Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
|
A 29-year-old G1P0 at 41 weeks gestation presents for a prenatal visit. Her prenatal course is complicated by tobacco abuse and intermittent prenatal care. Her last visit was at 35 weeks. Prenatal labs are unremarkable except cervical DNA probe positive for Chlamydia, which was treated, and a Pap smear with low-grade squamous intraepithelial lesion. Ultrasound at 21 weeks was consistent with gestational age. Her vitals reveal a blood pressure of 128/76; pulse 74; and temperature 98° F (36.7° C). Fundal height is 39 cm with estimated fetal weight of 2700 gm. Cervix is dilated to 1 cm, 50% effaced, -2 station. What is the next best step in the management of this patient?
A. Non-stress test B. Vibroacoustic stimulation test C. Oxytocin challenge test D. Return visit in one week E. Cesarean section |
Non-stress test
|
|
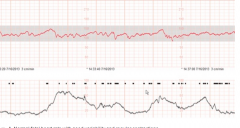
A 29-year-old G1P0 at 41 weeks gestation presents in early labor. The prenatal course was uncomplicated. Ultrasound at 21 weeks was consistent with gestational age. Her vitals reveal a blood pressure of 128/76; pulse 74; and she is afebrile. Fundal height is 36 cm with estimated fetal weight of 2700 gm. Cervix is dilated to 1 cm, 50% effaced and the fetal vertex is at -2 station. The nurse calls you to evaluate the fetal tracing. Which statement best describes the tracing seen below?
|
. Normal fetal heart rate with good variability and regular contractions
|
|
Normal fetal heart rate with good variability and regular contractions
B. Fetal tachycardia with good variability and regular contractions C. Normal fetal heart rate with poor variability and irregular contractions D. Fetal tachycardia with poor variability and regular contractions E. Normal fetal heart rate with good variability and irregular contractions |
Fetal tachycardia with poor variability and regular contractions
|
|
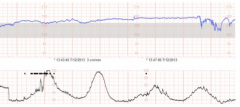
A. Late deceleration
B. Variable decelerations C. Early decelerations D. Sinusoidal rhythm E. Normal fetal heart rate pattern |
Early decelerations
|
|
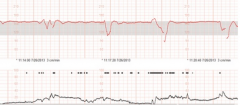
A. Normal fetal heart rate pattern
B. Sinusoidal rhythm C. Late deceleration D. Variable deceleration E. Early deceleration |
Variable deceleration
|
|
|
A 19-year-old G1P0 at 39 weeks gestation presents in labor. She denies ruptured membranes. Her prenatal course was uncomplicated and ultrasoundat 18 weeks revealed no fetal abnormalities. Her vital signs are: blood pressure 120/70; pulse 72; temperature 101.0° F (38.3° C); fundal height 36 cm; and estimated fetal weight of 2900 gm. Cervix is dilated to 4 cm, 100% effaced and at +1 station. She receives 10 mg of morphine intramuscularly for pain and soon after has spontaneous rupture of the membranes. Light meconium-stained fluid was noted and, five minutes later, the fetal heart ratetracing revealed variable decelerations with good beat-to-beat variability. What is the most likely cause for the variable decelerations?
A. Umbilical cord compression B. Meconium C. Maternal fever D. Uteroplacental insufficiency E. Morphine administration |
Umbilical cord compression
|
|
|
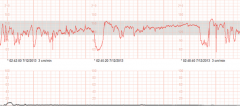
A 29-year-old G1P0 at 42 weeks gestation presents to labor and delivery because of intermittent contractions. She denies ruptured membranes. Her prenatal course was uncomplicated. Her vital signs are: blood pressure 140/96; pulse 72; afebrile; fundal height 32 cm; and estimated fetal weight of2900 gm. Cervix is closed, 25% effaced, -2 station. The fetal heart rate tracing shows occasional late decelerations. Of the following, what is the nextbest step in management?
A. Maternal left lateral position B. Intrauterine resuscitation with terbutaline Start an amnioinfusion Begin magnesium sulfate Augment labor with oxytocin |
Maternal left lateral position. Initial measures to evaluate and treat fetal hypoperfusion include a change in maternal position to left lateral position which increases perfusion to the uterus, maternal supplemental oxygenation, treatment of maternal hypotension, discontinue oxytocin, consider intrauterine resuscitation with tocolytics and intravenous fluids, fetal acid-base assessment with fetal scalp capillary blood gas orpH measurement. An amnioinfusion may be used to treat patients with variable decelerations
|
|
|
A 36-year-old G1 woman presents in active labor. Her past medical history and prenatal course were complicated by chronic hypertension and superimposed preeclampsia. She received magnesium sulfate for seizure prophylaxis and oxytocin augmentation. She undergoes an uneventful spontaneous vaginal delivery. Postpartum, she has a 1000 ml hemorrhage due to uterine atony. Her blood pressure is 130/80; pulse 96; and she is afebrile. Which of the following uterotonic agents is contraindicated in this patient?
A. Oxytocin B. Methylergonovine C. Prostaglandin F2-alpha D. Prostaglandin E2 E. Misoprostol |
Methylergonovine. Methylergonovine is an ergot alkaloid, which is a potent smooth muscle constrictor. It is also a vasoconstrictive agent and should be withheld from women with hypertension and/or preeclampsia. Misoprostol, non-FDA approved, is used for cervical ripening and labor induction.
|
|
|
A 19-year-old G1 woman at 40 weeks gestation has an uncomplicated vaginal delivery followed by a brisk hemorrhage. Her past medical history is significant for steroid-dependent asthma. Her blood pressure is 110/70; pulse 84; and she is afebrile. Which of the following uterotonic agents should not be used in this patient?
A. Intramuscular oxytocin B. Intravenous oxytocin C. Prostaglandin F2-alpha D. Prostaglandin E1 (Misoprostol) E. Methylergonovine |
Prostaglandin F2-alpha. Prostaglandin F2-alpha (Hemabate) is a potent smooth muscle constrictor, which also has a bronchio-constrictive effect
|
|
|
. Factors that lead to an over-distended uterus are risk factors for uterine inversion
|
Grand multiparity, multiple gestation, polyhydramnios and macrosomia are all risk factors. The most common risk factor, however, is excessive (iatrogenic) traction on the umbilical cord during the third stage of delivery.
|
|
|
A 37-year-old G2P1 woman with poorly controlled chronic hypertension presents in labor at term. Her prenatal course was uncomplicated. She delivers a 3500 gram infant spontaneously after oxytocin augmentation of labor. Immediately postpartum, she experiences excessive bleeding. Her blood pressure is 130/90; pulse 84; and she is afebrile. On examination, uterine fundus is firm and the placenta is intact. Which of the following is the most appropriate next step in the management of this patient?
A. Exploration for lacerations B. Methylergonovine C. B Lynch suture D. IV push of oxytocin E. Uterine artery embolizatio |
Exploration for lacerations. After ensuring appropriate backup, establishing intravenous access and stabilizing a patient as needed, the first steps in the management of postpartum hemorrhage are to make sure the uterus is well-contracted, there is no retained placental tissue and to look for lacerations. This patient has a firm fundus, which indicates a contracted uterus. Her placenta is complete, which typically rules out retained placental tissue, so it is important to rule out lacerations,
|
|
|
A 30-year-old G4P3 woman at 24 weeks gestation is found to have an anterior placenta previa. She has a history of three prior Cesarean deliveries. What is the most likely serious complication that can lead to obstetric hemorrhage in this woman?
A. Placental abruption B. Uterine dehiscence prior to labor C. Uterine inversion D. Placenta accreta E. Uterine atony |
Placenta accreta. Placental abruption and uterine atony are both common, but, in the presence of a low-lying anterior placenta in a patient with a history of multiple Cesarean births, the diagnosis of the placenta accreta must be entertained
|
|
|
A 28-year-old G3P2 woman presents in labor at 39 weeks gestation and delivers a 3500 gram infant spontaneously after oxytocin augmentation of labor. Thirty minutes later, the placenta has not delivered. Her past medical history is significant for leiomyoma uteri. Her prenatal course was uncomplicated. What is the most likely risk factor for retained placenta in this case?
A. Placental abruption B. Labor augmentation C. Leiomyomas D. Multiparity E. Circumvallate placenta |
Leiomyomas
The following are associated with retained placenta: prior Cesarean delivery, uterine leiomyomas, prior uterine curettage and succenturiate lobe of placenta. |
|
|
A 37-year-old G4P3 woman presents in labor at term. Her medical history and prenatal course are uncomplicated. She delivers a 3500 gram infant spontaneously after oxytocin augmentation of labor. Immediately postpartum, there is excessive bleeding greater than 2000 cc. She has an IV in place. There are no lacerations and the uterus is found to be boggy. Which of the following is the most appropriate next step in the non-operative management of this patient?
A. Intravenous misoprostol B. Intramuscular misoprostol C. Intravenous prostaglandin F2-alpha D. Intramuscular prostaglandin F2-alpha E. Intravenous oxytocin push |
Prostaglandin F2-alpha should be administered intramuscularly. It could also be injected directly into the uterine muscle. Prostaglandin F2-alpha should not be administered IV, as it can lead to severe bronchoconstriction. Oxytocin is administered as a short time, rapid infusion of a dilute solution (20-80 units in a liter) and not as an IV bolus/push. Misoprostol (800 to 1000 mcg) can be administered orally or rectally and is not administered IV or IM.
|
|
|
A 23-year-old G1P0 woman presents in labor at term. Her prenatal course was uncomplicated. She delivers a 3500 gram infant spontaneously after oxytocin augmentation of labor. Immediately postpartum, there is excessive bleeding greater than 2000 cc. There are no lacerations and the uterus is found to be boggy. Her blood pressure is 90/40; pulse is 120. Conservative and medical management have failed and you proceed with an exploratory laparotomy. Which of the following is the most appropriate next step in the management of this patient?
A. Cervical artery ligation B. Ovarian artery ligation C. External iliac artery ligation D. B-Lynch suture E. Hysterectomy |
B-Lynch suture. A uterine compression suture such as a B-Lynch has been shown to be effective in the management of unresponsive uterine atony. Ligation of a number of pelvic vessels can lead to reduction in the vascular pressure in the pelvis thus controlling hemorrhage. This is especially true with internal iliac artery (hypogastric artery) ligation. However, ligation of the ovarian arteries should not be undertaken as a primary approach. Ligation of the external iliac artery results in devascularization of the leg and, therefore, should not be performed. If these more conservative maneuvers fail, hysterectomy may be necessary but should be a last resort considering the age and parity of the patient.
|
|
|
A 20 year-old G1P1 delivered her first baby 24 hours ago. Delivery was uncomplicated and she had an epidural placed for analgesia at 5 centimeters of cervical dilation. Earlier in the afternoon, she was complaining of a headache and was given ibuprofen. Three hours later, she complained of increasing headache, photophobia and nausea. She denies heavy bleeding. Vital signs are pulse 110; respirations 20; temperature 101.5°F, 38.6°C; and blood pressure 100/50. Physical examination reveals obvious distress, as she has her eyes covered and pain when she moves her neck. Her lungs are clear and heart has a regular rate. Her abdomen is nontender, and uterine fundus is easily palpable just below the umbilicus and is nontender. Her extremities reveal no erythema, swelling or tenderness. Which of the following would be your next diagnostic step?
A. Chest x-ray B. Urinalysis C. Lumbar puncture D. CBC with differential E. Pelvic ultrasound |
Lumbar puncture. Epidurals are used commonly for pain relief during labor. Complications of epidural include spinal headache, localized back pain and meningitis. Symptoms of meningitis progress rapidly and require aggressive treatment with antibiotics. Diagnosis is made with evaluation of the cerebral spinal fluid from a lumbar puncture.
|
|
|
Thirty-six hours ago a 23 year-old G1P1 delivered vaginally and sustained a 2nd-degree laceration. She had a prolonged first stage of labor, ruptured membranes for 26 hours and received penicillin for group B Strep prophylaxis. She now complains of increasing abdominal pain, cramping and heavy foul smelling lochia. Her vital signs reveal a temperature of 100.0° F, 37.8° C; pulse 80; blood pressure 120/60; and respirations 18. She has a tender uterine fundus that measures at the umbilicus. Her extremities reveal mild bilateral edema; no erythema or tenderness. Blood work reveals a white count of 12.2; hematocrit of 34%; and normal chemistries. Her urinalysis is positive for blood and negative for WBCs, leukocyte esterase and nitrites. In addition to ampicillin, which of the following would be the best antibiotic choice?
A. Erythromycin B. Gentamicin C. Doxycycline D. Vancomycin E. Ciprofloxacin |
Gentamicin. Endomyometritis is a common complication of prolonged labor, prolonged rupture of membranes and multiple vaginal examinations. The infection is polymicrobial, mostly anaerobic and requires broad spectrum antibiotics for treatment until the patient is afebrile for 24 hours. By adding Gentamicin, you are covering the spectrum of gram-negative organisms.
|
|
|
A 23 year-old G1P1 delivered vaginally a 42-week infant after a prolonged induction of labor. She had an epidural, with an indwelling catheter for 36 hours and three IV sites for her intravenous medications. She now complains of lower abdominal pain, frequency and dysuria. Her vital signs are temperature 98.6°F , 37°C; pulse 70; blood pressure 100/60; and respirations 12. On examination, her lungs are clear, cardiac exam is normal, abdomen is soft, uterine fundus is firm and nontender, and she has mild suprapubic tenderness. Which of the following organisms is most likely causing her discomfort?
A. Group A streptococcus B. Gardnerella vaginalis C. Chlamydia trachomatis D. Escherichia coli E. Group B Streptococcus |
Escherichia coli. Acute cystitis is a common complication after vaginal delivery and the risk increases with the use of an indwelling catheter
|
|
|
A 23 year-old G1P1 delivered her first baby two days ago after an uncomplicated labor and vaginal delivery. She wants to breast feed and has been working with the lactation team. Prior to discharge, her temperature was 100.4°F, 38°C (other vitals were normal). She denies urinary frequency or dysuria and her lochia is mild without odor. On examination, her lungs are clear, cardiac exam normal, and abdomen and uterine fundus are nontender. Her breasts are firm and tender throughout, without erythema and nipples are intact. Which of the following is the most likely cause of her fever?
A. Endomyometritis B. Septic pelvic thrombophlebitis C. Mastitis D. Breast engorgement E. Vaginitis |
Breast engorgement. D. Breast engorgement is an exaggerated response to the lymphatic and venous congestion associated with lactation. Milk “let-down” generally occurs on postpartum day 2 or 3. If the baby is not feeding well, the breast can become engorged, which can cause a low-grade fever.
|
|
|
A 23 year-old G1P1 is 5 days post-operative from a Cesarean section for arrest of labor at 7 centimeters. She now complains of minimal abdominal pain and drainage from the right side of the incision. Lochia is normal and she has no urinary complaints. Her vital signs are normal and she is afebrile. On physical exam, her lung and cardiac examinations are normal. Her abdomen and uterine fundus are nontender. Her Pfannenstiel incision has erythema extending 3 centimeters from the incision and there is purulent, bloody drainage coming from the right side. What is the next best step in the management of this patient?
A. Initiate intravenous antibiotics B. Initiate oral antibiotics C. Occlusive dressing to the wound D. Open drainage of wound E. Tropical antibiotics to the wound |
Open drainage of wound. Mixed bacteria originating from the skin, uterus and vagina cause wound infections after a Cesarean section. Treatment requires opening the wound, checking for fascia dehiscence and drainage of the purulent material. Packing the wound until it has healed from the bottom up prevents persistent infection. Broad spectrum antibiotics are started, but alone will not treat the abscess. Hot packs may relieve some minor symptoms, but is not adequate treatment alone.
|
|
|
A 22 year-old delivered her first baby five days ago after a prolonged labor and subsequent Cesarean section for arrest of cervical dilation at 7 centimeters. Fever was noted on postoperative day 2 and, despite broad spectrum antibiotics, she continues to have temperature spikes above 101.3°F, 38.5°C. She is eating a normal diet and ambulating normally. On physical examination, her breasts have no erythema and nipples are intact. Her abdomen is soft, uterine fundus is firm and nontender, and her incision is healing without induration or erythema. She has normal lochia and her urinalysis is normal. Pelvic examination reveals a firm nontender uterus and no adnexal masses or tenderness. Which of the following is the most likely cause of her fevers?
Endometritis Mastitis Ovarian abscess Cystitis Septic pelvic thrombophlebitis |
Septic pelvic thrombophlebitis. Septic thrombophlebitis involves thrombosis of the venous system of the pelvis. Diagnosis is often one of exclusion of other causes, but sometimes a CT scan will reveal thrombosed veins. Treatment requires addition of anticoagulation to antibiotics and resolution of fevers is rapid. Anticoagulation treatment is short-term. Classic clinical findings for endometritis include fever and maternal tachycardia, uterine tenderness and no other localizing signs of infection. The clinical manifestations of cystitis include lower abdominal pain, frequency, urgency and dysuria. The clinical findings in patients with mastitis include fever, tenderness, induration and erythema of the affected breast.
|
|
|
A 32 year-old delivered a 9-pound baby and sustained a 4th-degree laceration two days ago. The delivery was complicated by a shoulder dystocia. The laceration was repaired in layers in the customary fashion. She now complains of increasing perineal pain, fever chills and weakness. Her vital signs are: blood pressure 90/50; pulse 120; and temperature 102.2°F 39°C. Her abdomen is soft, nontender and her uterine fundus is firm and nontender. Her perineum is erythematous, swollen and the laceration edges are grey. The laceration site is nontender and without feeling but there is tenderness of the surrounding tissue. What is the most likely etiology for her fevers?
A. Endomyometritis B. Necrotizing Fascitis C. Cellulitis D. Hematoma E. Proctocolitis |
Necrotizing Fascitis. ecrotizing fascitis, a dangerous infection caused by gas forming organisms, such as Clostridium, can quickly cause sepsis and death. Classic clinical manifestations include fever, pain and induration of the wound. Treatment involves early recognition, antibiotics and debridement of the necrotic tissue. Cellulitis presents as swollen, erythematous, tender and warm area, but without grey necrotic edges
|
|
|
A 23-year-old G1P0 patient at 24 weeks gestation requires treatment for depression. She has no other pregnancy complications. In addition to counseling, she begins therapy with fluoxetine (Prozac). Which of the following symptoms is the most common side effect of her therapy?
A. Fatigue B. Sleep disturbance C. Headache D. Irritability E. Agitation |
Sleep disturbance. While all the side effects listed are reported in patients on fluoxetine, an SSRI antidepressant medication, the most common side effect is insomnia
|
|
|
A 29-year-old G1P0 is at 11 weeks gestation. She has a history of depression which has been well controlled with fluoxetine (Prozac). Although the medication is very helpful in controlling her depression, she is concerned about potential side effects on her neonate. Which of the following conditions in the neonate is associated with maternal use of Fluoxetine during pregnancy?
A. Seizures B. Hypotonia C. Pulmonary hypertension D. Temperature instability E. Intracranial hemorrhage |
. Pulmonary hypertension
|
|
|
A 22-year-old patient with regular periods reports tension, depressed mood and decreased productivity towards the end of each cycle. She is otherwise healthy and maintains a high-profile job. Her past medical history is benign and she denies prior psychiatric problems. She denies smoking and drinks alcohol socially. What is the next best step in the management of this patient?
A. Reassure her that her monthly symptoms are normal B. Initiate anti-depressant therapy C. Psychiatry consult D. Ascertain the timing of her symptoms each month E. Initiate psychotherapy |
Ascertain the timing of her symptoms each month. Symptoms of Premenstrual Dysphoric Disorder occur in the luteal phase and are absent in the beginning of the follicular phase. It is therefore important to document the timing of symptoms each month when considering a diagnosis of Premenstrual Dysphoric Disorder. Additionally, it is important to ascertain that these symptoms are not an exacerbation of an underlying psychiatric disorder before initiating therapy.
|
|
|
A 19-year-old G1 at 40 weeks gestation reports that she is postterm and wants to be induced. She has had an uncomplicated pregnancy. Her blood pressure is 124/76 and her pulse is 84. What gestational age would define postterm pregnancy?
A. The due date B. 40 completed weeks C. 41 completed weeks D. 42 completed weeks E. 43 completed weeks |
42 completed weeks
|
|
|
A 29-year-old G1 is at 42 weeks gestation based on her last menstrual period and a first trimester ultrasound. Of the following, what factor is most likely to be associated with postterm pregnancy?
A. Placental sulfatase deficiency B. Fetal adrenal hyperplasia C. Fetal alpha-fetoprotein deficiency D. Fetal renal anomalies E. Fetal chromosomal abnormalities |
Placental sulfatase deficiency
|
|
|
A 20-year-old G2P1 is at 41 weeks gestation. Her prenatal course and past history are unremarkable. She has not had any complications with her pregnancy and fetal surveillance is reassuring. Which of the following complications is most likely to occur in this pregnancy?
A. Preeclampsia B. Retained placenta C. Postpartum hemorrhage D. Macrosomia E. Placenta abruption |
Postterm pregnancies are associated with macrosomia, oligohydramnios, meconium aspiration, uteroplacental insufficiency and dysmaturity. Gestational diabetes is associated with macrosomia, but is not alone a risk factor for postterm pregnancies. There is no associated risk for preeclampsia in postterm gestations.
|
|
|
Question 4 of 10Point value 0 - 1
A 32-year-old G2P1 is at 41 weeks gestation. Her cervix is long and closed. She does not report contractions and states there is good fetal movement. The patient strongly desires not to have an induction of labor. She would like to wait until she goes into labor spontaneously. Which of the following treatment options is optimal at this time? A. Perform a non-stress test (NST) and amniotic fluid index (AFI) twice a week with induction of labor for a nonreactive non-stress test or oligohydramnios B. Patient should perform daily fetal movement counts and proceed with induction for decreased fetal movement C. Perform daily biophysical profiles and deliver if 4 or less D. Immediate induction of labor E. Immediate Cesarean section |
Perform a non-stress test (NST) and amniotic fluid index (AFI) twice a week with induction of labor for a nonreactive non-stress test or oligohydramnios
|
|
|
A 22-year-old G2P1 has a history of a previous postterm pregnancy. She delivered a 3500 g healthy male infant at 42-½ weeks gestation via a Cesarean section secondary to fetal distress. She is currently 15 weeks pregnant, based on an irregular last menstrual period. What is the most appropriate management at this time?
A. Plan for a repeat Cesarean section at 38 completed weeks B. Schedule for a repeat Cesarean section if she does not go into spontaneous labor by 40 weeks gestation C. Plan to admit the patient for an induction of labor (a VBAC) if she does not go into spontaneous labor by 41 weeks gestation D. Obtain a fetal ultrasound to date the pregnancy E. Start weekly non-stress tests and amniotic fluid indexes at 40 weeks gestation and proceed with either induction of labor or Cesarean section for a nonreactive non-stress test or oligohydramnios or if patient has not gone into spontaneous labor by 41 weeks gestation |
Obtain a fetal ultrasound to date the pregnancy. Approximately 50% of patients with a history of a postterm pregnancy will experience prolonged pregnancy with the next gestation. The diagnosis of postterm pregnancy is based on the establishment of an accurate gestational age. In a patient with irregular menses, it is important to obtain an ultrasound prior to 20 weeks to accurately date the pregnancy. It is reasonable to allow a patient with reassuring fetal surveillance to go past 41 weeks gestation. However, because of a prior Cesarean birth, consideration should be given to delivery before 41 weeks.
|
|
|
A 32-year-old G2P1 is at 42 weeks gestation. Her prenatal course was uncomplicated and she had a first trimester ultrasound confirming dates. Her cervix is 4 cm dilated and 100% effaced. She does not report contractions and states there is good fetal movement. What is the next best step in the management of this patient?
A. Ultrasound to assess amniotic fluid volume B. Twice weekly non-stress test (NST) and amniotic fluid index (AFI) C. Daily biophysical profiles D. Induction E. Ultrasound to assess fetal growth |
Induction. Optimal management for the patient with a favorable cervix at greater than or equal to 41 weeks gestation is delivery. Her dilation and effacement make it likely her induction will be successful. Induction of labor in a patient with an unfavorable cervix increases the risk of Cesarean section significantly, compared to a patient who goes into spontaneous labor. It is not advisable to follow a patient who is >42 weeks with antepartum fetal testing, such as twice weekly non-stress tests with amniotic fluid index, if the gestational age is certain.
|
|
|
A 22-year-old G1P1 with no prenatal care delivered a 2100 g male infant who looks like an old man. The pediatricians estimate the gestational age to be greater than 43 weeks. Of the following, which finding is not associated with the dysmature postdate infant?
A. Peeling skin B. Smooth skin C. Meconium-stained D. Long nails E. Fragile |
Smooth skin. The incidence of infants with dysmaturity approaches 10% when the gestational age exceeds 43 weeks. Infants are described as withered, meconium stained, long-nailed, fragile and have an associated small placenta. These infants are at great risk for stillbirth.
|
|
|
A 22-year-old G1 presents at 42 weeks gestation. Her cervix is long and closed. She does not report contractions and states there is good fetal movement. You discuss the benefits of induction at this time versus waiting until she goes into labor spontaneously. She agrees to proceed with an induction. Which of the following means should be used to ripen the cervix in this patient?
A. Artificial rupture of membranes B. Membrane stripping C. Oxytocin infusion D. Prostaglandin E1 tablet E. RU486 (progesterone antagonist |
Prostaglandin E1 tablet. he American College of Obstetricians and Gynecologists (ACOG) recommendations for the management of postterm pregnancy includes: patient records fetal kick counts, and fetal surveillance using one of the following: NST, CST, biophysical profile and delivery for nonreassuring testing. If the patient has a favorable cervix, induce at 42 weeks and, if the cervix is unfavorable, use cervical ripening agents. Membrane stripping (digital separation of chorioamnion from lower uterine segment) and artificial rupture of membranes cannot be performed in a patient with a closed cervix. Prostaglandins applied locally are the most commonly-used cervical ripening agents.
|