Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
202 Cards in this Set
- Front
- Back
|
Name the 3 parts of the diencephalon
|
1. thalamus
2. hypothalamus 3. epithalamus |
|
|
what structure blocks the lateral growth of the thalamus during embryological development?
|
the internal capsule
|
|
|
What makes up the rostral boundary of the hypothalamus?
|
the lamina terminalis
|
|
|
What makes up the medial boundary of the hypothalamus?
|
the IIIrd ventricle
|
|
|
What makes up the inferior surface of the hypothalamus?
|
the floor of the IIIrd ventricle
|
|
|
What makes up the superior border of the hypothalamus?
|
The hypothalamic sulcus
|
|
|
What makes up the posterior border of the hypothalamus?
|
The beginning of the cerebral aqueduct
|
|
|
what structure divides the hypothalamus into the medial and lateral zones?
|
The fornix
|
|
|
Where is the medial forebrain bundle found and where does it run?
|
found in the lateral region of the hypothalamus. It runs between the forebrain and the reticular formation (it is bidirectional)
|
|
|
What are the 3 zones of the medial region of the hypothalamus?
|
1. pre-optic/supra-optic
2. Tuberal 3. Mammillary |
|
|
What is the function of the pre-optic and supra-optic regions?
|
project to the posterior lobe of the pituitary gland to release AHD and Oxytocin
|
|
|
What nucleus is found in the tuberal zone?
|
The arcuate nucleus - contains neurons that release hypothalamic releasing factors (these factors influence the anterior pituitary)
|
|
|
The main function of the tuberal zone, then, is _____________.
|
endocrine
|
|
|
The dorsomedial and ventromedial nuclei of the tuberal zone play a role in _____________.
|
regulation of appetite
|
|
|
What is a major characteristic of the mammillary zone?
|
Major location where efferent pathways leave the hypothalamus
|
|
|
What are the 3 efferent pathways that leave the hypothalamus via the mammillary zone? Where does each run to?
|
1. mammillothalamic - to anterior thalamic nucleus
2. mammillotegmental - to midbrain reticular formation 3. dorsal longitudinal fasciculus - to brainstem reticular formation and spinal cord. |
|
|
What is the autonomic function of the anterior hypothalamus?
|
parasympathetic functions; also heat disposal (sweating).
|
|
|
What is the autonomic function of the posterior hypothalamus?
|
sympathetic functions; also heat retention (shivering)
|
|
|
Hypothalamic nuclei influence the 4 F's: what are these? What system influences the 4 F's?
|
Feeding, Fighting, Fleeing, Fornication
The limbic system |
|
|
What other connections does the hypothalamus have with the limbic system?
|
amygdala
ant. and dorsomedial nuclei of thalamus |
|
|
Which structure makes up the medial boundary of the thalamus?
|
The IIIrd ventricle
|
|
|
Which structure makes up the lateral boundary of the thalamus?
|
PLIC
|
|
|
Which structure makes up the superior boundary of the thalamus?
|
transverse cerebral fissure (subarachnoid space between corpus callosum and thalamus)
|
|
|
Which structure makes up the inferior boundary of the thalamus?
|
the hypothalamus and hypothalamic sulcus
|
|
|
The structure that splits the thalamus into 4 groups groups of nuclei is ___________?
|
the internal medullary lamina
|
|
|
What is the thalamic reticular coat?
|
a surrounding structure that overlies the lateral and anterior thalamus (aka. the reticular nucleus)
|
|
|
The thalamus sends out 4 types of radiations - name them
|
1. anterior
2. Superior 3. Posterior 4. Inferior |
|
|
Regarding the anterior thalamic radiations:
1. Where do they begin 2. Run in what structure 3. Where do they project? |
1. start in anterior and medial thalamic groups
2. run in ALIC 3. project to frontal lobe |
|
|
Regarding superior thalamic radiations:
1. Where do they begin 2. Run in what structure 3. Where do they project |
1. start in VPL, VPM, VL
2. run in PLIC 3. project to sensorimotor strip (areas 1, 2, 3, 4, 6) |
|
|
Regarding posterior thalamic radiations?
1. Where do they begin 2. Run in which structure 3. where do they project |
1. start in LGN, Pulvinar
2. run via optic radiations 3. project to area 17; occipital lobe |
|
|
Regarding Inferior thalamic radiations:
1. where do they begin? 2. run in which structure 3. project to where? |
1. MGN
2. run in auditory radiations 3. project to temporal lobe and insular cortex, Area 41 |
|
|
What is meant by the fact that VPM and VPL have "reciprocal connections?"
|
VPM & VPL project to somesthetic strip (areas 1,2,3). If you knock out VPL and VPM: cortical neurons will die. If you knock out the somesthetic strip: neurons in VPM and VPL die.
|
|
|
Pulvinar:
1. Inputs? 2. Outputs? |
1. areas 18, 19
2. inferior parietal lobe |
|
|
Dorsomedial Nucleus:
1. Inputs? 2. Outputs? |
1. Amygdaloid complex, temporal neocortex
2. Prefrontal Cortex |
|
|
Anterior Nuclei:
1. Inputs? 2. Outputs? |
1. mammillothalamic tract (from hypothalamus), fornix
2. Cingulate gyrus |
|
|
VA:
1. Inputs? 2. Outputs? |
1. Globus Pallidus
Substantia Nigra 2. Frontal Cortex (Area 6) |
|
|
VL:
1. Inputs? 2. Outputs? |
1. Globus Pallidus
Substantia Nigra Dentate Nucleus (from cerebellum) 2. Area 4 (Motor Cortex) |
|
|
VPL:
1. Inputs? 2. Outputs? |
1. Medial Lemniscus
Spinothalamic tracts 2. Areas 1, 2, 3 - sensory cortex |
|
|
VPM:
1. Inputs? 2. Outputs? |
1. Trigeminothalamic nucleus
2. Areas 1,2,3 - sensory cortex |
|
|
LD Output?
LP Output? |
To Caudate Nucleus
To Superior parietal lobe |
|
|
LGN:
1. Inputs? 2. Outputs? |
1. Optic Tract
2. Optic Radiations to Area 17 |
|
|
MGN:
1. Inputs? 2. Outputs? |
1. Inferior colliculus, lateral lemniscus
2. Auditory Radiations to Areas 41, 42 |
|
|
Branches of the internal carotid supply which portion of the thalamus?
|
The anterior nuclear group
|
|
|
What is the blood supply to anteromedial aspect of the thalamus?
|
Posteromedial striatal arteries (aka. thalamoperforant arteries): branches from PCmA
|
|
|
What is the blood supply to VPM, VPL, LGN, MGN?
|
posterolateral striatal arteries (aka. thalamogeniculate arteries): branches of the PCA
|
|
|
the _____cortex covers the cerebral hemispheres; it has six distinct cellular layers
|
neocortex
|
|
|
the ______cortex is also known as the hippocampus; it has four cellular layers
|
Archicortex
|
|
|
the _____cortex is found on the ventral surface of the cortex and the parahippocampal gyrus; it has three cellular layers
|
Paleocortex
|
|
|
There are three basic types of neurons in the cerebral cortex. Name them.
|
1. Projection Neurons
2. Association Neurons 3. Commissural neurons |
|
|
Elaborate on projection neurons
|
send axons to areas of the CNS that lie outside of the cortex
|
|
|
Elaborate: association neurons
|
connect cortical regions to the same hemisphere
|
|
|
Elaborate: commissural neurons
|
connect cortical regions to the contralateral hemisphere
|
|
|
General rule: projection fibers arise from _________, while association and commissural fibers arise from _________.
|
deep neocortex
superficial cortex |
|
|
What are the largest and most prominent neurons in the cortex?
What type of fibers do they give rise to? |
*pyramidal neurons
*association fibers or projection fibers |
|
|
What characterizes a stellate nueron and where are these neurons found?
|
Stellate neurons have extensive dendrites projecting from all directions of the cell body. THey are found in layer IV (internal granular)
|
|
|
Where are fusiform neurons found?
What type of nerve fibers do they form? |
In the deepest cortical layers.
They form projection fibers |
|
|
What are the Horizontal Cells of Cajal AND the Cells of Martinitti?
|
Other types of neurons found in the cortex
|
|
|
In general: cortical efferent fibers originate in layer (lamina) _____, while thalamic projections originate in ____.
|
cortical efferent fibers - lamina VI
Thalamic projections - lamina V |
|
|
List the cellular Cortical layers from superficial to deep.
|
I. Molecular
II. External granular layer III.External pyramidal layer IV. Internal granular layer V. Internal pyramidal layer VI. Fusiform layer |
|
|
The molecular layer contains mainly _________ fibers.
|
horizontal
|
|
|
The external granular layer is comprised of _________.
|
small densely packed granule cells
|
|
|
What is notable about layer III?
|
This is a very prominent layer and consists of pyramidal neurons arranged in two sub-layers.
|
|
|
The two sub layers of the external pyramidal layer are made up of ________ and _______.
|
outer layer - medium sized neurons
inner layer - larger pyramidal cells |
|
|
The external pyramidal layer (III) gives rise to what type of fibers?
|
Association and commissural fibers.
|
|
|
What makes up the internal granular layer (IV)?
|
densely packed stellate neurons and bands of Baillarger (horizontal fiber layer)
|
|
|
What makes up the internal pyramidal layer (V)
|
pyramidal neurons, granule neurons, neurons of Martinotti, and internal band of Baillarger.
|
|
|
Which type of fibers does the internal pyramidal layer (V) give rise to?
|
projection fibers
|
|
|
What makes up the fusiform layer (VI)
|
small fusiform nuerons with dendrites that project to other cortical layers.
|
|
|
The fusiform layer gives rise to what type of fibers?
|
Projection fibers
|
|
|
What is characteristic of visual cortex nerve firing patterns?
|
The visual cortex has functional columnar units - the whole column fires at once.
|
|
|
Radial fibers project from _______ to ________.
|
from inside to out. (medullary region to cortex)
|
|
|
Tangential fibers project ________, parallel with the _________.
|
horizontally, parallel with the cortical surface.
|
|
|
List the three basic types of circuits in the neocortex.
|
1. point to point
2. local 3. divergent |
|
|
Point to point circuits are major __________ and _________ pathways such as the __________ (2 categories)
|
afferent and efferent
cortico-cortical circuits Thalamo-cortical circuits |
|
|
Are point to point circuits (+) or (-)?
|
(+)
|
|
|
Point to point circuits are well suited to transfer what type of informations?
|
precise, topographically organized information
|
|
|
Are local circuits (+) or (-)
|
(-) or (+) (although there is more (-) than (+)).
|
|
|
Inhibitory local circuits use __________ as a neurotransmitter.
|
GABA
|
|
|
Divergent circuits use ___________ as a neurotransmitter.
|
Monoamines
|
|
|
Divergent circuits are well suited for __________________.
|
activites that involve cohesive activity of large areas of neocortex such as attention, arousal, mood.
|
|
|
Cortico-cortico projections connect _______________. Example?
|
cortices within hemispheres. Ie. frontal cortex with visual cortex
|
|
|
Commissural Cortical Fibers connect ________________.
|
the hemispheres via the anterior and posterior commissures or the corpus callosum
|
|
|
There are two anatomical differences between the R and L hemispheres of the brain. What are they?
|
1. L tempo-parietal cortex has more tissue
2. L lateral fissure is longer (at a shallower angle) |
|
|
1. The use of sodium amytal in the early days?
2. What kind of a drug is sodium amytal? |
1. injected into internal carotid to find out hemispheral dominance (it temporarily "paralyzes" neurons in that area.
2. barbituate |
|
|
What is the result of amytal injected into the dominant lobe?
|
Loss of ability to speak
|
|
|
Amytal injected in the left ICA will produce __________, whereas amytal injected into the right ICA will produce __________/
|
left - depression
right - euphoria |
|
|
if there is cortical damage to a child sparing the right hemisphere - what will be the influence on language?
|
Damage to the R hemisphere in children is not so significant: they "adapt" so their speech is adequate. Above the age of 6 this observation is not seen.
|
|
|
In general, will cortical damage to the right hemisphere effect language skills?
|
No
|
|
|
What is the operculum and where is it located?
|
associated with 2 main areas of language (Broca's & Wernicke's). It is located in the area around the lateral sulcus overlying the insula.
|
|
|
What area of the brain is called the writing area? Where is this located?
|
Exner's area - superior to Broca's area in premotor cortex.
|
|
|
What are the two parts of Wernicke's area? What is their main function?
|
1. traditional Wernicke's area (anterior) - spoken language
2. angular gyrus (btwn visual and auditory cortex) - written language |
|
|
T/F: The arcuate fasciculus is bidirectional.
|
True
|
|
|
The "modern" view of language areas lists 3 area networks. What are they?
|
1. Conceptual - concepts from higher cortices
2. mediational - intermediary btwn. conceptual and implementation.(around B & W) 3. Implementation - controls articulation and grammar. (B, W, insula, basal ganglia) |
|
|
In regards to the temporal cortex:
1. place/people's names go here 2. tools/utensil names go here 3. Common names (dog) go here. |
1. anterior
2. posterior 3. inferior |
|
|
What is the insula responsible for in regards to language function?
What would a lesion in this location look like? |
motor planning for speech. A lesion would result in trouble saying words accurately.
|
|
|
What is the medial frontal cortex responsible for in regards to language function?
What would a lesion in this location look like? |
"desire" to communicate
lesion results in mutism |
|
|
What are CN nuclei responsible for in regards to language function?
|
motor, sensory and parasympathetic aspects of speech
|
|
|
Define prosity
Where is this function found? |
timing, intonation and stress of language. Function found in right cortex.
|
|
|
Define pragmatics.
Where is this function found? |
language appropriate to social settings. (a lesion will cause innapropriate actions and inability to "get" jokes). Found in right cortex
|
|
|
The area of the brain responsible for familiar voices, music and rythm is _____________.
|
The right cortex
|
|
|
Communication vs. language
What is thinking? |
communication: transmit ideas
language: transmit abstract ideas thinking = the ability to have ideas |
|
|
1. define phonology
2. define morphology 3. Define syntax 4. define semantics |
1. speech sounds (phonics)
2. combining sounds into words 3. combining words to form sentences 4. relation of phonology and syntax to meaning |
|
|
T/F: intelligence correlates with language.
|
False. Language is separate from intelligence.
|
|
|
Aphasia is an UMN problem. name the two types of aphasia
|
1. expressive aphasia - cannot transform thought into spoken or written information
2. receptive aphasia - cannot transform spoken or written information into thoughts. |
|
|
define logorrhea
|
excessive output of words
|
|
|
Conduction aphasia is damage to ____________. How does it present?
|
arcuate fasciculus
can comprehend and produce meaningful speech: have word finding problems, cannot repeat sentences |
|
|
1. Damage to higher cortical areas that initiate speech is _____________ aphasia. 2. How would this present?
|
1. transcortical motor aphasia (info does not pass from higher centers)
2. presents as: intact comprehension, can repeat long sentences, trouble initiating speech. |
|
|
1. Damage to the posterior end of the lateral sulcus would result in ____________ aphasia.
2. How would this patient present? |
1. Transcortical sensory aphasia (info does not pass to higher centers)
2. fluent speech, can repeat long sentences, echolalia, anomic aphasia, can repeat sentences (vs. Wernicke's - can't repeat sentences) |
|
|
1. What is global aphasia?
2. How would this patient present? |
1. damage to the Left hemisphere and basal ganglia.
2. severe impairment of understanding and language expression. may retain automatic speech (ie. counting) |
|
|
What is anomic aphasia?
|
trouble finding a name for objects
|
|
|
define: alexia
|
lack reading. damage in angular gyrus: disrupt pathways to language centers.
|
|
|
define: agraphia
|
lack writing. damage to Exner's area
|
|
|
Define: dysarthria
|
motor speech problem (LMN) located in brainstem or CN nuclei of fibers. Only affects muscles
|
|
|
define: apraxia
|
disorder of programming muscles of articulation. (cannot combine sounds to form a word)
|
|
|
define: dysphonia
|
disorder of the larynx
|
|
|
define: amusia
|
lesion of Right parietal, occipital or temporal cortex resulting in inability to recognize familiar voices, music and rythm.
|
|
|
define: akinetic mutism
|
lose motivation to speak (usually temporary). Damage is to medial frontal cortex
|
|
|
define: agnosia
|
lack of sensory recognition of speech (due to lesioned sensory association areas)
|
|
|
What is a characteristic of lesions to the Right hemisphere? This finding is characteristic of a __________ lobe lesion.
|
Contralateral Neglect (fail to act with or acknowledge left side of body). This is characteristic of a parietal lobe lesion.
|
|
|
Failure to respond to stimuli on one side of the body is known as __________.
|
inattention. If stimulus in strong enough pt. will respond
|
|
|
How can you confirm inattention in a patient?
|
by double simultaneous stimulation. Elicit a moderate stimuli on both sides - results in extinction of inattention side.
|
|
|
Extinction is defined as:
|
failure of the inattention side to respond to double simultaneous stimulation.
|
|
|
How can extinction and innattention be overcome?
|
by elicing a strong stimulus: that will be noticed on the inattention side.
|
|
|
Regarding music: if you are untrained it is percieved in the ___(1)________ cortex. If trained (professional) it is perceived in the ____(2)_____ cortex. If you are singing it comes from the ______(3)____ cortex.
|
1. Right
2. Left 3. right |
|
|
What are the three components of the 3 neuroaxis model of brain functioning?
|
1. Right-Left Axis
2. Anterior-Posterior Axis 3. Up-Down Axis |
|
|
What are the three components to a functioning memory?
|
1. Encoding
2. Storage 3. Retrieval |
|
|
Cortical dementias would be a problem in which component of memory?
|
Storage
|
|
|
Test Anxiety is a classic example of which component of memory?
|
Retrieval
|
|
|
In adults, a common aquired neurological problem of the LH is __________. In children it is __________.
|
Adults - aphasia
Children - dyslexia |
|
|
reading comprehension, prosodic expression and comprehension, Calculation of spacial alignment: these are all characteristics of which hemisphere?
|
RH
|
|
|
Which hemisphere of the brain allows us to apply "affect" to our statements?
|
RH
|
|
|
Damage to which hemisphere results in a more severe spacial attention loss (severe contralateral neglect)
|
Damage to the RH.
|
|
|
What is meant by executive functions?
|
control or self-regulatory functions that ORGANIZE and DIRECT all cognitive activity, emotional response and overt behavior.
|
|
|
What is a disorder that has problems with executive function?
|
ADHD
|
|
|
Executive functions have to do with __________. Examples of this include self regulation, planning and organization, social adaptation
|
Performance
|
|
|
'Knowing what to do is not the same as doing what you know' Knowing is a function of which area? What about doing?
|
knowing - posterior based
doing - frontal based |
|
|
The relationship between ______ functions and ______ functions is like the relationship between athletes and their coach.
|
cognitive functions
executive functions |
|
|
The up-down axis mediates communication between __________ and _________.
*give an example |
Cortical gray matter and Subcortical White matter
*frontal system vs. brainstem, hippicampus. (executive functions vs. arousal, attention, motivation) |
|
|
What are some roles of white matter in human behavior?
|
speed of processing
integration retrieval of memories/knowl. organization multitasking |
|
|
Would a disturbance in white matter result in a disturbance of IQ?
|
NO.
|
|
|
What % of PD pts develop dementia?
|
10-30%
|
|
|
Neuroimaging tells you about the _____________ of the brain: neuropsychological eval. tells you about the __________ .
|
structural
function (Structural damage does not always correlate with functional ability) |
|
|
What is pragmatic damage?
|
Talking too much: taking the "scenic route" to expain or define something.
|
|
|
Where is the damage in global aphasia?
|
in both Broca's and Wernicke's areas.
|
|
|
Which hemisphere stroke is at a higher risk for developing depression?
|
LH
|
|
|
An indifference reaction is often observed following a ____ hemisphere CVA.
Symptoms? |
RH or bilateral
Sx. undue cheerfulness, apathy. |
|
|
A frontal heteromodal syndrome of unawareness presents as unawareness of ________? (2)
|
social innapropriatness
planning or anticipation |
|
|
A parietal heteromodal syndrome of unawareness presents as unawareness of _____________? (2)
|
impaired sensory function
hemiplegia, hemi-neglect |
|
|
Catastrophic reaction syndrome is often observed following a ____ CVA. Symptoms?
|
Left anterior-subcortical
Sx: axiety, tears, verbal, physical aggression |
|
|
a left frontal or a basal ganglia lesion often results in ________________. Pt. presents as irritated, anxious, sad, weight loss, trouble sleeping.
|
Depression
|
|
|
What is the disease/problem?
- memory dysfunction - neglect - problems with "affect" - cause sometimes HTN, DM |
Subcortical Vascular disease
|
|
|
The following are all risk factors for what?
hypertension Cardiac disease TIA's Smoking, ETOH, drug abuse Elevated lipids |
Vascular Cognitive Impairment
|
|
|
What is one of the earliest symptoms of cardiovascular disease?
|
HTN
|
|
|
Can there be cognitive decline after CABG?
|
Yes: due to precedures, equipment used.
|
|
|
Mixed dementia is defined as...
|
coexistance of AD and Vascular Dementia (VaD)
|
|
|
Development of AD plaques & tangles may be due to ____________.
|
Ischemia from CV disease
|
|
|
What is the pathophysiology of seizures and epilepsy?
|
Unknown (65-75%)
|
|
|
What are the indications and the MOA of Phenytoin and Carbamezepine?
|
indications: epilepsy
MOA: enhance Na+ activation: result - reduce firing rates |
|
|
Define paroxysmal
|
sudden outburst or alteration of behavior, movement or sensation
|
|
|
Define: ictal
|
during a seizure
|
|
|
Define: post-ictal
|
after a seizure
|
|
|
Define: interictal
|
between seizures
|
|
|
What are the three main classifications for seizures?
|
1. Partial (small area)
2. Generalized (both hemisph) 3. Unclassified |
|
|
Partial Seizures can be further subdivided into two types: Simple (Focal) seizures and Complex seizures. What is difference between the two?
|
Simple (focal) seizures are partial seizures without alteration of consciousness.
Complex Seizures involve an alteration of consciousness. |
|
|
T/F: Partial seizures never evolve to secondary generalized seizures.
|
FALSE. They can evolve.
|
|
|
What is the most common type of epilepsy?
|
Generalized seizure epilepsy
|
|
|
Define: generalized seizures
|
uncontrollable discharge of neurons on both sides of the brain. (they start in one side and spread across the brain)
|
|
|
Do generalized siezures result in a loss of consciousness?
|
Yes. People w/ this type of epilepsy do not remember having a seizure.
|
|
|
Define: myoclonic seizure
|
generalized seizure that involves the motor cortex. (causes twitching and jerking)
|
|
|
What is status epilepticus?
|
A period of frequent, long-lasting seizures WITHOUT regaining consciousness between attacks. Can be fatal; req. medical attention
|
|
|
What are 3 known causes of epilepsy?
|
1. Genetic (defect in genes that encode ion channels)
2. Structural (tumor, infection, excess CSF, Scar tissue) 3. Metabolic (hypoglycemia, hypocalcemia, drug use or abuse) |
|
|
seizures that develop in old age are known as _________?
|
Neurodegerative seizures (often secondary to CVA)
|
|
|
In an EEG: what is the source of current that causes fluctuating scalp potential?
|
Pyramidal neurons
(These are the neurons most prone to seizure activity) |
|
|
What is basic epileptogenesis?
|
Thought to be a biologic event that alters balance between (+) and (-) in neural networks.
|
|
|
Why are EEGs so useful in diagnosing seizures?
|
They are very good at measuring synchronicity of cell firing. In a seizure all the cells fire at once.
|
|
|
T/F: An EEG can read one pyramidal neuron when it fires an AP.
|
FALSE. It takes many thousands of neurons firing at once to generate a signal large enough to detect w/EEG
|
|
|
What is the major EEG rythm seen in normal relaxed adults? (Eyes must be closed)
|
Alpha rythm
|
|
|
What is the major EEG rythm that is normal in infants and sleep: if seen in an adult, it indicates pathology.
|
Theta activity
|
|
|
What is the major EEG rythm that is normal when eyes are open and patients are alert?
|
Beta activity
|
|
|
Spikes, Sharp Waves and Polyspikes on an EEG are known as __________ and are due to ____________.
|
Epileptiform discharges
synchrony of thousands and thousands of firing neurons |
|
|
There are three basic mechanisms used by AEDs. What are they?
|
1. Increased inactivation of Na+ channels - reduces sustained firing
2. Act on synaptic transmission ((+) of (-) neurotransmission or vice versa) 3. Act on NT receptors: enhance GABA receptor action reduce glutamate receptor action |
|
|
The MOA of the older AEDs was/is ____________, whereas the newer drugs are starting to target _____________. Advantage?
|
Na+ channel inactivation
GABA and NMDA receptors Targets are more specific - causes less adverse effects |
|
|
What are 3 other treatment modalities used for seizures?
|
1. Ketogenic diet
2. Vagus Nerve Stimulation 3. Biofeedback |
|
|
T/F: 25-30% of epilepsy patients on AEDs still have inadequate seizure control.
|
True
|
|
|
There are four functional "groups" of the reticular formation. Name them and where they would be found...
|
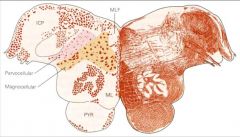
1. Parvocellular (Lateral, small) Group
2. Magnocellular (medial, large) group 3. Paramedian group (PPRF) 4. Raphe group (midline: "Raphe" = seam) |
|
|
What is the function of the Lateral group of the pontomedullary reticular formation?
|
function: local "circuit" control of CN functions. (visceral and motor coordination)
|
|
|
What is the function of the Medial group of the pontomedullary reticular formation?
|
descending: movement and posture, pain modulation
ascending: cortical arousal |
|
|
What is the function of the Paramedian group of the pontomedullary reticular formation?
|
PPRF - controls voluntary horizontal conjugate gaze.
|
|
|
What is the function of the Raphe group of the pontomedullary reticular formation?
|
descending: pain modulation
ascending: cortical arousal, affective behavior |
|
|
There are 3 monoaminergic systems that arise from the brainstem reticular formation. Name them.
|
1. Noradrinergic
2. Seratonergic 3. Dompaminergic |
|
|
The Noradrenergic projections arise from ____________ and project to ________. Functions?
|
Locus ceruleus
project all over the brain function: maintain attentiveness, sleep-wake states and mood. |
|
|
The Seratonergic projections arise from _________ and project to ________. Functions?
|
from midline raphe nuclei
project all over brain. functions: descending: pain modulation, regulation of motor systems ascending: cortical arousal, affective behaviors |
|
|
The Dopaminergic projections arise from two locations. What are they?
|
1. Substantia Nigra
2. Ventral Tegmental Area of midbrain |
|
|
Name the 3 dopaminergic projections, where they start and end, functions.
|
1. mesostriatal - substantia nigra to striatum. (Motor)
2. Mesolimbic - ventral tegmental area to limbic system (emotion, thought memory). 3. mesocortical - ventral tegmental area to prefrontal cortex. (emotion, thought, memory). |
|
|
Cholaminergic projections seem to be involved in _______________?
|
cortical arousal
alertness learning memory |
|
|
The dementia in Alzheimer's disease is contributed to cholinergic projections from ______________.
|
the Basal Nucleus of Meynert. (It has widespread cortical connections)
|
|
|
Histaminergic projections arise from the ___________ and project to the ___________. Function?
|
hypothalamus to the forebrain
function: maintainance of an alert state |
|
|
How does the reticular formation carry out sensory modulation?
|
PAIN MODULATION: they send a descending "reticulospinal" projection to the spinal dorsal horn - influence inhibitory interneurons by releasing enkephalin. Pain neuron transmission inhibited.
|
|
|
What do the pontine and medullary reticulospinal pathways regulate? How?
|
regulate tone and posture
they have descending influences on alpha and gamma motor neurons |
|
|
The descending tectobulbar projections carry out what function of the reticular formation?
|
PPRF = controls voluntary conjugate movement of the eyes.
|
|
|
How does the reticular formation modulate arousal and consciousness?
|
via the RAS. (Reticular activating system)
|
|
|
Alteration of consciousness or arousal states involving bilateral lesions to the reticular formation results in___________.
|
either a coma or persistant vegitative state.
|