![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back

Tactile, pain, temperature. |
Free nerve endings. |
|

Position sense, dynamic fine touch. |
Meissner's Corpuscles. |
|

Vibration, deep pressure. |
Pacinian corpuscles. |
|

Position sense, static touch. |
Merkel's disk. |
|
|
Autoimmune (via molecular mimicry) disorder attacking peripheral nerves and motor fivers of ventral. This causes symmetrical ascending paralysis starting in distal LE. Elevated protein and normal cell count. |
Guillain-Barre Syndrome. (Acute inflammatory demyelinating polyneuropathy.) |
|
|
Hereditary; defective production of proteins of axons and/or myelin sheath. Motor and sensory affected. Classic sx: foot drop (dysfunctional common perineal n). |
Charcot- Marie-Tooth disorder. (Chronic inflammatory demyelinating polyneuropathy.) |
|
|
AR lysosomal storage disease where sulfide buildup impairs myelin production. |
Metachromatic leukodystrophy. |
|
|
Multifocal perivenular inflammation with demyelination occurring after infection of vaccination. |
Acute disseminated encephalomyelitis. |
|
|
Pancoast tumor invades the ______________ (ipsilateral/contralateral) brachial plexus and the ascending cervical sympathetics leading to ______________ (ipsilateral/contralateral) radicular pain and Horner's Syndrome. |
Ipsilateral; ipsilateral. |
|
|
Compression of cervical plexus at level of axilla. |
Saturday night palsy. |
|
|
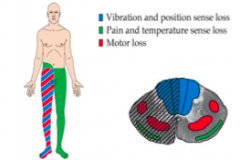
Brown-Sequard syndrome (cord hemisection) |
|
|
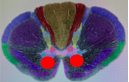
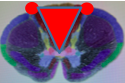
Commisural syndrome |
|

|
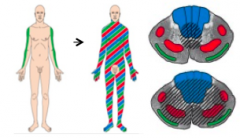
Anterior and posterior cord syndrome. |
|
|
What may cause an anterior and posterior cord syndrome. |
Anterior spinal artery occlusion liely involving T1-T4 or L1. |
|
|
What may cause a commisural syndrome? |
Syringomyelia (usually C8-T1) or tumor. |
|
|
C4- C5 transection. |
Quadriplegia, impaired respiration, SB, AD, OH. |
|
|
C6-C7 transection. |
Quadriplegia, SB, AD, OH |
|
|
C8-T1 transection. |
Hand weakness, paraplegia, SB, AD, OH. |
|
|
T2, T3 transection. |
Paraplegia, SB, AD, OH. |
|
|
T12-L1 transection. |
Paraplegia, SB. |
|
|
L4, L5 transection. |
Paraplegia, SB. |
|
|
S2, S3 transection. |
Flaccid bladder. |
|
4 clinical sx of LMN lesions. |
Weakness, atrophy, fasciculations, absent/diminished deep tendon reflexes. |
|
|
2 examples of LMN Spinal cord syndromes. |
Polio, Werdnigg-Hoffman Disease. |
|
|
2 examples of UMN Spinal cord syndromes. |
Multiple sclerosis, ataxia telangiectasia. |
|
|
4 Clinical sx of UMN spinal cord syndromes. |
Weakness, clasp-knife rigidty, spasticity, hyperreflexia. |
|
|
Cervical cord showing degeneration of axons in lateral corticospinal tract and alpha motor neurons in ventral horn. |
Amyotrophic lateral sclerosis (UMN + LMN spinal cord disorder). |
|

Freidrich's ataxia, Vitamin B12, and Vitamin E deficiencies leads to ______________. |
Tract demyelination. |
|
|
Dementia may be linked with Vitamin ____ deficiency due to degeneration of periventricular white matter. |
B12. |
|
Degeneration of dorsal roots and columns. |
Tabes dorsalis. (Eg tertiary syphilis) |
|
|
At least 3 clinical sx of tabes dorsalis. |
Ataxia, charcot's joints, lightning pains. |
|
|
Radicular pain, sensory loss of all modalities, weakness, lack of DTRs, decreased muscle tone, loss of anal reflex, urinary retention. |
Cauda equina syndrome. |
|
|
(Stroke) Contralateral hemiparesis and hemisensory loss of face and arm. |
Middle cerebral artery. |
|
|
(Stroke) Contralateral paresis and sensory deficit of leg. |
Anterior cerebral a. |
|
|
(Stroke) Contralateral hemiparesis. Purely motor. |
Lenticulostriate aa. |
|

(Stroke) Contralateral sensory deficit --> "Thalamic syndrome." |
Thalamogeniculate aa. |
|

(Stroke) "Suprathalamic syndrome" |
Thalamocortical radiation. |
|
|
Middle cerebral a supplies motor and sensory cortex of _____ and _______ along with Broca's and Wernicke's area. |
Face and arm. |
|
|
Anterior cerebral a supplies motor and sensory cortex of _____. |
Leg. |
|
|
Lenticulostriate aa supply ______ and ______. |
Striatum and internal capsule. |
|
|
Thalamogeniculate aa supply ______. |
VPL Thalamic nucleus |
|
|
(Stroke) Anterior spinal a will cause (ipsilateral/contralateral) ____________________ of leg and (ipsilateral/contralateral) _______________. |
Contralateral hemiparesis & proprioception of leg (lateral corticospinal tract); ipsilateral tongue paresis. |
|
|
(Stroke) Posterior inferior cerebellar a supplies the _____________ and will cause _______________ Syndrome if damaged. |
Lateral medulla; Wallenberg Syndrome. |
|
|
At least 2 clinical sx of Wallenberg Syndrome |
Ipsilateral diminished pain and temperature in face, contralateral diminished pain and temperature in body. |
|
|
(Stroke) Anterior inferior cerebellar a supplies the ___________ and will cause ___________ Syndrome if damaged. |
Lateral pons; lateral pontine syndrome. |
|
|
At least 4 clinical sx of lateral pontine syndrome. |
Vomiting, vertigo, nystagmus, facial paralysis & decreased pain & temperature, Horner's Syndrome |
|
|
(Stroke) Posterior cerebral a supplies ___________ and will present with _____________ if damaged. |
Occipital cortex and visual cortex; contralateral hemianopia with macular sparing. |
|
|
Worst headache of your life? |
Subarachnoid hemorrhage. |
|
|
Paralysis of vertical gaze. |
Dorsal midbrain (Parinaud's) syndrome |
|
|
Vertical gaze is under control of what 3 midbrain structures? |
riMLF, INC, nucleus of fibers of posterior commisure. These control CN 3 and 4. |
|
|
Internuclear opthalmoplegia results from damage to what nuclear structure? |
Damage to medial longitudinal fasciculus (MLF) between CN 6 and CN 3. Injury affects contralateral eye. |
|
|
What two CN's are compromised in facial colic's syndrome of the Pons? |
CN 6, 7 |
|
|
What 3 structures are damaged in medial medullary syndrome (give the sx too) 1) 2) |
1) Cortical spinal tract (contralateral hemiparesis) 2) Medial lemniscus (contralateral loss of proprioception in trunk & extremities) 3) Hypoglossal n (ipsilateral flaccid paralysis of tongue... "lick the wound") |