![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
7 Cards in this Set
- Front
- Back

|
This shows the aortic valve which has fused commisures and calcific nodules. . This would lead to stenosis, and pulmonary oedema, orthopnoea, and syncope. Changes like this are typical of rheumatic heart disease, which affects the mitral valve 100% of the time, then aortic, then tricuspid. |
|
|
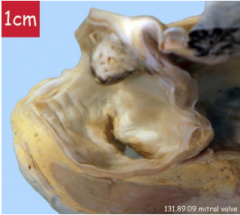
A fished mouth deformity of the mitral valve is visible- thickened edges from fibrosis. Would cause regurgitation and stenosis, leading to built up pressure, and a dilated atrium. A large mural thrombus in the LA from blood stasis. Treated with prophalactic AB's, and a MV repair. |
|

|
There is a large vegetation present on the aortic valve likely infective endocarditis- as a result of staph a, or strep viridians. The mitral valve appears normal. Micro-emboli can break off from here and go to the coronary arteries and body! |
|

|
Centrally you can see a bicuspid aortic valve. This is prone to distrophic calcifications (as seen here), and resulting stenosis. congenital change where 2 valve leaflets have to work harder than 3, so a higher risk of calcification with age, thickening and AS. |
|

|
Very thickened LV wall, giving a narrowed lumen. Pale areas within the wall are typical of ischemia- interstitial fibrosis. Heart failure, so pulmonary oedema, murmurs, syncope, endocarditis, and sudden heart failure, aortic dissection and MI are all possible outcomes. |
|

|
Aortic valve on the left, mitral valve on the right. Vegetations are present on the aortic valve, and there is possible thickening of the leaflets. Small microthrombi are visible on the mitral valve, and there are shortened thickened chordae tendinae beneath the mitral valve. The left ventricle is dilated- hypertrophy and dilation from aortic regurgitation. The patient had a history of rheumatic heart disease, but was feeling feverish and unwell for the month leading up to death- likely infective endocarditis. |
|

|
The kidney is ischaemic (white) with dark areas of granulation tissue, in attempt to repair. Possibly died from thrombo-embolism causing ischaemic kidneys (AKI). |