![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
|
What is physiologic leukorrhea? |
normal vaginal discharge that occurs prior to menstruation or during pregnancy
(HEALTHY discharge) |
|
|
When someone comes in complaining or genital pain what should the focused physical exam consist of? |
1. abdomen, suprapubic tenderness 2. inguinal lymph nodes 3. pelvic exam (external, internal, sample) |
|
|
Normal vaginal pH is < ______ & ODORLESS |
< 4.5
(pH > 4.5 indicated an infection**) |
|
|
What is the KOH amine test?
What is a positive result? |
KOH reacts w/ acidic vaginal fluid & help clear debris to allow for a better view
Postive whiff test= reacts w/ Gardnerella vaginalis or Trichomonas vaginalis & produces a fishy odor |
|
|
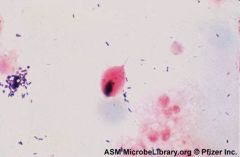
How can a wet mount be used to differentiate Gardnerella vaginalis? |
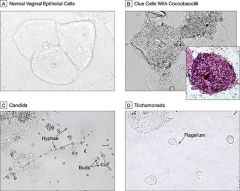
presence of clue cells (w/ coccobaccilli- B) |
|
|
How can a wet mount be used to differentiate Trichomonas vaginalis? |
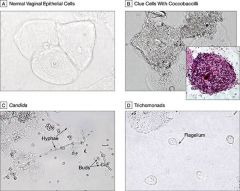
presence of motile trichomonads w/ flagella (D) |
|
|
How can a wet mount be used to differentiate Candida? |
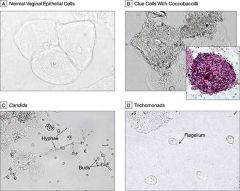
presence of pseudohyphae or budding yeast (C) |
|
|
90% of Vaginitis is caused by either; bacterial vaginosis (gardnerella vaginalis), vulvovaginal candidiasis, & Trichomonias.
Which of these is the MOST COMMON?
Which of these can be transferred to male sexual partners (is an STI)? |
MC= Bacterial Vaginosis= Gardnerella vaginalis
STI= Trichomonas vaginalis |
|
|
Pt comes in complaining of vaginal discharge with a bad smell that increases after sex. Pt has a new bf, an IUD, & douches regularly. She describes discharges as white-grey, homogenous, & non-adherent. likely Dx? confirm w/ what tests? |
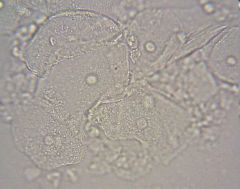
Dx: Bacterial Vaginosis (BV)
wet mount= clue cells present ph > 4.5 KOH amine test = Positive whiff test
|
|
|
How is Bacterial Vaginosis (BV) (Gardnerella vaginalis) treated? |
Metronidazole 500mg PO BID for 7 days |
|
|
Pt comes in complaining of vaginal itching & white, curd-like discharge. Pt recently took antibiotics for a sinus infection & takes birth control. likely Dx? confirm w what tests?
|
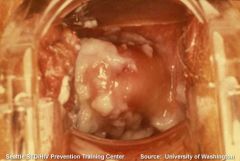
Dx: Vulvovaginal Candidiasis (Yeast infection)
wet mount= hyphae or buds pelvic exam= image |
|
|
How do you tx a Vulvovaginal Candidiasis (yeast infection)? |
Diflucan 150 mg PO X 1 (Topical antifungals) |
|
|
Pt comes in complaining of a frothy, green-yellow vaginal discharge. She has been experiencing pain with intercourse & urination (dyspareunia & dysuria). Likely dx? confirm w/ what tests? |
Trichomoniasis
KOH amine test= Positive whiff test pH > 4.5 wet mount= motile trichomonads |
|
|
How do you tx a Trichomoniasis infection?
|
Metronidazole 2g PO x 1
*also treat male partner** prevent retransfer* |
|
|
Treating a Trichomoniasis infection is considered ___________ prevention |
tertiary prevention -prevents complications such as PID & transmission
(primary prevention= education, secondary prevention= screening exam) |
|
|
Pt comes in complaining of multiple, painful red blisters & sores (ulcers) on his penis. He has been feeling uncomfortable (malaise) & has a headache. He denies having sex with anyone with visible lesions. likely Dx? confirm w/ what test? |
Genital Herpes (HSV 1 or 2)
Viral culture- Tzank smear confirmation (Dx mostly clinical) |
|
|
T/F 70% of HSV transmissions are from asymptomatic viral shedding (no visible lesions) |
TRUE
(only about 10-20% infected ppl even know they have herpes) |
|
|
How can Genital Herpes be managed? (NO CURE) |
antivirals: acyclovir, famciclovir, valcyclovir
(^reduce outbreaks, inc healing, pain relief & dec risk of transmission) |
|
|
What is the MOST PREVALENT STI in the US? |
Human Papillomavirus (HPV) |
|
|
Pt comes in complaining of genital warts (condyloma accuminata). There are no visible lesions on PE. likely Dx? confirm w/ what test? |
Human Papilloma virus (HPV)
pap smear/colposcopy w. abnormal cells |
|
|
How is HPV managed? |
Topical: -Podophyllin -TCA/BCA -Imiquimod -podpfilox
Excision- removes warts but doesn't cure |
|
|
MALE pt comes in complaining of painful urination (dysuria) & penile (urethrea) mucopurulent discharge. likely dx? confirm w/ what? |
Chlamydia trachomatis or Neisseria gonorrhoeae
urethral swab or urine test (best in morning) to differentiate |
|
|
Cervical swabs are very important for detection of what STIs? |
Gonorrhea & Chlamydia
(cause cervicitis) |
|
|
Gonorrhea & Chlamydia are commonly asymptomatic in females. If symptoms present what are they? |
mucopurulent discharge from cervix dysuria inflammed, friable, easily bleeding cervix PID (if untreated) |
|
|
Tx for Chlamydia |
Doxycycline 100 mg PD BID 7 days Azithromycin 1gm PO single dose |
|
|
Tx for Gonorrhea |
Ceftriaxone 400mg PO single dose (or 250mg IM) Azithromycin 2gm PO single dose (^can be used to tx both if unsure/waiting for result) |
|
|
T/F In both Gonorrhea & Chlamydia tx it is important for patients to abstain from any sexual contact for 10 days after beginning antibiotics |
FALSE
ABSTAIN for 7 days (not 10) |
|
|
T/F As a physician, you are responsible to report chlamydia & gonorrhea infections to the Southern Nevada Health District |
TRUE |
|
|
_________ is a serious complication that can result from untreated Chlamydia, Gonorrhea, & genital mycoplasmas infections.
What does this increase the risk for? |
Pelvic inflammatory Disease (PID)
inc risk for ectopic pregnancy, infertility, endometriosis, chronic pelvic pain |
|
|
25 yr old female patient comes in w/ fever & pelvic pain. PE reveals lower abdominal tenderness, adnexal tenderness, cervical motion tenderness. likely dx? confirm w/ what tests? |
Pelvic Inflammatory disease
pelvic ultrasound: free fluid in pelvic cul-de-sac STD screen, pregnancy test, to rule out/in causes |
|
|
PID tx |
outpatient: oral antibiotics
inpatient: IV antibiotics |
|
|
What situations indicate inpatient tx for PID? |
-surgical emergency -pregnancy -immunocompromised -tuboovarian abscess |