatremia
Central pontine myelinolysis |
|
|
axial T1-weighted MRI
abnormally increased signal in the pons condition? |
central pontine myelinolysis
|
|
|
hoarseness
loss of all laryngeal muscles what structure is injured? what muscle is excluded? |
recurrent laryngeal nerve
cricothyroid |
|
|
higher-order inability to speak vs. motor inability to speak
name of conditions? |
Aphasia vs. Dysarthria
|
|
|
Nonfluent aphasia with intact comprehension
where in the brain is the lesion? |
inferior frontal gyrus (Broca's area)
(Broca's aphasia) |
|
|
fluent aphasia with impaired comprehension
where in the brain is the lesion? |
superior temporal gyrus
Wernicke's aphasia |
|
|
nonfluent asphasia with impaired comprehension
where in the brain is the lesion? |
Both Broca's and Wernickes area
Global aphasia |
|
|
Poor repetition but fluent speech, intact comprehension
where in the brain is the lesion? |
arcuate fasciculus - connects Brocas and Wernicke's area
Conduction aphasia |
|
|
can't repeat phrases such as "No ifs, ands, or buts"
|
conduction aphasia
|
|
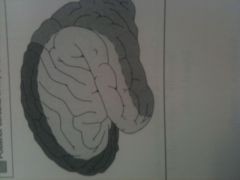
What vessel supplies each area?
|
black - anterior cerebral artery (anteromedial surface)
middle - middle cerebral artery (lateral surface) grey - posterior cerebral artery (posterior and inferior) |
|
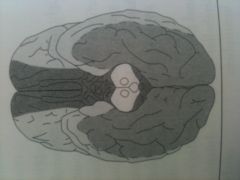
What vessel supplies each region?
|
black - anterior cerebral
white - middle cerebreal gray - posterior cerebral |
|
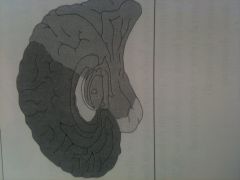
what vessel supplies each region?
|
black - anterior cerebral
white - middle cerebreal gray - posterior cerebral |
|
|
contralateral hemiparesis of lower extremities
decreased contralateral proprioception ipsilateral paralysis of hypoglossal nerve what vessel is compromised? |
anterior spinal artery
(medial medullary syndrome) |
|
|
contralateral loss of pain and temp
ipsilateral dysphagia, hoarseness decreased gag reflex vertigo, diplopia, nystagmus, vomitting ipsilateral horner's, facial pain and temp, ataxia what vessel is compromised? |
PICA
(lateral medullary syndrome aka Wallenbergs) |
|
|
ipsilateral facial paralysis, cochlear nucleus, nystagmus, facial pain and temp, dystaxia (MCP, ICP)
what vessel is compromised? |
AICA
(lateral inferior pontine syndrome) |
|
|
contralateral hemaniopia with macular sparing
what vessel is compromised? |
posterior cerebral artery
supplies occiptal cortex |
|
|
contralateral face and arm paralysis and sensory loss, aphasia (dominant sphere), left-sided neglect
what vessel is compromised? |
middle cerebral artery
|
|
|
loss of motor and sensory in left foot
what vessel is compromised? |
anterior cerebral artery
|
|
|
most common site of circle of Willis aneurysm
visual field defects |
anterior communicating artery
|
|
|
common area of aneurysm, causes CN III palsy
|
posterior communicating artery
|
|
|
supply internal capsule, caudate, putamen, globus pallidus
"arteries of stroke" what region is defective? |
lateral striate
|
|
|
pure motor hemiparesis
what brain region is infarcted? |
posterior limb of the internal capsule
|
|
|
upper leg/arm weakness
defect in higher-order visual processing severe hypertension what region is damaged? |
watershed zones
|
|
|
"locked-in syndrome"
CN III still intact what vessel is infarcted? |
basilar artery
|
|
|
general sensory and motor dysfunction, aphasia
what vessel region is defective? |
stroke of anterior circle
|
|
|
cranial nerve defecits (vertigo, visual defects)
coma cerebellar deficits (ataxia in dominant hemisphere), neglect in nondominant what vessel area is defective? |
stroke of posterior circles
|
|
|
where do berry aneurysms occur?
what happens? |
bifurcations in the circle of Willis, most common the anterior communicating artery
hemorrhagic stroke/subarachnoid hemorrhage |
|
|
Adult polycystic kidney disease
Ehler-Danos syndrome Marfans syndrome associated with what? |
Berry aneurysms
|
|
|
What complication is HTN associated with in the brain?
what regions? |
Charcot-Bouchard microaneurysms (small vessels)
basal ganglia, thalamus |
|
|
lucid interval, rapid expansion under systemic arterial pressure
what bone is fractured? what vessel is ruptured? what type of herniation? what nerve palsy? |
- temporal bone
- middle meningial artery (branch of maxillary) - transtentorial herniation, CN III palsy epidural hematoma |
|
|
CT shows biconvex disk
doesn't cross suture lines can cross falx, tentorium condition? |
epidural hematoma
|
|
|
delayed onset of symptoms
elderly, alcoholics, blunt trauma, shaken babies predisposing factors? what structures are damaged? |
brain atrophy, shaking
bridging veins -> slow venous bleeding less pressure = gradual hematoma subdural hematoma |
|
|
"worst headache of my life"
bloody or yellow spinal tap cause? risk of what 2-3 days later? treat with what? |
- rupture of an aneurysm (often Berry) or an AVM
- risk of vasospasm due to blood breakdown products 2-3 days later - treat with Calcium Channel Blockers (Subarachnoid hemorrhage) |
|
|
hypertension
amyloid angiopathy lobar strokes all over brain diabetes mellitus condition? where in brina? |
parenchymal hematoma
basal ganglia and internal capsule |
|
|
how long does it take for ischemic brain disease to cause irreversible damage?
|
5 minutes
|
|
|
what regions of the brain are most vulnerable to ischemic brain injury?
|
hippocampus
neocortex cerebellum watershed areas |
|
|
its 12-48 hrs after ischemic brain injury
what do you see histologically? |
red neurons
|
|
|
its 24-72 hrs after ischemic brain injury
what do you see histologically? |
necrosis + neutrophils
|
|
|
its 3-5 days after ischemic brain injury
what do you see histologically? |
macrophages
|
|
|
its 1-2 weeks after ischemic brain injury
what do you see histologically? |
reactive gliosis + vascular proliferation
|
|
|
its >2 weeks after ischemic brain injury
what do you see histologically? |
glial scar
|
|
|
thrombi led to ischemic stroke with subsequent necrosis
formed cystic cavity with reactive gliosis cause? |
atherosclerosis
|
|
|
intracerebral bleeding, due to aneurysm rupture
secondary to ischemic stroke followed by reperfusion (^ vessel fragility) name of event? |
hemorrhage
|
|
|
cause of ischemic stroke for 1) large vessels 2) small vessles
treatment? |
Large vessels (emboli)
- atrial fib - carotid dissection - patent foramen ovale - endocarditis small vessels - lacunar strokes secondary to HTN tx: tPA w/in 3 hrs |
|
|
brief reversible episode of neurologic dysfunction due to focal ischemia
symptoms last for under 24 hrs |
TIA (Transient Ischemic Attack)
|
|
|
bright on diffusion weighted-MRI in 3-30 min and remains bright for 10 days
dark on non-contrast CT in 24 hrs condition? |
stroke
|
|
|
bright areas on noncontrast CT
tx? |
hemorrhage
tx: tPA |
|
|
where do the venous sinuses run?
what is there order? |
in the dura mater (where its meningeal and periosteal layers separate)
cerebral veins -> venous sinuses -> internal jugular vein |
|
|
what are the branches eminating from the confluence of sinuses? what other branches do they form?
|
superior saggital sinus
straight sinus (becomes inferior saggital sinus and great cerebral vein of Galen) transverse sinus -> sigmoid sinus -> internal jugular vein |
|
|
what structure makes CSF?
what reabsorbs it? |
choroid plexus
venous sinus arachnoid granulations |
|
|
where does the lateral ventricle empty into? via what opening?
3rd ventricle " " " 4th ventricle |
3rd ventricle via foramen of Monro
4th ventricle via cerebral aqueduct subarachnoid space via: 1) Foramina of Luschka (Lateral) 2) Foramen of Magendie (Medial) |
|
|
wet, wobbly and wacky
|
normal pressure hydrocephalus
|
|
|
does not result in increase in subarachnoid space volume
clinical triad of dementia, ataxia, and urinary incontinence (reversible cause of dementia in the elderly) condition? |
normal pressure hydrocephalus
expansion of ventricle distorts the fibers of the corona radiata |
|
|
what causes the ^ intracranial pressure, papilledema, and hernitation (arachnoid scarring post-meningitis) in communicating hydrocephalus?
|
decreased CSF absorption by arachnoid villi
|
|
|
what is the problem in Obstructive (noncommunicating) hydrocephalus?
|
structural blockage of CSF circulation within the ventricular system (stenosis of the aqueduct of Sylvius)
|
|
|
^ CSF in atrophy of brain, normal intracranial pressure
what diseases have this? |
hydrocephalus ex vacuo
AIDS Pick's disease |
|
|
how many spinal nerves are there?
cervical nerves? thoracic? lumbar? sacral? coccygeal? |
31 spinal total
8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal |
|
|
which groups of nerves exits via intervertebral foramina ABOVE the corresponding vertebrate while others exit below?
|
nerves C1-C7
|
|
|
patient has a herniated vertebral disk
mechanism? where most common? |
nucleus pulposus herniates through annulus fibrosus (b/w L5 and S1)
|
|
|
what vertebrate marks the end of the spinal cord?
subarachnoid space? where is lumbar puncture performed? |
spinal cord: L1-2
subarachnoid space: S2 lumbar puncture: L3--5 interspaces at the level of the cauda equina |
|
|
patient can't sense pressure, vibration, touch, prioprioception
whats spinal cord tracts are compressed |
dorsal columns
|
|
|
pt lost voluntary motor control
whats spinal cord tracts are compressed |
lateral corticospinal tract
|
|
|
pt can't feel temperature or pain
|
spinothalamic tract
|
|
|
where is control of the legs in the spinal cord?
|
Legs are Lateral in Lateral corticospinal, spinothalamic tracts
|
|
|
Dorsal column - medial lemniscal pathway
senses? 1st order neuron? synapse 1? second order neuron? synapse 2? 3rd order neuron? |
pressure, vibration, touch, proprioception
1st order - sensory nerve ending -> cell body in dorsal root ganglion -> spinal cord Synpase 1 - ipsilateral nucleus cuneatus or gracilis (medulla) 2nd order - decussates in medulla -> contralateral in medial lemniscus Synapse 3 - VPL of thalamus 3rd order - sensory cortex |
|
|
Spinothalamic tract
senses? 1st order neuron? synapse 1? second order neuron? synapse 2? 3rd order neuron? |
pain and temperature
1st order - sensory nerve endings (A-d, C fibers) -> cell body in dorsal root ganglion -> spinal cord Synapse 1 - ipsilateral gray matter 2nd order neuron - decussates at anterior white commissure -> ascends contralaterally Synapse 2 - VPL of thalamus 3rd order neuron - sensory cortex |
|
|
Lateral corticospinal tract
senses? 1st order neuron? synapse 1? second order neuron? synapse 2? 3rd order neuron? |
descending voluntary movements of contralateral limbs
1st order - upper motor neuron in cortex -> descends ipsilateral (through internal capsule) -> decussates at caudal medulla (pyramidal decussation) -> descends contralateral Synapse 1 - cell body of anterior horn 2nd order - lower motor neuron -> leaves spinal cord Synapse 2 - neuromuscular junction |
|
|
Motor neuron signs
weakness |
UMN
LMN |
|
|
Motor neuron signs
Atrophy |
LMN
|
|
|
Motor neuron signs
Fasciculation |
LMN
|
|
|
Motor neuron signs
Reflexes |
^ in UMN
reduced in LMN |
|
|
Motor neuron signs
Tone |
^ in UMN
reduced in LMN |
|
|
Motor neuron signs
Babinski sign UMN or LMN? |
UMN
|
|
|
Spastic paralysis
|
UMN
|
|
|
Clasp knife spasticity
UMN or LMN? |
UMN
|
|
|
Motor neuron signs
everything lowered (less muscle mass, tone, reflexes, downgoing toes) |
LMN
|
|
|
Motor neuron signs
everything up (tone, DTR, toes) |
UMN
|
|
|
poliomyelitis and Werdnig-Hoffman disease
where is the lesion? |
LMN
|
|
|
scanning speech, intention, tremor, nystagmus
where is the lesion? |
white matter of cervical region from demyelination
|
|
|
ALS
|
combined UMN and LMN deficits
NO SENSORY DEFICIT (pure motor disease) |
|
|
anterior spinal artery is occluded
what parts of spina cord are spared |
dorsal columns
tract of Lissauer |
|
|
what part of spinal cord is degenerated in tertiary syphillis
effects? |
dorsal roots and columns
- impaired proprioception and locomotor ataxia tabes dorsalis |
|
|
bilateral loss of pain and temperature sensation
seen in what diseases? |
damage of white commissure of spinothalamic tract (2nd order neuron)
(C8-T1) chiari type 1 and 2 (Syringomyelia) |
|
|
ataxic gait
hyperreflexia impaired position and vibration sense |
Vitamine B12 neuropathy
Vitamine E deficiency Friedreich's ataxia |
|
|
polio virus
life cycle |
fecal-oral
replicates in oropharynx and small intestine -> bloodstream -> CNS (spinal cord) -> destruction of anterior horn -> LMN destruction |
|
|
malaise
headache fever nausea abdominal pain sore throat + LMN signs what would you see in CSF? where is virus recovered from? |
lymphocytic pleocytosis
elevated protein normal glucose virus recovered from stool or throat poliomyelitis |
|
|
floppy baby
tongue fasciculations median age of death 7 months associated with what? |
associated with degeneration of anterior horns (LMN involvement only)
Werdnig-Hoffman disease (aka infantile spinal muscular atrophy) |
|
|
Associated with BOTH UMN and LMN signs
no sensory, cognitive, or oculomotor deficits |
AML
|
|
|
can be caused by a defect in superoxide dismutase 1 (SOD1)
fasciculations and eventual atrophy progressive and fatal tx and mechanisms? |
Riluzole lengths survival by decreasing presynaptic glutamate release
AML |
|
|
impaired proprioception and locomotor ataxia
Charcot's joints shooting (lightening) pain dx/mechanism? |
Tabes dorsalis
degeneration of dorsal columns and dorsal roots due to teritary syphillis |
|
|
pupils reactive to accomodation but not to light
absence of DTRs positive Romberg sensory ataxia at night |
Tabes dorsalis
"Argyll Robertson pupils" |
|
|
child with kyphoscoliosis and:
staggering gait frequent falling nystagmus dysarthria pes cavus hammer toes hypertrophic cardiomyopathy dx/mechanism? |
Freidreich's ataxia
AR trinucleotide repeat disorder (GAA) in the frataxin gene --> impaired mitochondrial functioning "Freidreich is your favorte FRAT brother, always staggering and falling" |
|
|
1. ipsilateral UMN signs below lesion
2. ipsilateral loss of tactile, vibration, proprioception below lesion 3. contralateral pain and temp loss below lesion 4. ipsilateral loss of all sensation at level of lesion 5. LMN signs (flaccid paralysis) at level of lesion |
Brown-Sequard syndrome
|
|
|
presents with Horner's syndrome if lesion occurs above T1
|
Brown-Sequard syndrome
|
|
|
Ptosis
Anhidrosis Miosis dx/mech? |
Horner's syndrome
lesion of spinal cord above T1 (i.e. Pancoast, Brown-Sequard, late stage syringomyelia) PAM is HORNY |
|
|
describe the path of the 3-neuron oculosympathetic pathway
|
hypothalamus --> interomedial column of spinal cord --> superior cervical (sympathetic ganglion) --> pupil --> smooth muscle of eyelids --> sweat glands of forehead and face
|
|
|
landmark dermatomes
posterior half of a skull "cap" |
C2
|
|
|
landmark dermatomes
high turtleneck shirt |
C3
|
|
|
landmark dermatomes
low-collar shirt |
C4
|
|
|
landmark dermatomes
at the nipple |
T4
|
|
|
landmark dermatomes
at the xiphoid process |
T7
|
|
|
landmark dermatomes
at the umbilicus |
T10
|
|
|
landmark dermatomes
at the inguinal ligament |
L1
|
|
|
landmark dermatomes
includes the kneecaps |
L4
|
|
|
landmark dermatomes
erection and sensation of penile and anal zones |
S2,3,4
|
|
|
where is pain in the diaphragm and gallbladder referred to?
|
right shoulder via the phrenic nerve
|
|
|
clinical reflexes
biceps |
C5
|
|
|
clinical reflexes
triceps |
C7
|
|
|
clinical reflexes
patella |
L4
|
|
|
clinical reflexes
achilles mediated by which spinal nerve? |
S1
|
|
|
Babinski in 3 yo
cause? |
UMN lesion
|
|
|
primitive reflexes
extend limbs when startled and then draw back together |
Moro reflex
|
|
|
primitive reflexes
movement of the head toward one side if cheek or mouth is stroked (nipple seeking) |
Rooting reflex
|
|
|
primitive reflexes
sucking response when roof of mouth is touched |
Sucking reflex
|
|
|
primitive reflexes
curling of fingers/toes if palms of hands/feet are stroked |
Palmar and plantar reflexes
|
|
|
primitive reflexes
dorsiflexion of large toe and fanning of other toes with plantar stimulation |
Babinski reflex
|
|
|
reduced melatonin secretion and circadian rhythm
what structure is defective? |
pineal gland
|
|
|
where is the vertical gaze center?
what is the name of the condition where you have a lesion here? |
superior colliculi
Parinaud syndrome (i.e. from pinealoma) |
|
|
where is the auditory center in the brain
|
inferior colliculi
eyes are above ears, superior is above inferior colliculus |
|
|
pnemumonic for cranial nerves
|
Some Say Marry Money But My Brother Says Big Brains Matter Most
(CN I-XII) S= sensory M = motor B = both |
|
|
pt can't move SR, IR, MR, IO
can't constrict pupil can't accomodate can't open eyelid what CN is defective? |
CN III
|
|
|
pt can't move SO eye muscle
what CN is defective? |
CN IV (trochlear)
- motor |
|
|
pt can't chew
can't feel face what CN is defective? |
CN V (trigeminal)
- both |
|
|
pt can't move LR
what CN is defective? |
CN VI (abducens)
- motor |
|
|
pt can't move face
can't taste from anterior 2/3 of tongue can't lacrimate or salivate can't close eyelids trouble hearing what CN is defective? |
CN VIII (facial)
- both |
|
|
pt has trouble hearing and maintaining balance
what CN is defective? |
CN VIII (vestibulocochlear)
- sensory |
|
|
pt has no taste from posterior 1/3 of tongue
can't swallow or salivate defective carotid and baroreceptors and chemoreceptors can't elevate pharynx and larynx what CN is defective? |
CN IX (glossopharyngeal)
- both |
|
|
can't taste from epiglottic region
can't swallow or elevate palate uvula deviated from midline can't talk or cough innervates thoracoabdominal viscera monitors aortic arch chemo- and baroreceptors what CN is defective? |
CN X (vagus)
- both |
|
|
pt can't turn head or shrug shoulders
what CN is defective? |
CN XI (accessory)
- motor |
|
|
pt can't move tongue
what CN is defective? |
CN XII (hypoglossal)
- motor |
|
|
midbrain is wiped out
which CN nuclei are affected? |
CN III, IV
|
|
|
pons is wiped out
which CN nuclei are affected? |
CN V, VI, VII, VIII
|
|
|
medulla is wiped out
which CN nuclei are affected? |
CN IX, X, XI, XII
|
|
|
function different b/w lateral vs. medial nuclei in tegmentum
|
lateral = sensory (alar plate)
medial = motor (basal plate) |
|
|
what CN control the afferent/efferent paths of the following reflex:
corneal |
Afferent - V1(opthalmic - nasociliary branch controls levator palpebrae)
Efferent - VII (temporal branch controls orbicularis oculi) |
|
|
what CN control the afferent/efferent paths of the following reflex:
lacrimation |
Afferent - V1 (loss of reflex does not preclude emotional tears)
Efferent - VII |
|
|
what CN control the afferent/efferent paths of the following reflex:
jaw jerk |
Afferent - V3 (sensory - muscle spindle from masseter)
Efferent - V3 (motor - masseter) |
|
|
what CN control the afferent/efferent paths of the following reflex:
pupillary |
Afferent - II
Efferent - III |
|
|
what CN control the afferent/efferent paths of the following reflex:
gag |
Afferent - IX
Efferent - IX, X |
|
|
defect in taste, baroreceotors, gut distension info (visceral sensory info)
which vagal nuclei is affected? |
nucleus solitarius
|
|
|
defect in motor innervation of pharynx, larynx, and upper esophagus (swallowing, palate elevation)
which vagal nuclei is affected? |
nucleus ambiguus
|
|
|
defect in sending autonomic (parasynpathetic) fibers to hear, lungs, and upper GI
which vagal nuclei is affected? |
Dorsal motor nucleus
|
|
|
what CN's passes through the middle cranial fossa?
|
CN II-IV
|
|
|
what CN passes through the optic channel?
|
CN II
|
|
|
what CN's and vessels pass through the superior orbital fissure?
|
CN III, IV, V1, opthalmic vein, sympathetic fibers
|
|
|
what CN's passes through the foramen rotundum?
|
CN V2
|
|
|
what CN's passes through the foramen ovale?
|
CN V3
|
|
|
what vessel passes through the foramen spinosum?
|
middle meningeal artery
|
|
|
what CN's passes through the posterior cranial fossa (temporal or occipital bone)?
|
CN VII-XII
|
|
|
what CN's passes through the internal auditory meatus?
|
CN VII, VIII
|
|
|
what CN's and vessels pass through the jugular foramen?
|
CN IX, X, XI, jugular vein
|
|
|
what CN's passes through the hypoglossal canal?
|
CN XII
|
|
|
what CN's and vessels pass through the foramen magnum?
|
spinal roots of CN XI, brain stem, vertebral arteries
|
|
|
a collection of venous sinuses on either side of the pituitary
input/output for blood through this structure? |
cavernous sinus
blood from eye and sueprficial cortex --> cavernous sinus --> internal jugular vein |
|
|
what vessels pass through the cavernous sinus?
|
The nerves that control extraocular muscles (+V1,2)
CN III, IV, V1, V2m and VI postganglionic sympathetic fibers internal carotid all en route to the orbit |
|
|
opthalmoplegia
opthalmic and maxillary sensory loss mechanism? |
cavernous sinus syndrome from mass effect
|
|
|
tongue deviates TOWARD side of lesion (lick your wounds)
cause? |
CN XII lesion (LMN)
- decussates before medulla and synapse on contralateral hypoglossal nucleus |
|
|
jaw deviates TOWARD side of lesion,
|
CN V lesion
bilateral cortical input to lateral pterygoid muscle |
|
|
uvula deviates AWAY from side of lesion, weak side collapses and uvula points away
cause? |
CN X lesion
|
|
|
weakness turning head to contralateral side of lesion (SCM)
shoulder droop on same side as lesion (trapezius) cause? |
CN XI lesion
|
|
|
Contralateral paralysis of lower face only
type of lesion? |
UMN
lesion of motor cortex or connection b/w cortex and facial muscles - upper face receives bilateral UMN innervation |
|
|
ipsilateral paralysis of upper and lower face
type of lesion? |
LMN
|
|
|
Peripheral ipsilateral facial paralysis with inability to close eye on involved side
type of lesion? prognosis? complication of which diseases? |
Bell's palsy
complete destruction of the facial nucleus itself or its branchial efferent fibers - gradual recovery in most cases - AIDS, Lyme disease, Herpes simplex, Sarcoidosis, Tumors, Diabetes (ALexander graHam Bell with STD) |
|
|
can't say kuh-kuh-kuh
defect in which CN? |
CN X (vagus)
- elevates palate |
|
|
can't say la-la-la
defect in which CN? |
CN XII - hypoglossal
|
|
|
can't say mi-mi-mi
defect in which CN? |
CN VII - facial
|
|
|
pt can't close jaw
defect in which 3 muscles? |
Masseter
teMporalis Medial pterygoid "M's Munch" |
|
|
pt can't open jaw
defect in which muscle? |
lateral pterygoid
"Lateral Lowers" |
|
|
pt can't open OR close jaw
which NERVE is damaged? |
V3 (trigeminal nerve)
|
|
|
retinal necrosis + edema --> atrophic scar
condition? |
retinitis
|
|
|
systemic inflammation (i.e. Reiters)
condition? |
Iritis
|
|
|
ciliary muscle contracts (zonular fibers relax --> lens relaxes --> more convex)
condition? |
near vision
|
|
|
ciliary muscle relaxes (lens flattens)
condition? |
distant vision
|
|
|
sclerosis and decrease in elasticity cause lens shape to change
condition? |
aging
|
|
|
acute, painless monocular loss of vision; pale retina and cherry-red macula (has its own blood supply - choroid artery)
|
retinal artery occlusion
|
|
|
what structure absorbs aqueous humor?
|
trabecular meshwork
|
|
|
what structure collects aqueous humor from the trabecular network?
|
Canal of Schlemm
|
|
|
what structure produces aqueous humor?
what receptors are on it? |
Ciliary process
B-adrenergic |
|
|
what structure is responsible for accomodation?
what receptors are on it? |
Ciliary muscle
M3 |
|
|
what structure is responsible for mydriasis?
what receptor is on it? |
radial/dilator muscle
a1 |
|
|
what structure is responsible for miosis?
what receptor is on it? |
Sphincter/circular/constrictor muscle
M3 |
|
|
where are the muscles responsible for mydriasis and miosis located?
|
iris
|
|
|
mechanism of glaucoma?
what would you see? |
impaired flow of aqueous humor --> ^ intraocular pressure --> ocular disk atrophy with cupping
|
|
|
difference b/w open(wide angle) and closed (narrow angle) glaucoma?
How does each manifest clinically? what conditions are each associated with? |
open(wide angle) - obstructed outflow (e.g. canal of Schlemm)
- associated with myopia, old age, African-American - silent, painless (more common) closed(narrow angle) - obstruction of flow between iris and lens --> pressure buildup behind iris - very painful, decrease in vision, rock-hard eye, frontal headache (opthalmologic emergency!) |
|
|
what should you NOT give to treat someone with closed/narrow angle glaucoma?
|
epinephrine
|
|
|
painless, bilateral opacification of lens --> decrease in vision
what are some risk factors for this condition? |
cataract
age, smoking, EtOH, diabetes (sorbitol), trauma, infection random causes: sunlight, classic galactosemia, galactokinase deficiency, |
|
|
^ in intracranial pressure --> elevated optic disk with blurred margins, bigger blind spot (can be seen in hydrocephalus)
dx? |
papilledema
|
|
|
eye looks down and out
ptosis pupillary dilation loss of acommodation where is the damage? |
CN III
|
|
|
- problems reading newspaper or going down stairs
- eye drifts upward causing vertical diplopia where is the damage? |
CN IV
|
|
|
medially directed eye all the time
where is the damage? |
CN VI
|
|
|
what are the mechanical functions of the superior oblique muscle in the eye?
|
abduct
intort depress while adducted |
|
|
which direction should you have the patient look if you want to test their inferior oblique?
|
Up
|
|
|
patient cannot constrict their pupil (miosis)
from what nucleus did the defective nerve originate? |
Edinger-Westphal nucleus --> CN III --> ciliary ganglion
|
|
|
patient cannot dilate their pupil (mydriasis)
from what nucleus did the defective nerve originate? |
T1 preganglionic sympathetic --> superior cervical ganglion --> postganglion sympathetic --> long ciliary nerve
|
|
|
which brain structures are involved in the pupillary light reflex?
|
CN II --> pretectal nucleus (midbrain) --> activate bilateral Edinger-Westphal nucleus --> pupils contract bilaterally (consensual reflex)
*normal: illumination of 1 eye results in bilateral pupillary constriction |
|
|
decreased in bilateral pupillary constrictions when light is shone in affected eye
condition? mechanism? |
Marcus Gunn pupil
afferent pupillary defect (i.e. due to optical nerve damage or retinal detachment) |
|
|
ocular muscles are not working
which part of CN III is affected? possible causes? |
central
vascular disease (diabetes: glucose --> sorbitol) due to increase in diffusion to interior |
|
|
blown pupil
which part of CN III is affected? possible causes? |
peripheral - is responsible for parasympathetic output
- 1st to be affected by compression (i.e. PCA berry aneurysm, uncal herniation) * check with pupillary light reflex |
|
|
separation of neurosensory later of retina from pigment epithelium --> degeneration of photoreceptors --> vision loss. May be secondary to trauma, diabetes
condition? |
retinal detachment
|
|
|
degeneration of macula (central area of retina)
loss of central vision (scotomas) condition? difference b/w 2 types? |
Age-related macular degeneration (ARMD)
Dry/atrophic ARMD - slow, due to fat deposites --> causes gradual decrease in vision Wet - rapid, due to neovascularization |
|
|
pt can't see out of right eye
condition? |
right anopia
|
|
|
patient can't see on lateral half of each eye
condition? |
bitemporal hemianopia
|
|
|
patient can't see on left side of each eye
condition? |
left homonymous hemianopia
|
|
|
pt can't see on upper left corner of each eye
condition and cause? |
left upper quadrantic anopia
right temporal lobe lesion, MCA |
|
|
pt can't see on lower left corner of each eye
condition and cause? |
left lower quadrantic anopia
right parietall lobe lesion, MCA |
|
|
pt can't see on left side or center in both eyes
condition and cause? |
left hemianopia with macular sparing (PCA) --> macula --> bilateral projection to occiput
|
|
|
pt can't see out of left eye at all
condition? |
central scotoma (macular degeneration)
|
|
|
what happens to an image when it hits the primary visual cortex?
|
becomes upside down and left-right reversed
|
|
|
What is Meyer's loop?
|
inferior retina, loops around inferior horn of lateral ventricle
|
|
|
What is the Dorsal optic radiation?
|
superior retina, takes shortest path via internal capsule
|
|
|
nystagmus in abducting eye
convergence is normal pt has multiple sclerosis condition? mechanism? |
internuclear opthalmoplegia (MLF syndrome)
lesion in the MLF --> medial rectus palsy on attempted lateral gaze (aka patient's eye can't look to the other side) |
|
|
decrease in cognitive ability, memory, or function with intact consciousness
condition? |
dementia
|
|
|
most common cause of dementia in elderly
what type of pts have a higher risk of developing this condition? |
Alzheimer's disease
Down syndrome patients |
|
|
What are the familial forms of Alzheimers?
what genes are they associated with? |
Early onset: APP (21), presenilin-1 (14), presenilin-2(1)
Late onset: ApoE4 (19) - ApoE4 is protective |
|
|
widespread cortical atrophy
decrease in Ach Senile plaques condition? |
Alzheimer's disease
|
|
|
complication of senile plaques?
|
(extracellular B-amyloid core): may cause amyloid angiopathy --> intracranial hemorrhage
|
|
|
intracellular, abnormally phosphorylated tau protein
what are they and what do they correlate with? |
neurofibrillary tangles (insoluble cytoskeletal elements)
correlate with degree of dementia |
|
|
dementia
aphasia parkinsonian aspects change in personality condition? what parts of brain are spared? |
Pick's disease
spares parietal lobe and posterior 2/3 of superior temporal gyrus |
|
|
you see intracellular, aggregated tau protein and frontotemporal atrophy
condition? |
Pick's disease (Pick bodies)
|
|
|
Parkinsonism with dementia and hallucinations
what is the defect in microscopically? |
a-synuclein
Lewy body dementia |
|
|
rapidly progressive (weeks to months) dementia with myoclonus
what would you see histologically? what is the pathogen? name of condition? |
histo: spongiform cortex
pathogen: prions (a-helix --> B sheet[resistant to proteases]) Creutzfeldt-Jakob disease (CJD) |
|
|
what is the second most common cause of demential in elderly?
|
multi-infarct
|
|
|
syphilis
HIV vitamin B12 deficiency Wilson disease can all cause what? |
dementia
|
|
|
optic neuritis (sudden loss of vision)
MLF syndrome (intranuclear opthalmoplegia) hemiparesis hemisensory symptoms bladder/bowel incontinence condition? gold standard for diagnosis? |
multiple sclerosis
MRI - oligoclonal bands are also diagnostic |
|
|
30 yo female
periventricular plaques (areas of oligodendrocyte loss and reactive gliosis) w/ preservation of axons sudden loss of vision tx? |
B-interferon
or immunosuppressant therapy + symptomatic treatment for neurogenic bladder, spasticity, pain multiple sclerosis |
|
|
symmetric ascending muscle weakness beginning in distal lower extremities
facial paralysis condition? affects which part of spinal cord? mechanism? |
Guillain-Barre syndrome
inflammation and demyelination of peripheral nerves and motor fibers of ventral roots (sensory effect less severe than motor) |
|
|
cardiac irregularities
HTN or hyPOtension complications of what neurological disease that also has symmetric ascending muscle weakness beginning distally? |
autonomic complications of Guillain-Barre syndrome
|
|
|
^ CSF protein w/ normal cell count
papilledema symmetric ascending muscle weakness starting distally condition? |
Guillain-Barre syndrome
|
|
|
what external pathogens can prompt Guillain-Barre syndrome?
tx? (3) |
inoculations, stress, infections like Campylobacter jejuni or herpesvirus --> molecular mimicry --> autoimmune attack on peripheral myelin
1. respiratory support is critical until recovery (weak diaphragm) 2. plasmapheresis 3. IV immune globulins |
|
|
demyelinating diseases (4)
|
1. Progressive multifocal leukoencephalopathy (PML)
2. Acute disseminated (postinfectious) encephalomyelitis 3. Metachromatic leukodystrophy 4. Charcot-Marie-Tooth disease |
|
|
- demyelination of CNS due to destruction of oligodendrocytes
- rapidly progressive, usually fatal associated with what pathogen? mechanism? |
JC virus
- reactivation of latent viral infection in AIDS patients Progressive multifocal leukoencephalopathy (PML) |
|
|
multifocal perivenular inflammmation and demyelination after infection (i.e. chickenpox, measles) or certain vaccinations (rabies, smallpox)
condition? |
Acute disseminated (postinfectious) encephalomyelitis
|
|
|
AR lysosomal storage disease due to arylsulfatase A deficiency. Buildup of sulfatides leads to impaired production of myelin sheath
|
Metachromatic leukodystrophy
|
|
|
synchronized, high-frequency neuronal firing
types? |
1. partial
2. generalized 3. epilepsy seizures |
|
|
synchronized, high-frequency neuronal firing
1 area of the brain preceded by aura where does it originate from? |
mesial temporal lobe
partial seizure |
|
|
seizure
motor sensory autonomic psychic type of seizure? |
simple partial
|
|
|
impaired consciousness
seizure originating in 1 part of brain type? |
complex partial
|
|
|
types of generalized seizures?
|
1. absence
2. myoclonic 3. tonic-clonic 4. tonic 5. atonic |
|
|
generalized seizure
petit mal 3 Hz no postical confusion blank stare condition? |
absence seizure
|
|
|
generalized seizure
quick, repetitive jerks condition? |
myoclonic seizure
|
|
|
generalized seizure
alternating stiffening and movement condition? |
tonic-clonic seizure
|
|
|
generalized seizure
stiffening condition? |
tonic seizure
|
|
|
generalized seizure
sudden drops commonly mistaken for fainting condition? |
atonic seizure
|
|
|
most common causes of seizures in children (3)
|
genetic
infection (febrile) trauma |
|
|
most common causes of seizures in adults (4)
|
tumors
trauma stroke infection |
|
|
most common causes of seizures in elderly (5)
|
stroke
tumor trauma metabolic infection |
|
|
pt has a headache
mechanism? |
pain due to irritation of structure such as dura, cranial nerves, or extracranial structures...NOT brain parenchyma itself
|
|
|
unilateral headache
4-72 hrs of pulsating pain nausea photophobia phonophobia aura of neurologic symptoms before headache cause? tx? |
irritation of CN V and release of substance P, CGRP, vasoactive peptides
tx: propranolol, sumatriptan (acute), NSAIDS Migraines |
|
|
bilateral headache
>30 minutes of steady pain not aggravated by light or noise no aura condition? |
tension headache
|
|
|
unilateral headache
repetitive brief headaches periorbital pain associated with ipsilateral lacrimation rhinorrhea Horner's syndrome more common in males tx? |
sumatriptan
Cluster headache |
|
|
common causes of headaches
|
1. subarrachnoid hemorrhage (worst headache of my life)
2. meningitis 3. hydrocephalus 4. neoplasia 5. arteritis |
|
|
illusion of movement
(NOT dizziness or lightheadness) condition? |
vertigo
|
|
|
peripheral vertigo
cause? diagnosis method? |
inner ear etiology
1. semicircular canal debris 2. vestibular nerve infection 3. Meniere's disease dx: positional testing --> delayed horizontal nystagmus |
|
|
central vertigo
cause? diagnosis method? |
brain stem or cerebellar lesion
1. vestibular nuclei 2. posterior fossa tumor dx: positional testing --> immediate nystagmus in any direction, may change directions |
|
|
congential disorder with port-wine stains (aka nevus flammeus), typicall in V1 opthalmic distribution
ipsilateral leptomeningeal angiomas pheochromocytomas this condition can cause what complications? |
glaucoma
seizures hemiparesis mental retardation Sturge-Weber syndrome - occurs sporadically |
|
|
hamartomas in CNS, skin, organs
cardiac rhabdomyoma renal angiomyolipoma subependymal giant cell astrocytoma mental retardation seizures hypopigmented "ash leaf spots" shagreen patch condition? |
tuberous sclerosis
|
|
|
cafe-au-lait spots
lisch nodules (pigmented iris hamartomas) neurofibromas in skin optic gliomas pheochromocytomas defective gene and chromosome? |
NF-1 on chromosome 17
Neurofibromatosis type I (von Recklinghausen's disease) |
|
|
cavernous hemangiomas in skin, mucosa, organs
bilateral renal cell carcinoma hemanigoblastoma in retina, brain stem, cerebellum pheochromocytomas defective gene and chromosome? |
VHL tumor suppressor gene on chromosome 13
von Hippel-Landau disease |
|
|
what are the typical symptoms of mass effects in the brain? (3)
|
seizures
dementia focal lesions |
|
|
primary brain tumors
chance of metastases? location in adults? location in kids? |
- rarely undergo metastases (altho most brain tumors ARE the result of metastases)
- adult = supratentorial - child = infratentorial |
|
|
adult
most common primary brain tumor prognosis? location? diagnosis method? |
- very bad (<1 year life expectancy)
- cerebral hemispheres - stain astrocytes for GFAP glioblastoma multiforme (grade IV astrocytoma) |
|
|
"butterfly glioma"
what would you see histologically? |
"pseudopalisading" pleomorphic tumor cells - border central areas of necrosis and hemorrhage
|
|
|
adult
second most common primary brain tumor location? origin? |
- convexities of hemispheres and parasaggital region
- arises from arachnoid cells external to brain Menigioma |
|
|
seizure, dementia, focus defects
you see spindle cells concentrically arranged in a whorled pattern - psammoma bodies (laminated calcifications) condition? |
meningioma
|
|
|
3rd most common primary brain tumor
localized to CN VIII --> acoustic - found at cerebellopontine angle - S-100 positive what condition would you find this in bilaterally? |
neurofibromatosis type 2
Schwannoma |
|
|
primary adult tumor in frontal lobes
chicken-wire capillary pattern "fried egg" cells (round nuclei with clear cytoplasm) what condition? |
Oligodendroglioma
|
|
|
most common prolactinoma
adult primary brain tumor bitemporal hemianopia (pressure on optic chiasm) Rathke's pouch condition? |
Pituitary adenoma
|
|
|
childhood primary brain tumor
well circumscribed GFAP positive benign, good prognosis what structures would you see histologically? |
eosinophilic, corkscrew fibers (rosenthal fibers)
pilocytic astrocytoma |
|
|
child primary brain tumor
highly malignant cerebellar tumor a form of primitive neuroectoderm tumor (PNET) can compress 4th ventricles --> hydrocephalus what would you see histologically? |
rosettes or perivascular pseudorosette
solid, small blue cells medulloblastoma |
|
|
childhood primary brain tumor
bordering 4th ventricle --> hydrocephalus poor prognosis perivascular rosettes rod-shaped blepharoplasts (basal ciliary bodies) found near nucleus type of tumor? |
Ependymoma
|
|
|
childhood primary brain tumor
cerebellar foamy cells and high vascularity can produce EPO --> secondary polycythemia what condition is this tumor associated with? |
von Hippel-Landau angiomas
Hemangioblastoma |
|
|
childhood primary brain tumor
benign confused with pituitary adenoma (can also cause bitemporal hemianopia) most common childhood supratentorial tumor calcification common origin? |
Rathke's pouch
Craniopharyngioma |
|
|
cingulate (subfalcine) hernitation under falx cerebri
what vessel is compressed? |
anterior cerebral artery
|
|
|
uncal herniation
what vessel is compressed? |
posterior cerebral artery
|
|
|
duret hemorrhages
result of what? |
cerebellar tonsillar herniation into the foramen magnum
|
|
|
increased ICP
ipsilateral dilated pupil/ptosis cause? |
stretching of CN III (innervates levator palpebrae)
uncal herniation |
|
|
increased ICP
contralateral homonymous hemianopia cause? |
compression of ipsilateral posterior cerebral artery
|
|
|
increased ICP
ipsilateral paresis cause? |
compression of contralateral crus cerebri (Kernoham's notch)
|
|
|
brain lesion
ring-enhancing possibilities? |
metastases
abscesses toxoplasmosis (multiple) AIDS lymphoma (single) |
|
|
brain lesion
uniformly enhancing lesion possibilities? |
lymphoma
meningioma metastases (usually ring enhancing) |
|
|
brain lesion
heterogeneously enhancing possibilities? |
glioblastoma multiforme
|
|
|
glaucoma drugs
a-agonist reduces aqueous humor synthesis due to vasoconstriction contraindication? |
epinephrine
do NOT use in closed-angle glaucoma! |
|
|
glaucoma drugs
a-agonist reduces aqueous humor synthesis no vasoconstriction |
Brimonidine
|
|
|
glaucoma drugs
b-blockers reduce aqueous humor secretion (3) adverse effects? (3) |
timolol
betaxolol carteolol non-specific 1. bronchoconstriction 2. vasospasm 3. hypoglycemia |
|
|
glaucoma drugs
diuretic mechanism? |
inhibit carbonic anhydrase --> decreased HCO3 --> decreased aqueous humor secretion
Acetazolamide |
|
|
glaucoma drugs
cholinomimetics increase outflow of aqueous humor contract ciliary muscle and open trabecular meshwork which would you use for emergencies and why? |
pilocarpine - very effective at opening trabecular meshwork into canal of Schlemm
Direct: pilocarpine, carbachol Indirect: physostigmine, echothiophate |
|
|
glaucoma drugs
prostaglandin mechanism? would effect would you see? |
increases outflow of aqueous humor
darkens color of iris (browning) Latanoprost (PGF2a) |
|
|
pt was treated for pain, cough, diarrhea, and acute pulmonary edema with drugs that open K+ channel, close Ca+ channels --> reduce synaptic transmission
toxicities of these type of drugs? |
addiction
respiratory depression constipation miosis(pinpoint pupils) CNS depression opioids |
|
|
opioids inhibit the release of what substances? (5)
|
1. ACh
2. NE 3. 5-HT 4. glutamate 5. substance P |
|
|
partial agonist at opioid "mu" and "kappa" receptors
advantage over full opioid agonists? |
causes less respiratory depression
Butorphanol |
|
|
very weak opioid agonist
also inhibits serotonin and NE reuptake (works on multiple neurotransmitters) use? |
chronic pain
tramadol |
|
|
pt has partial seizures
what drugs can you use? |
everything except ethosuximide and benzodiazepines
|
|
|
pt has tonic-clonic seizures
first line drugs? (3) |
phenytoin
carbamazepine valproic acid |
|
|
absence seizures
first line drug? |
ethosuximide
|
|
|
status epilepticus
first line drug for prophylaxis? |
phenytoin
|
|
|
status epilepticus
first line drug for acute? |
benzodiazepines (diazepam or lorazepam)
|
|
|
antiepileptic drugs
which drugs inactivate Na channels? |
phenytoin
carbamazapine lamotrigine topiramate valproic acid |
|
|
antiepileptic drugs
which drugs ^GABA transmission? |
topiramate
phenobarbital valproic acid benzodiazepines tiagabine (inhibits GABA reuptake) levetiracetam vigabatrin (irreversibly inhibits GABA transaminase) |
|
|
antiepileptic drugs
which drugs primarily inhibits HVA Ca+ channels? |
Gabapentin
|
|
|
antiepileptic drugs
which is first line for trigeminal neuralgia? |
carbamazapine
|
|
|
antiepileptic drugs
which is also used for peripheral neuropath and bipolar disorder? |
Gabapentin
|
|
|
antiepileptic drugs
first line for pregnant women, children |
Phenobarbital
|
|
|
antiepileptic drugs
which drug is also used for myoclonic seizures? |
valproic acid
|
|
|
antiepileptic drugs
which drugs are also used for seizures of eclampsia? what is first line for these seizures? |
Benzodiazepines
first line is MgSO4 |
|
|
epilepsy drug toxicities
sedation tolerance dependence |
benzodiazepines
|
|
|
epilepsy drug toxicities
diplopia ataxia agranulocytosis aplastic anemia liver toxicity induction of P450 SIADH Stevens-Johnson syndrome |
Carbamazapine
|
|
|
epilepsy drug toxicities
GI distress fatigue headache urticaria Stevens-Johnson syndrome |
Ethosuximide
|
|
|
epilepsy drug toxicities
sedation tolerance dependence induction of cytochrome P450 |
Phenobarbital
|
|
|
epilepsy drug toxicities
Nystagmus diplopia ataxia gingival hyerplasia hirsutism megaloblastic anemia SLE-like induction of cytochrome P450 teratogenesis (fetal hydantoin syndrome) |
Phenytoin
|
|
|
epilepsy drug toxicities
GI distress fetal hepatoxicity neural tube defects (spinal bifida) tremor weight gain CONTRADINDICATED in pregnancy |
Valproic acid
|
|
|
epilepsy drug toxicities
Steven's Johnson syndrome |
Lamotrigine
Carbamazapine Ethosuximide |
|
|
epilepsy drug toxicities
sedation ataxia |
Gabapentin
|
|
|
epilepsy drug toxicities
sedation mental dulling kidney stones weight loss |
topiramate
|
|
|
use-dependent blockage of Na channels
^ refractory period inhibition of glutamate release from excitatory presynaptic neuron clinical use? toxicity? |
tonic-clonic seizures
- also a class IB antiarrythmic - nystagmus, ataxia, diplopia, SLE-like phenytoin |
|
|
phenobarbital
pentobarbital thiopental secobarbital mechanism of action? treatment of overdose? |
^ GABA-A action by increasing the DURATION of Cl- channel opening --> decrease neuron firing
respiratory assistance ^ BP Barbituates |
|
|
in which condition are baribituates contraindicated?
|
porphyria
|
|
|
diazepam
lorazepam triazolam temazepam midazolam mechanism? |
^ GABA-A action by ^ the frequency of Cl- channel opening
- reduces REM sleep |
|
|
anxiety
spasticity status epilepticus detox night terrors sleepwalking general anesthetic what drug category do you use to treat these? how do you treat an overdose? |
benzodiazepines
- flumazenil (competitive antagonist at GABA receptor) |
|
|
Zolpidem
zaleplon eszopiclone mechanism of action? uses? |
act via BZL receptor subtype, reversed by flumazenil
- insomnia nonbenzodiazepine hypnotics |
|
|
Anesthetic general principles
drug with low solubility in blood induction speed? recovery time? |
rapid induction
rapid recovery |
|
|
Anesthetic general principles
drug with high solubility in lipids potency? MAC? |
high potency
low MAC |
|
|
diazepam
lorazepam triazolam temazepam midazolam mechanism? |
^ GABA-A action by ^ the frequency of Cl- channel opening
- reduces REM sleep |
|
|
anxiety
spasticity status epilepticus detox night terrors sleepwalking general anesthetic what drug category do you use to treat these? how do you treat an overdose? |
benzodiazepines
- flumazenil (competitive antagonist at GABA receptor) |
|
|
Zolpidem
zaleplon eszopiclone mechanism of action? uses? |
act via BZL receptor subtype, reversed by flumazenil
- insomnia nonbenzodiazepine hypnotics |
|
|
Anesthetic general principles
drug with low solubility in blood induction speed? recovery time? |
rapid induction
rapid recovery |
|
|
Anesthetic general principles
drug with high solubility in lipids potency? MAC? |
high potency
low MAC |
|
|
N20 vs. Halothane
blood & lipid solubility? induction speed? potency? |
N20
- low solubility - fast induction - low potency Halothane is opposite |
|
|
mechanics of anesthetics
in lungs |
^ rate+depth of ventilation = ^ gas tension
|
|
|
mechanics of anesthetics
in blood |
^ blood solubility = ^ blood/gas partition coefficient = ^ solubility = ^ gas required to saturate blood = slower onset of action
|
|
|
mechanics of anesthetics
in tissue (e.g. brain) |
AV concentration gradient ^ = ^ solubility = ^ gas required to saturate tissue = slower onset of action
|
|
|
Halothane
enflurane isoflurane sevoflurane nitrous oxide effects? toxicity? |
myocardial depression
respiratory depression nausea/emesis ^ cerebral blood flow tox: - Hepatotoxicity (Halothane) - Nephrotoxicity (Methoxyflurane) - convulsions (enflurane) - malignant hyperthermia |
|
|
intravenous anesthetics
high potentcy, high lipid solubility, rapid entry into brain - used for induction of anesthesia and short surgical procedures - reduces cerebral blood flow |
thiopental - barbituates
|
|
|
what are the main intravenous anesthetics? (5)
|
barbituates (thiopental)
benzodiazepines (midazolam) ketamine opiates propofol |
|
|
pt undergoing endoscopy
what anesthetic do you use? what would you need to use with it? adverse effects? |
midazolam
- coupled with gaseous anesthetics and narcotics - AE: severe postop respiratory depression, hypotension, and amnesia |
|
|
how does ketamine work?
effect on CV system? adverse effects? |
block NMDA receptors
- cardiovascular stimulant, increases cerebral blood flow AE: disorientation, hallucination, and nightmares |
|
|
intravenous anesthetics
used for rapid anesthesia induction and short procedures advantage? |
less postop nausea than thiopental
- potentiates GABA Propofol |
|
|
procaine
cocaine tetracaine amides (all have two I's in their name) - lidocaine - mepivacine - bupivacaine mechanism? |
block Na+ channels by binding preferentially to ACTIVATED channels --> most effective on rapidly firing neurons
local anesthetics |
|
|
different in mechanism b/w regular local anesthetics (esters?) and teritary amines?
|
regular esters: block Na channels by binding to specific receptors on the INNER portion of the channel
teritary amines: penetrate membrane in unchanged form, then bind to ion channels as charged form, then bind to ion channels as charged form |
|
|
effect of acidity on effectiveness of local anesthetics?
|
less effect in infected (acidic) tissue because alkaline anesthetics are charged and cannot penetrate membrane effectively --> more anesthetic is needed
|
|
|
local anesthetics
order of nerve blockade? |
small > large
myelinated > unmyelinated size > myelination = small myelinated fibers > small unmyelinated > large myelinated > large unmyelinated fibers |
|
|
local anesthetics
order of loss |
pain (first) > temperature > touch > pressure (last)
|
|
|
local anesthetics
usually given with what? exception? |
usually given with vasoconstrictors (epinephrine) --> enhance local action to stop bleedng
|
|
|
pt has a local painful wound
pt is allergic to esters, what type of local anesthetics do you give them? possible toxicities? |
amides
CNS excitation severe CV toxicity (bupivacaine) HTN/hypotension, arrhythmias (cocaine) |
|
|
need to immobilize pt during surgery
what type of receptor are these drugs selective for? |
selective for motor (vs. autonomic) nicotinic receptor
|
|
|
pt got a depolarizing muscle relaxant drug
now has hypercalcemia and hyperkalemia cause? |
succinylcholine
|
|
|
pt experiencing negative effects from neuromuscular blocking drugs
what drugs can you use to reverse it and when? |
cholinesterase inhibitors (neostigmine)
can only use in Phase II (repolarized but blocked) because Phase I is a prolonged depolarization (cholinesterase inhibitors would actually make the muscle blockade WORSE) |
|
|
tubocurarine
atracurium mivacurium pancuronium type of drugs? mechanism? how would you reverse it? |
nondepolarizing neuromuscular blockers
- compete with ACh for receptors - reversal: neostigmine, edrophonium, and other cholinesterase inhibitors |
|
|
pt on operating table has malignant hyperthermia
what caused it? how do you treat it? |
cause - inhalation anesthetics (except N2O) and succinylcholine
treat w/ dantrolene |
|
|
what would you use dantrolene to treat?
mechanism? |
1. malignant hyperthermia
2. neuroleptic malignant syndrome (from antipsychotic drugs) mechanism - prevents release of Ca from the sarcoplasmic reticulum of skeletal muscle |
|
|
condition from excess cholingeric activity and loss of dopaminergic neurons
|
Parkinson's disease
|
|
|
different strategies to treat Parkinson's disease? (4)
|
1. Agonize dopamine receptors
2. increase dopamine 3. prevent dopamine breakdown 4. curb excess cholingeric activity |
|
|
pt w/ Parkinson's
you want to agonize dopaminer receptor drug? |
Bromocriptine
pramipexole ropinirole (non-ergot, preferred) |
|
|
pt w/ Parkinson's
you want to ^ dopamine. drug? what is this drug also used for? toxicity? what other drug? |
1. Amantidine
- also used as an antiviral against influenza A and rubella - toxicity: ataxia 2. L-dopa/carbidopa (converted to dopamine in CNS) |
|
|
pt w/ Parkinson's
want to prevent dopamine breakdown. drug? (2) mechanism? |
Selegiline (selective MAO type B inhibitor)
- entacapone, tolcapone (COMIT inhibitors - prevent L-dopa degradation --> increase dopamine availability) |
|
|
pt w/ Parkinson's disease w/ sweating, diarrhea, etc
you want to curb excess cholingeric activity. drug? |
Benztropine (Antimuscarinic - improves tremor and rigidity but has little effect on bradykinesia)
|
|
|
pt has essential and familial tremors
tx? |
propranolol (Beta-blocker)
|
|
|
Parkinson's pt
you want to increase dopamine in the brain and something that can cross the blood-brain barrier drug? toxicity? what is it given with to prevent these effects? |
Levodopa (L-dopa)/carbidopa
tox - arrhythmias from peripheral conversion to dopamine. Long term use --> dyskinesia, akinesia - given w/ carbidopa (peripheral decarboxylase inhibitor) --> ^ bioavailability of L-dopa in the brain and reduces peripheral effetcs |
|
|
enzyme that preferentially metabolizes dopamine over NE and 5-HT
what drug inhibits this? use? |
Selegiline
MAO-B |
|
|
Alzheimers drug
NMDA receptor antagonist helps prevent excitotoxicity (mediated by Ca+2) toxicity? |
Dizziness
confusion hallucinations Memantine |
|
|
Donapezil
galantamine rivastigmine mechanism? toxicity? |
acetylcholinesterase inhibitor
toxicity - nausea, dizziness, insomnia |
|
|
dopamine - increased
GABA - decreased ACh - decreased what disease? tx? |
Huntington's
Reserpine + tetrabenazine = amine depleting Haloperidol - dopamine receptor antagonist |
|
|
5-HT1B/1D agonist
causes vasoconstriction inhibition of trigeminal activation and vasoactive peptide release drug? use? toxicity? contraindications? |
sumatriptan
for migraine, cluster headaches tox - coronary vasospasm, mild tingling contraindicated - in pt w/ CAD or prinzmetal's angina), mild tingling |