![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
In animals, what are the behaviours for recognising animal is asleep? |
•Eyes Shut (humans) •Certain Postures •Inactivity •Reduced muscle tone •Reduced responsiveness (not completely unconscious as you can be awakened) |
|
|
What are the three measurement tools for sleep? |
EEG EOG (Electrooculography; eye movements) EMG (Electromyography; muscle movement, typically on the face/under chin for humans) |
|
|
What is the EEG activity in wakefulness called? |
Beta Activity (13-30 Hz) |
|
|
What are characteristics of Beta Activity? |

Blinks in the eyes. Blob = going into alpha activity Not very sinewavy |
|
|
What is the EEG activity in dosing/mediation called? |
Alpha activity (8-12 Hz) |
|
|
What is the first stage of sleep |
Stage 1 Non-REM Sleep |
|
|
What are typical features of Stage 1 Non-REM Sleep? |
Left Eye rolls backwards and forwards slowly Still have muscle tone EEG has slowed down (theta waves 3-7 Hz) |
|
|
What is a sign that you see a person get into established sleep? |
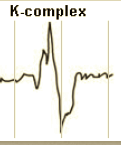
The K-complex: Negative followed by positive deflection - neg. = up, pos. = down Has to last .5-1 second Must be 75 mV in amplitude |
|
|
What is the second stage of sleep? |
Stage 2 Non-REM Sleep |
|
|
What are the typical features of Stage 2 Non-REM Sleep? |
Eyes have stopped rolling Muscle tone has gone down (less amplitude) Presence of K-complexes and sleep spindles |
|
|
What are sleep spindles? |

They have a sort of waxing and waning characteristic to the one second activity. waves are a little faster than alpha 12-14Hz |
|
|
What is the third (and fourth) stage of sleep? |
Stage 3 Non-REM Sleep |
|
|
What are the typical features on Stage 3 Non-REM Sleep? |
K-complexes occur in runs (referred to as Delta waves, 0.5-2 Hz) Must count up delta waves = if more than 20% of the 30 sec page is taken up by delta waves If more than 50% of the 30 sec page is taken up by delta waves then this is considered Stage 4 Non-REM Sleep = much deeper sleep |
|
|
What happens if you get woken up during Stage 4 of sleep? |
Most difficult stage to be woken up Feel quite disorientated - takes a couple of seconds to catch up Have very rationale thoughts, not dreamlike |
|
|
Why does it look like we see lots of eye movements in Stage 3/4 Non-REM Sleep? |
It is just the machinery picking up electrical potentials from around the eyes. So how we determine artifacts from the drivers or cause of electrical activity is to see which movement is bigger from the multiple measures. e.g. if delta wave is bigger than eye movement, you know "eye" activity is an artifact. |
|
|
What are the alternative names for stage 1, stage 2, and stage 3/4 sleep respectively? |
N1 N2 Slow-wave sleep; SWS or N3 (for both stages 3 & 4) |
|
|
What are the characteristics of REM Sleep? |
Rapid Eye movement (slightly slower than blinks, but more quick than eye movement in Non-REM) Muscle atonia = body paralysis (except eye and breathing muscles) Theta waves (3-7 Hz) |
|
|
Can it be difficult to tell Stage 1 Non-REM from REM sleep? |
Yes from if only considering the EEG, but if look at the eye movements and muscle tension, these are the two ways to tell them apart. *Can see some periods of alpha (8-12 Hz), but as long as muscle atonia is present, still REM sleep |
|
|
What are "saw-tooth" waves in relation to REM sleep? i.e. they look like little teeth on the blade of a saw... |

Gradual build-up in negative polarity and then they return to baseline (often occur in runs) |
|
|
What are some other characteristics of REM sleep? |
•Presence of theta activity (desynchronized EEG pattern) •Enhanced and variable respiration and blood pressure •Rapid eye movements (REM) •Pontine-Geniculate-Occipital (PGO) waves •Loss of muscle tone (paralysis) •Vivid, emotional dreams •Signs of sexual arousal |
|
|
Why can REM sleep be used as a measure for impotence? |
If present in REM sleep, then impotence is psychological (functional) and not physical (organic) |
|
|
What are Pontine-Geniculate-Occipital (PGO) waves? |
These are known to occur in animals to measure whether they are asleep. |
|
|
What is the mental activity that occurs during sleep? |
Dreams and nightmares can occur during both SWS and REM |
|
|
What activity occurs in the brain during REM sleep? |
1. REM sleep is accompanied by high levels of blood flow in the visual association cortex but low levels in the primary visual cortex 2. REM eye movements resemble those made when a person scans a visual image |
|
|
How is sleep structure? i.e. the sleep cycles |
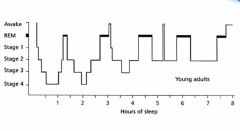
First sleep cycle lasts about 90 min. Towards end of night, no SWS |
|
|
Which age group has the most REM sleep? Hint: they sleep many hours a day |
0-2 year-olds |
|
|
What is the next age group that has the middle large amount of REM sleep? blah< X < blah |
2 - 10 year-olds |
|
|
Even though older people may have the same amount of hours sleep as young people, how does the quality of sleep differ? |
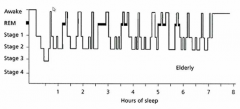
Wake up much more frequently But REM still occurs (even modestly) every 90 mins approx. |
|
|
How have researchers study what the function of sleep actual is? |
Sleep deprivation studies on humans and more in animals |
|
|
What are the three common features that humans display while being sleep deprived? |
1. slight increased appetite 2. impaired cognitive functioning (e.g. concentrate, reduced memory function, perceptual distortions and hallucinations) 3. Does not dramatically impair normal bodily functioning |
|
|
According to Zager, Anderson, Ruiz, Antunes and Tufik (2007), what was the difference between rats who had slept and those who were sleep-deprived? |
Rats which had slept had 20% more white blood cells than those who were sleep deprived suggesting restoration of the immune system. Rats that are completely deprived of sleep showed increased eating but lost weight and eventually became ill and died. |
|
|
What are the evolutionary theories of why sleep is important? |
To protect individuals during the most dangerous types when inactivity is beneficial to survival |
|
|
Which other sleep theory does not have lots of support from the literature, and followed by one that does? |
1. Energy conservation, but the energy dsavings is not that great (not much support) 2. Restoration (brain and body) |
|
|
Why does Restoration theory have more support? |
Learning and Memory and Sleep. But more recent discovery was the glymphatic system (or glymphatic clearance pathway) which is a functional waste clearance pathway for the vertebrate central nervous system (CNS). *This switches on during sleep |
|
|
What is a circadian rhythm? |
a cycle that lasts about a day |
|
|
What is the difference between a circadian rhythm and a diurnal rhythm (24 hour system tool ? |
Circadian - Internal is within the body (e.g. a circadian rhythm, of which light is an external cue for this) Diurnal (24hr mammals typically) is using tools, like alarm clocks, to keep you in routine. |
|
|
Silver, LeSauter, Tresco and Lehman (1996) observed that removal of which structure eradicated the circadian rhythms of hamsters? |
the suprachiasmatic nucleus (SCN) |
|
|
Where is the suprachiasmatic nucleus located? |
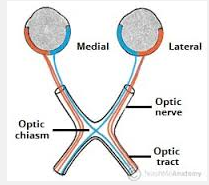
just behind the optic chiasm |
|
|
What are the two pathways that influence the SCN? |
1. the Ganglion cells containing melanopsin 2. the intergeniculate leaflet of the lateral geniculate thalamic nucleus. |
|
|
What the hell is the intergeniculate leaflet of the lateral geniculate thalamic nucleus? |
This is when other external cues, like getting up at the same time of day, eating at the same times (routine stuff), is embodied into the body to remind it of circadian rhythms. |
|
|
How do individual SCN clock cells exhibit circadian rhythms? |
clock cells produced a protein that upon reaching a critical level They switch on if dip below critical limit and switch off if excede critical limit. These proteins are produced by genes. |
|
|
Do these clock cells activity, individually , occur at different times? |
Yes, but combined they broadly synchronise with external "zeitgeber" cues, and the cells also talk to each other and synchronise with eachother. |
|
|
What are the four different sleep disorders mentioned in the lecture? |
1. Narcolepsy 2. Obstruction sleep apnea 3. Sleep Terror and Sleep walking 4. Delayed sleep phase syndrome |
|
|
Are these considered a primary sleep disorder? |
Yes, other sleep disorders can be related to other mental conditions e.g. bipolar ( manic - hardly any sleep; depressive - too much sleep) |
|
|
What are the symptoms of narcolepsy? (typically at least one or more of them present with a diagnosis) |
1. Excessive daytime sleepiness/sleep attacks 2. Cataplexy: loss of skeletal muscle tone in response to strong emotion 3. Hypnagogic hallucinations: hallucinations at the onset (or offset) of sleep. 4. Sleep paralysis: wake up paralysed |
|
|
How are all these symptoms associated with REM sleep? |
–cataplexy - REM sleep atonia –sleep paralysis - REM sleep atonia –hallucinations - intrusion of dreams –REM appears at sleep onset (and in MSLT), as opposed to healthy individuals and 1st REM occurs after 90mins |
|
|
What is the cause of narcolepsy? |
abnormalities to do with Orexin [in dogs] (but narcolepsy can develop even if orexin is fine) mostly commonly develops in teen/twenties, and commonly following an illness/flu vaccination |
|
|
how is narcolepsy diagnosed? |
usually a sleep study - time in the sleep lab |
|
|
What are the three narcolespy factors you might see in a sleep study? |
1. short sleep onset, 2. short REM latency, 3. increased wakefulness (like what we see in elderly) |
|
|
What else is used in the sleep study for diagnosing narcolepsy? |
–Multiple Sleep Latency Test: (rapid sleep onset, REM at sleep onset in most naps) |
|
|
What is treatment for Narcolepsy? |
EDS - planned naps, CNS stimulants (modafinil), sodium oxybate ALSO antidepressants for cataplexy to reduce the amount of REM |
|
|
What are the two kinds of sleep apnea? (only looking at one though) |
–Obstructive (patients try to breathe but can’t) –Central (no breathing efforts are made; brain is not telling them to breath during sleep) |
|
|
What are the two types of breathing events that occur in sleep apnea? |
• APNEA = cessation of airflow • HYPOPNEA = reduction in airflow |
|
|
What does the obstruction of sleep apnea look like? |
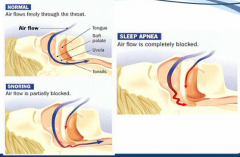
|
|
|
Which stage of sleep is sleep apnea most severe |
REM |
|
|
How often can someone who has severe sleep apnea wake up in the night? |
1-2 a minute - very difficult for them to progress through stages of sleep and REM sleep |
|
|
What are two types of treatment for OSA? |
• BEHAVIOURAL –weight loss (including exercise) –avoidance of alcohol/sedatives before bedtime –avoidance of supine sleeping position • NASAL CPAP (Continuous Positive Airwave Pressure) –non-invasive –short term efficacy –Patient compliance variable (mostly quite poor) *opposite than vacuum cleaner |
|
|
What are some other, more last resort, sleep apnea treatments [3]? |
• ORAL / DENTAL DEVICES –useful in mild cases • OXYGEN • SURGERY (one of the most painful types of surgery) |
|
|
What is the parasomnia spectrum, in relation to the next part of the lecture? |
Mild: Bruxism (teeth grinding)/ Confusional arousals Sleep Talking Sleep walking/eating/sex Sleep Terrors Severe: *Arousal disorders = SWS |
|
|
What are the six general features for these arousal disorders? |
1. Occur in association with an arousal from SWS 2. Mental confusion and disorientation 3. Relative non reactivity to external stimuli 4. Poor response to efforts to provoke behavioural wakefulness 5. Retrograde amnesia for the event 6. Only fragmentary or no recall of dream mentation |
|
|
What is Delayed Sleep Syndrome? |
Delayed circadian rhythm *normal in adolescents |
|
|
What is treatment for Delayed Sleep syndrome? [4] |
• Aim is to re-align their circadian system. • Progressively set an alarm to get up earlier and expose the person to bright light in the morning. • Melatonin in the evening. • Keep a regular schedule (even on weekends!) |
|
|
Side note: what is systematic hypertension? |
Systemic Hypertension is high blood pressure in the systemic arteries
|