Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
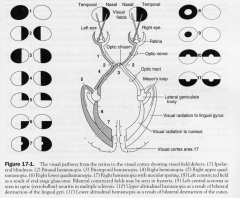
Visual Pathway
|
1. ganglion cells of retina
2. optic nerve 3. Optic chiasm 4. Optic tract 5. LGN 6. Geniculocalcarine tract (visual radiation) 7. Visual cortex |
|
|
Ganglion cells of retina
|
- form optic nerve
- nasal contralateral LGN - temporal hemiretina ipsilateral LGN |
|
|
Optic Nerve
|
TRANSECTION: causes ipsilateral blindness with no direct pupillary light reflex
|
|
|
Optic Chiasm
|
- decussation of the nasal hemiretinas & non-crossing temporal hemiretinas
- project fibres to suprachiasmatic nucleus of the hypothalamus 1. midsagittal transection or pressure (often pituitary tumour) 2. Bilateral lateral compression (ofteen due to calcified ICAs |
|
|
Optic Tract
|
projects to ipsilateral LGN, pretectal nuclei, superior colliculus
|
|
|
LGN
|
6 layered
1,4,6 recieved crossed fibres 2,3,5 uncrossed - LGN recieved input also from layer VI striate cortex (BA 17). PROJECTS through optic radiation to layer IV of 1o visual cortex |
|
|
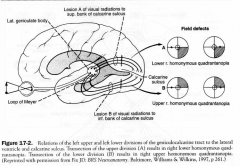
Optic Radiation (Geniculocalcarine tract)
|
have 2 divisions
1. UPPER division; to upper banks of calcarine (cuneus) represents superior retinal quadrants - lesion of both sides causes an lower altitudinopia 2. LOWER division; loops from LGN anteriorly (meyer's loop) then posteriorly to terminate in the lower calcarine sulcus, the lingual gyrus. Input from lower retinal quadrants |
|
|
Visual Cortex
|
BA 17
- has a retinotopic organsiation 1. posterior area recieves macular input (central vision) 2. Intermediate area; paramacular input (peripheral input) 3. anterior area receives monocular input |
|
|
Pupillary Light Reflex
|
1. afferent CNII
2. Efferent CNIII A. ganglion cells of retina project bilaterally to pretectal nuclei B. Pretectal nucleus of midbrain project via posterior commissure crossed and uncrossed fibres to EWN C. EWN preganglionic PS neurons to ciliary ganglion D. Ciliary ganglion- postganglionic PS fibres innervate sphincter muscles of iris |
|
|
Pupillary Dilation Pathway
|
1. Hypothalamus neurons of paraventricular nucleus project directly to the ciliospinal center (T1-2) of the intermediolateral cell column of the spinal cord
2. Cliocpinal center of Budge projects preganglionic sympathetic fibres through sympathetic trunk to superior cervical ganglion 3. Superior cervical ganglion projects postgang, through perivascualr plexus of the carotid system to the dilator muscle of the iris. The fibres pass through the tympaic cavity, cavernous sinus and superior orbital fissure. |
|
|
The near reflex & Acommodation Pathway
|
A. cotical visual pathways from BA 17 tp BA 19 (assoc. cortex)
B. BA 19 projects through corticotectal tract to superior colliculus & pretectal nucleus C. these 2 then project to CNIII complex involving 1. rostral EWN, pupil constriction 2. caudal EWN, contraction of ciliary muscles (INC. refreactive lens power) 3. Medial rectus subnucleus mediates convergence |
|
|
Ciliary Muscles and Suspensory Ligaments
|
because the ciliary muscle is a sphincter, when it contracts it gets pulled closer to the pupil and thus relaxes the suspensory ligmanets and allows the lens to take its natural shape
|
|
|
Cortical & Subcortical Centers for Ocular Motility
|
A. frontal eye fields
B. Occipital eye fields C. Subcortical centre for lateral conjugate gaze D. Subcortical center fro vertical conjugate gaze |
|
|
Frontal Eye Fields
|
A. frontal eye fields= post. part of middle frontal gyrus (BA 8). regulates Saccadic eye movements
STIMULATION: causes contralateral deviation of the eyes (away form the lesion) DESTRUCTION: causes transient ipsilateral conjugate deviation of the eyes |
|
|
Occipital eye fields
|
BA 18,19
- for involuntary smooth pursuit & tracking movements - Stimulation causes contralateral conjugate deviation |
|
|
Subcortical centre for lateral conjugate gaze
|
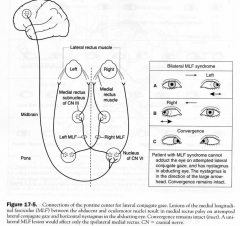
in abducent nucleus of pons
INPUT: contralateral frontal eye field PROJECTS: to ipsilateral LR and contralateral MR via MLF |
|
|
Subcortical centre for vertical conjugate gaze
|
in midbrain @ posterior commissure
- called rostral interstitial nucleus of MLF and is assoc. with parinauds Syndrome |
|
|
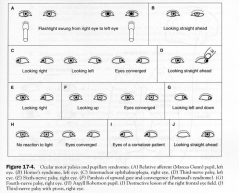
Ocular motor palsies and pupillary Syndromes
|
|
|
|
Internuclear Opthalmoplegia
|
- damage to MLF
- causes MR palsy on attempted lateral conjuagte gaze - & monocular horizontal nystagmus in the abducting eye - convergence is normal - common in MS |
|
|
One & a half syndrome
|
consists bilateral lesions of the MLF & a unilateral lesion of the abducent
|
|
|
Argyll Robertson Pupil
|
absence of miotic reaction to light (both direct & consensual) with preservation of a miotic reaction to near stimulus (accomodation-convergence)
- occurs in syphilis and diabetes |
|
|
Relative Afferent (marcus Gunn) pupil
|
lesion of optic nerve, afferent of pupil reflex
|
|
|
Transtentorial herniation
|
due to INC. supratentorial pressure (tumor, hematoma..)
1. pressure forces the parahippocampal uncus through tentorial incisure 2. the impacted uncus forces the contralateral crus cerebri aganist the tenotch) and puts pressure on the ipsilateral CNIII and post. cerebral aa. a. ipsilateral hemiparesis b. fixed and dilated pupils, ptosis & down & out eye (pressure on CNIII) c. Contralateral homonymous hemianopia (due to compression of the post. cerebral a. which irrigates the visual cortex) |
|
|
Papilledema (choked disk)
|
- non-inflammatory congestion of the optic diskdue to INC. intracranial pressure
- common cause brain tumor, subdural aematoma or hydrocephalus - MAY cause bilateral enlarged blind spots. Often assymmetric and greater on the side of the supratentorial lesion |
|
|
Adie's Pupil
|
large tonic pupil that reacts slowly to light but not to near (light-near dissociation)
- Fq seen in females with absent knee or ankle jerks |
|
|
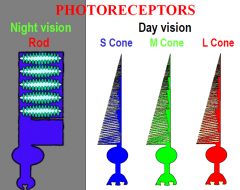
Retinal Layers
|
1. ganglion cells: (magnocellular + parvocellular)
2. Bipolar cells: link interneurons 3. Photoreceptors: light sens. RODS and CONES 4. Amacrine cells/Horizontal cells: interneurons 5. Pigment epithelium: light abs. (strongly adhere to the choriod but loosely to the photoreceptors so potential for retinal detachment) |
|
|
Location of retinal detachment
|
- pigment epithelium
|
|
|
Magnocellular
|
large cells for MOTION
|
|
|
Parvocellular
|
medium sized; deal with colour
|
|
|
Where is the one place light directly hits the photoreceptors?
|
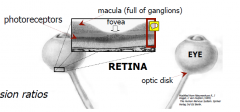
fovea centralis
|
|
|
Macula Lutea
|
area full of ganglion cells that have been pushed away from the fovea centralis
|
|
|
Macular degeneration
|
the central retina degenerates first so DEVASTING effects
unlike glaucoma where the periphery is first to go |
|
|
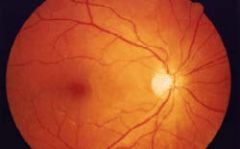
View through opthalmoscope
|
|
|
|
LGN Functions
|
• 3 BIG jobs
(1) STREAMS: what function? Magn and parvo (2) TOPOGRAPHY: where located? MAP (3) LATERALITY: which eye? • each layer driven by one or other eye - ipsilateral/contralateral inputs each LG maps the contralateral visual field (so the right picture ends up on the contralateral brain all together) |
|
|
LGN Organistion
|

inferior retina - lateral LG
superior retina - medial LG central retina - caudal LG peripheral retina - rostral LG green= contralateral red= ipsilateral |
|
|
Primary Visual Cortex
|
• banks of calcarine sulcus (band of Gennari)
• faithful projection from LG (same but different) - topography - streams - register inferior retina - inf bank V1 superior retina - sup bank V1 central retina - caudal V1 peripheral retina - rostral V1 |
|
|
NON-IMAGE FORMING PATHWAY
|
- unconscious vision and other details
Suprachiasmatic (Sch) - time-keeper (circadian) Pretectum (Pre) - pupillary reflex (II,III) Superior Colliculus (SCol) - attention, avoidance Pulvinar (Pul) - attention, integration (see, touch, hear) Secondary Visual Cortex (V2-V5) - orientation, colour, motion (adds a little more visual detail) |
|
|
Visual Cortical Functions
|
V5 - motion detection: a life in photographs
V5a - face recognition: facial agnosia V4 - colour, colour edges: colour blind V2,V3 - orientation V1 - conscious vision, topography: blindsight (some residual vision) |
|
|
Phtotoreceptors
|
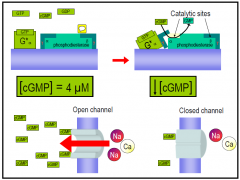
light shuts down cation conduction
|
|
|
Rod Cell Functioning
|
high cGMP in the dark (inward Na & Ca) and countered by K thus called the dark current
- depolarised photoreceptr releases glutamate - depolarisation around -40mV light closes the membrane cGMP channels, however the outwards K is still there, thus hyperpolarisation, thus realising less glutamate |
|
|
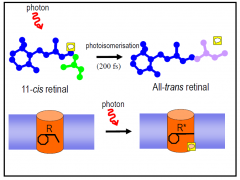
Rhodopsin
|
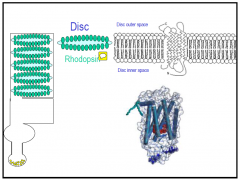
protein highly expressed in outer membrane...
-7TMD (like a GPCR) - protein part syn by golgi body of cell - VitA part - pigment eplithilium, provides retinal the photosensitve part of the retina |
|
|
Photon effect on the retinal...
|
|
|
|
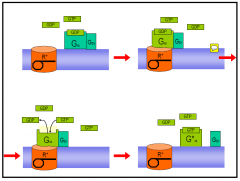
Step 1
|
|
|
|
Step 2
|
AMPLIFICATION: one photon to one rodopsin, then this interacts with many G-proteins, then it will act to many cGMP decreasing its conc.
|
|
|
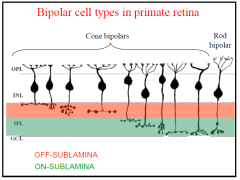
Bipolar Cells
|
|
|
|
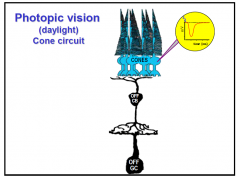
Cone vision
|
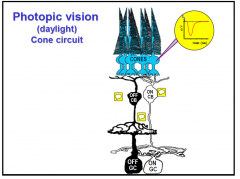
aka day light
OFF_ respond with hyperpolarisation ON_ respond with depolarisation then the glutamate released has different effects depending by whom its released |
|
|
Cone ON
|
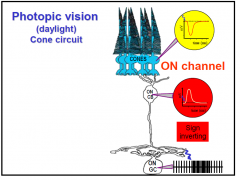
mGluR6
|
|
|
Cone OFF
|
AMPA/KA receptors
|
|
|
Parallel Processing of INFO
|
ON; optimised to INC. in intensity light
OFF: for dec. in light intesity and they both work to allow better discrimination PARALLEL processing of info; 2 different channels carring info separately Every single point in the retina hit by a light source is covered by every different physiological type of ganglion cell. Thus, each point is simultaneously analysed with regards to its contrast, colour, movement as well as other characteristics. Parallel processing of visual information starts in the retina |
|
|
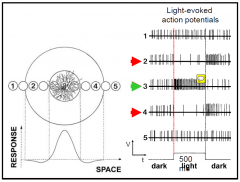
Types of Ganglion cells
|
•Local contrast detectors
•Direction selective neurons •Local Edge Detectors and Orientation Detectors •Fast motion detectors •Luminosity Detectors ("tonic units") |
|
|
intrinsically photosensitive Retinal Ganglion Cells
|
express melaopcin (express light irrespective of the photoreceptors)
- they have their own photpigment making them sens. to light so photoreceptors arent the only light sens cell in the eye •Encodes ambient light levels •Sets the biological clock •Regulates activity and melatonin levels •Adjusts pupil diameter. so this is important that people that are blind still have connections with the SCN (suprachiastmaitic nucleus) and they go free running no longer sync with the external envirnoment |
|
|
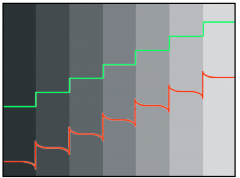
visual illusion; maach bands
- 8 uniform vertical strips of grey, however when u look at them the left edge looks lighter than the right edge - because our eyes are optimised to extract info about contrast so it enhance the contrast at the edges (lateral inhibition - that occurs at the retina) |
|
|
Zone of Inhibition
|
increase in activity when close and decrease when adjacent and nothing when far away (this is the receptive fields (excitatory center, with an inhbitory surround- anatgonist functions)
|
|
|
Function of horizontal cells
|
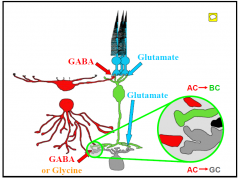
horizontal cells use inhibtory NT to modulate inhibotry stuff along the pathway
- important in things like inhibition zone and contrast definition |