![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
5 principles of Drug theory |
1. Bind specifically (receptor affinity) 2. Alter pathways (existing pathways) 3. Inhibit/Activate (physiological activity) 4. Compare basal (effectiveness) 5. Response proportional (to dose) |
|
|
Most drugs exist in a specific stereo-isomer & have a MW btwn ______ & ______ g/mole |
100 & 1000 g/mole |
|
|
list the following bonds from highest to lowest strength: ionic, hydrogen, covalent, van der waals |
covalent ionic hydrogen van der waals |
|
|
Binding affinity (KD) is a measure of how much of a drug is required to bind ____ of the receptors in a fixed population |
1/2 |
|
|
The (higher/lower) the KD of a drug, the lower its affinity for the receptor |
higher
(bc it takes more of that drug to reach 1/2 saturation) |
|
|
How can KD (equilibrium disassociation constant) be calculated? |
at equilibrium:
KD= K1/K2 = [L][R]/[LR]
L + R --(K1)---> LR L + R <--(K2)-- LR |
|
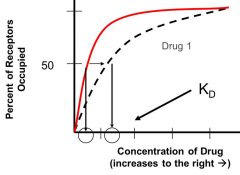
The receptor in this system has the greatest affinity for which of the drugs? |
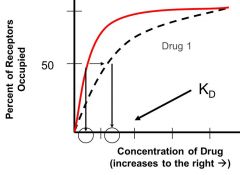
Drug 2
(because it reaches 50% or 1/2 receptor saturation at lower concentration) |
|
|
Define efficacy |
the ability of the ligand (drug) (once bound to the receptor) to generated a biological response (varies from 0-1)
(must have affinity to have efficacy) |
|
|
define full agonist |
-substance that generates maximum biological response in a system, by activating 100% or less of the receptors
-affinity & efficacy = 1
|
|
|
define partial agonist |
-substance that produces less than the maximum achievable response, even when 100% of receptors are bound (only partially activate receptors)
-affinity & efficacy < 0 & > 1 |
|
|
define inverse agonist |
-substance that produces a decrease in the biological activity (from basal) (partially inactivates receptors) |
|
|
Allosteric agonists also increase the biological activity, how do they differ from other agonists? |
the do NOT bind to the agonist binding region, bind to another site & alter receptor conformation to increase efficacy or affinity for other substrates
Ex: Benzodiazepines for Ca2+ receptors |
|
|
define chemical antagonist |
-substrate that binds to agonist & makes it inactive
Ex: chelator, used to treat metal poisoning by binding to Au, Hg, As, etc |
|
|
define physiological antagonist |
-substrate that interacts on the same system as another agonist, independently & causes opposite effects
Ex: ach & epi have opposite effects on heart rate, are antagonists of one another, but do not interact |
|
|
define indirect antagonist
|
-substrate that inhibits a biological response by acting on a site beyond the receptor, agonist still acts on receptor but process is not completed
(usually inhibit agonists that act on multiple receptors)
|
|
|
define competitive antagonist |
-substrate that competes with agonist for binding site, prevents agonist binding & activation, have affinity but no efficacy |
|
|
Define Equilibrium-competitive (reversible) antagonist |
-competitive antagonist that binds reversibly to the receptor
-antagonism CAN be overcome by increasing agonists |
|
|
Define Nonequilibrium- Competitive (irreversible) antagonist |
-competitive antagonist that binds irreversible to the receptor via COVALENT bond
-antagonist CANNOT be overcome by increasing agonist
|
|
|
define allosteric antagonist |
-substrates that reduce the affinity &/or efficacy of agonists by binding to & altering a receptors conformation, do NOT bind to agonist binding region |
|
|
What is a graded response? |
One that changes proportionally w each dose of drug (agonist) given
-each single dose produces a single tissue response, curve is comprised of multiple responses generated separately by individual doses |
|
|
What is a quantal response? |
Response curves represents the "all or nothing" effect at different doses
-each dose produces a response in a certain percentage of test subjects, graph is made up using multiple doses of drug |
|
|
Potency compares the relative effectiveness of drugs that _______________, using ED50 values |
act by similar mechanisms ONLY
ED50= dose at which 50% maximum response is reached |
|
|
T/F ED50 (potency) and KD (affinity) are directly related |
FALSE |
|
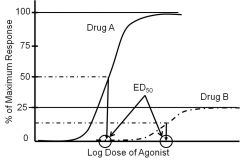
Which drug is more potent? |
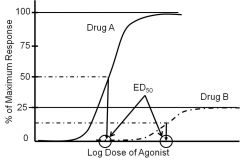
Drug A -has a lower ED50 dose |
|
|
Efficacy (KD) (or intrinsic activity) ranges btwn 0-1 for agonists & _____ for antagonists |
is 0 for antagonists |
|
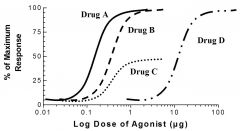
Which drug is most potent? |
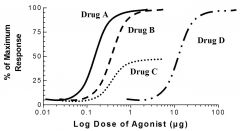
Drug A (A & B have same max, but ED50 is lower for A) |
|
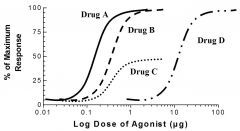
Which drug is a partial agonist? |
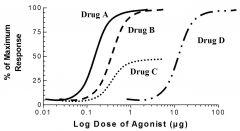
Drug C
-never reaches 100% response |
|
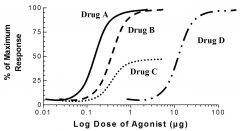
If drug B represents the normal curve, which drug represents a Reversible antagonist? |
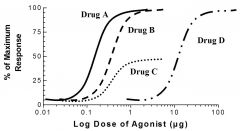
Drug D -Reversible antagonists cause a RIGHT shift = decrease in potency, while still allowing max response |
|
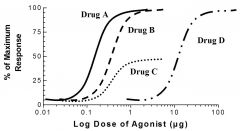
If drug B represents the normal curve, which drug represents an Irreversible antagonist? |
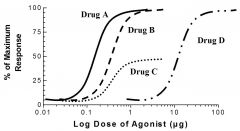
Drug C -Irreversible antagonists cause a DECREASE in MAX response (indirect antagonist will cause same change in graph) |
|
|
What is the only way to reactivate receptors, when nonequillibrium-competitive/ irreversible antagonist has been used? |
via synthesis of new receptors |
|
|
What happens when you add a partial agonist along to a full agonist? |
partial agonist acts as an antagonist bc it takes receptors and has a lower efficacy than the full agonist attached receptors (eventually outcompetes full agonist) |
|
|
________ receptors allow a max response to be achieved when only a small fraction (< 1/2) of receptors are occupied, even with a partial agonist |
spare receptors |
|
|
The fewer spare receptors present, the (more/less) receptors will need to be activated (by a full agonist) to reach maximal effect |
more receptors |
|
|
Most drugs act on (molecules essential to normal cell fxn/ enzymes/ DNA or molecules involved in specific intercellular communication) |
molecules involved in specific intercellular communications |
|
|
4 types of endogenous activators that act on 7-TMS G-Protein coupled receptors |
norepinephrine serotonin acetylcholine histamine
|
|
|
Norepinephrine activates what 7-TMS G-Protein coupled receptors? |
adrenergic receptors (alpha & beta) |
|
|
Serotonin acts on what receptors? |
serotonergice receptors (5-HT receptors) |
|
|
Acetylcholine acts on what receptors? |
muscarinic cholinergic receptors (M1, M2, M3, M4, M5) |
|
|
Histamine acts on what receptors? |
histamine receptors (H1 & H2) |
|
|
What are the 3 main Galpha subtypes? |
alphas, alphai, & alphaq/11 |
|
|
What are the main effectors of as (alphas) ? |
-increase adenyl cyclase activity--> increase cAMP |
|
|
What are the main effectors of ai? |
-decrease adenyl cyclase--> decrease cAMP |
|
|
What are the main effectors of aq/11? |
-increase phospholipase C--> increase protein Kinase C, IP3, & Ca2+ |
|
|
What are the as (a stimulatory) receptors? |
B1 B2 AR glucagon receptor |
|
|
What are the ai (a inhibitory) receptors? |
a2 AR uOR |
|
|
What are the aq/11 receptors? |
a1 AR angiotensin |
|
|
Which 2 subtypes are physiological anatagonists? |
ai & as, act to antagonize each others actions (adenyl cyclase & cAMP, one is inhibitory while other stimulates) |
|
|
Desensitization, tachyphylaxis, tolerance, & adaption all lead to what? |
decrease in receptor activity due to long term dosing
|
|
|
When chronic exposure leads to receptor down-regulation, the only way to increase effect is to ...... |
resynthesize receptors |
|
|
Sensitization (super sensitivity) commonly occurs as a result of ___________ |
receptor blockade removal -causes more receptors to be made, then when removed there is an increase in receptors available = increased drug response |
|
|
_____________ receptors, such as nicotinic ach receptors & GABA receptors, act w/i miliseconds, & can be acted on by ____________ ligands |
Ionotropic receptors (ligand-gated ion channels)
ionic ligands (+ or -) |
|
|
___________ receptors, regulate transcription of genes involved in cell growth & differentation, act w/i minutes/hours/days & can be acted on by ________ ligands |
tyrosine-kinase receptors cytoplasmic enzymes (tyrosine kinase, serine kinase, guanylate cyclase)
extracellular hormones (EGF, insulin, PDGF, ANF)= endogenous activators |
|
|
__________ receptors, such as JAK-STAT receptors, regulate genes involved in inflammation & hematoposis, act w/i hours/day & can be acted on by __________ ligands |
cytokine receptors
extracellular hormones (Growth Hormone, erythropoietin, interferon = endogenous activators |
|
|
___________ receptors, regulate gene transcription, act w/i hours/days & can be acted on by ____________ ligands |
intracellular receptors
hormone ligands: glucocortoids, mineralcorticoids, sex steriods, vit D, thyroid hormones = endogenous activators
|
|
|
What is one property of ALL drugs that act as nuclear receptors? |
hydrophobic |