![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
22 Cards in this Set
- Front
- Back
|
Calculate the Partial Pressue of O2 in inspired room air at sea level |
PiO2 = FiO2 x (Patm-PH2O) = 0.21 x (760 – 47 = 713) = 150mmHg Remember that water vapor "takes up room" in inspired air, usually 47mmHg of PP |
|
|
Rule of thumb for how much supplemental oxygen contributes to FiO2 |
Every additional L/min of100% O2 flow is about an extra 4% of O2 over room air aka 4L/min of 100% O2 byNC is about 21% + ~16% = ~37% O2 in air being breathed. In this example, PiO2 would = 0.37 x (760-47 =713) = ~264mmHg (instead of 150mmHg on normal room air) |
|
|
What is hyper/hypopnea? |
Increase or decrease in Tidal Volume (normal is ~500mL/breath) |
|
|
Formula for minute ventilation |

|
|
|
Normal amount of anatomical dead space
|
~150ml in adult, so with 500ml tidal volume there is normall ~350ml of inhaled air that reaches alveoli |
|
|
Difference between anatomical and physiological dead space |
Anatomical dead space is composed of parts of the respiratory tract that do not normally participate in gas exchange. Physiological dead space is composed of damaged parts of lung that can no longer participate in gas exchange because of pathology Normally little to no physiological dead space, presence indicates pathology |
|
|
What do central chemoreceptors measure, where are they located, and describe the mechanism of sensing? |
Central chemoreceptors are located in the brain, they measure the PaCO2 and adjust respiration to keep PaCO2 within normal limits. CO2 in blood crosses BBB and forms bicarbonate which liberates protons to drop pH, central chemoreceptors actually measure the CSF pH as a proxy for PaCO2 |
|
|
What do peripheral chemoreceptors measure, where are they located? |
Peripheral chemoreceptors measure PaO2, blood pH, and PaCO2. They are located on carotid bodies and aortic bodies Respond to PaO2 <60mHg |
|
|
Which type of chemoreceptor is more sensitive to PaCO2? |
Central chemoreceptors |
|
|
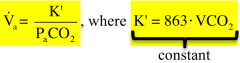
Formula for alveolar ventilation rate |
|
|
|
Normal range of PaCO2 |
Normal PaCO2 = 37 - 42mmHg (In acutely ill patients the TREND is often more important than the actual value) |
|
|
Normal PaO2 |
Normal PaO2 = 75-105mmHg (In acutely ill patients the TREND is often more important than the actual value) |
|
|
Dx & Etiology of Alveolar hyperventilation |
Dx by hypocapnia (PaCO2 < 37mmHg) ALWAYS due to increase respiratory drive, either increase in Tidal Volume or RR (drugs, anxiety, exercise, compensation for acidosis, etc) |
|
|
Dx & Etiologies of Alveolar hypoventilation |
Dx by hypercapnia (PaCO2 > 42mmHg) Four main etiologies: 1) Decreased drive/effort from CNS depression or drugs 2) Neuromuscular disease 3) Spinal/chest wall abnormalities 4) Fatigue |
|
|
Acute vs Chronic Hypercapnic Respiratory Failure |
PaCO2 high in both cases (>50mmHg) Acute: kidneys have not been able to compensate for acidosis, pH will be low (<7.3) Chronic: kidneys have compensated for acidosis by releasing bicarbonate, pH will be ~7.4 Carbonic acid levels can confirm, normal CA is 24, elevated CA indicates kidney compensation |
|
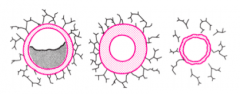
Three mechanisms for changing airway radius |
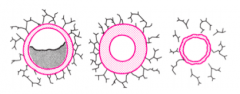
1) Intraluminal obstruction (secretions, foreign bodies) 2) Intramural obstruction (bronchoconstriction, inflammation) 3) Extraluminal (breakdown of structure in emphysema causing loss of radial traction) |
|
|
Formula for compliance |

|
|
|
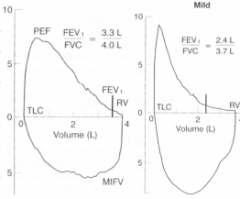
Cutoff for FEV1/FVC ratio to diagnose airflow obstruction |
If FEV1/FVC <70% of predicted value for age/gender/height |
|
|
PFT graph for mild airflow obstruction
|
|
|
|
PFT graphs for fixed and variable airflow obstruction |
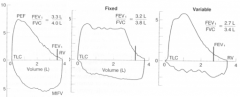
|
|
|
What test to you need to diagnose restrictive lung disease |
You need to measure total lung volume to diagnose. A PFT exam (spirometry) showing decrease FVC (forced vital capacity) is suggestive of restrictive lung disease but other etiologies can cause similar result so you cannot conclude this from PFT alone |
|
|
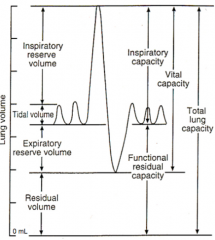
Summary of Lung Volumes |
|