Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
Digitalis:
MOA Side Effects Signs of Toxicity Toxicity Treatment |
Increases vagal tone to stimulate AV node. ( RICK OF AV BLOCK)
AE: Fatigue, blurry vision, changes in color perception, nausea, vomiting, diarrhea Bradycardia from inc'd AV nodal block, junctional escape beats-->v tach/fib Tox: Hyperkalemia due to action on Na/K ATPase Tox tx: Activated charcoal if suicide attempt (digitalis OD) Insulin, kayexalate, hemodialysis to manage serum K+ Digoxin-specific Ab's |
|
|
Uretrhritis
Conjunctivitis Arthritis Diagnosis Pathophys Additional Symptom |
Reiter syndrome (reactive arthritis, ReA)
ReA = autoimmune reaction initiated by infecting pathogen (Chlamydia--urethritis, or Salmonella, Shigella, Campylobacter, Yersinia--enteritis) 20% develop sacroiliitis |
|
|
Arthritis
HLA-B27 |
Reiter Syndrome
|
|
|
How would initiating niacin affect diabetic medication regimen?
|
Niacin can cause insulin resistance and often necessitates increase in DM medications.
|
|
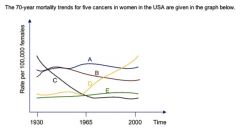
Label
|

A) Breast Cancer (mortality has decreased over the years)
B) Colon Cancer (mortality relatively stable after some decrease) C) Stomach Cancer (once very common, now very uncommon) D) Lung Cancer (once uncommon, now leading cause of cancer mortality in women) E) Ovarian cancer |
|
|
Define splitting.
|
Unconscious belief that people are either wholly good or wholly bad.
Same person can be either good or bad at different times, as can groups of people. Hallmark of borderline PD. |
|
|
This cell mediates delayed type hypersensitivity.
|
Th1
|
|
|
This cell mediates immunoglobulin class switching.
|
Th2
|
|
|
This cell initiates antibody response.
|
Th2
|
|
|
Under what conditions would a Naive CD4+ T-Cell (Th0) become a Th1 cell? Th2?
|
If macrophage presents antigen to Th0, macrophage will release IL-12 which will stimulate differentiation into Th1.
THIS CAN ALSO BE ACCOMPLISHED BY IFN-GAMMA If other APC presents antigen, IL-4 will be released by APC-->differentiation into Th2 subset. |
|
|
CD Markers for Th0 cells.
|
CD3
CD4 (in addition to T cell receptor) |
|
|
What cell-cell interactions are required for activation of Th0 cells?
|
MHC-II interaction with TCR and CD4 proteins
CD3 transmits signal to cell's interior |
|
|
How would a deficiency in IL-12 receptors affect T cells?
|
Would make T-cells unable to differentiate into Th1 subpopulation. Then can't make IFN-gamma to activate macs.
Wouldn't be able to mount attack against delayed hypersens rxns against intracell organisms such as mycobacteria. Thus will suffer from severe mycobacterial infections and need IFN-gamma. |
|
|
Neonate
Sacral, lumbar spine agenesis Flaccid Paralysis Urinary incontinence Diagnosis Pathophys |
Caudal regression syndrome
Due to poorly controlled maternal DM |
|
|
Where is the chemoreceptor trigger zone (emesis) located?
|
Dorsal Medulla (near fourth ventricle)
|
|
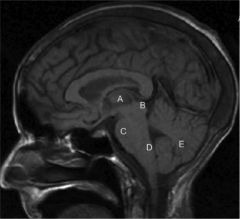
Label
Include third and fourth ventricles. |
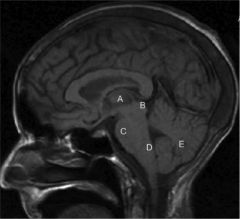
A) Thalamus (coordinates sensory, motor systems)
B ) Dorsal midbrain (superior, inferior colliculi; third ventricle just dorsal to here) C) Ventral pons D) Medulla (just caudal to 4th ventricle) E) Cerebellum |
|
|
Direct vs Indirect Inguinal Hernias:
Which are more common? Location Site of protrusion |
Indirect more common
Direct: Located medially to inferior epigastric vessels Protrude through anterior abdominal wall via Hesselbach triangle; NEVER protrude into scrotum Indirect: Located laterally to inferior epigastric vessels. Protrude through deep inguinal ring, can continue into scrotum and felt in inguinal canal (in scrotum). |
|
|
Varicoceles:
Where do they mostly occur? Why? |
On left
Left gonadal (testicular or ovarian) drains into left renal vein, commonly leading to left-sided varicoceles in males with obstructions of left renal vein. The right gonadal vein drains directly into inferior vena cava. |
|
|
6-month old
Hypoglycemia Hypertriglyercidemia Ketoacidosis Hepatomegaly Diagnosis Pathophys |
Cori Disease--debranching enzyme deficiency.
Alpha-1,6-glucosidic branch points can't be degraded so small chain dextrin-like material accumulates in cytosol of hepatocytes. |
|
|
What EKG changes would you expect to see with WPW?
|
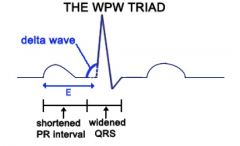
Shortened PR interval
Delta wave at start of QRS Widened QRS |
|
|
Describe physiologic compensatory mechanisms which exacerbate CHF.
|
Dec'd Cardiac Output
-->Dec'd renal perfusion -->Dec'd stretch of glomerular afferent arterioles -->Renin -->Ag I-->Ag II via ACE Ag II: Sodium retention, aldosterone release, VASOCONSTRICTION (increasing preload and afterload) Baroreceptors detect dec'd perfusion-->Inc'd sympathetic tone (inc'd HR and contractility, inc'd arterial resistance; thus, increasing afterload) |
|
|
Treatment for acute leukemia
Oliguria Elevated Creatinine Uric Acid Cystals Diagnosis Pathophys Treatment |
Tumor lysis syndrome--lyris of tumor cells cause intracellular ions (K+, P, Uric Acid) to be released in serum.
Uric acid soluble at physiologic pH, but precipitates in normally ACIDIC environment of DISTAL TUBULES AND COLLECTING DUCT. Tx: Urine alkalinization and hydration |
|
|
What determines what particles penetrate the nephron:
-with regard to size? -with regard to charge? |
Size: GBM and slit diaphragms
Charge: Negatively charged anions (heparan sulfate, proteoglycans0 on endothelial cells and GM--repel negatively charged molecules such as albumin |
|
|
Why doesn't albumin pass through the nephron?
|
Albumin is small enough to fit through pores in GBM; barrier to its excretion is mostly by charge selectivity.
|
|
|
Minimal Change Disease:
Highly or poorly selective? Why? |
Highly selective--mostly low-molecular weight proteins, such as albumin and transferrin, are excreted.
|
|
|
Bounding femoral pulses
Head-bobbing |
Aortic regurgitation
|
|
|
Describe the steps of heme synthesis.
Which would be affected by lead poisoning? What would be elevated? |

|
|
|
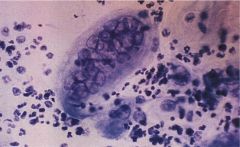
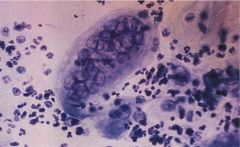
Oval cells resembling lymphocytes
Chromogranin positive Secretory granules in cytoplasm Diagnosis Origin |
Small cell carcinoma--CORRELATED WITH SMOKING
Arises from primitive cells of basal layer of bronchial epithelium |
|
|
Xanthomas
Lack ApoE3, ApoE4 Diagnosis Pathophys |
Familial dysbetalipoproteinemia
Without ApoE3/4, liver can't efficiently remove chylomicrons and VLDL remnants from circulation, causing accumulation in serum and elevations in cholesterol and TG levels. |
|
|
List the most important apolipoproteins and their functions.
|
ApoA-I: LCAT activation (cholesterol esterification)
ApoB-48: Chylomicron assembly, secretion by intestine ApoB-100: LDL particle uptake by extrahepatic cells ApoC-II: Lipoprotein lipase activaiton ApoE-3/4: VLDL and chylomicron remnant uptake by liver cells |
|
|
5 year-old female
Erythema, Scaling, Hyperpigmentation on sun-exposed areas Rapidly enlarging nevi on hands Diagnosis Pathophys |
Xeroderma pigmentosum--dec'd ability to repair DNA following damage by UV light (requires excision)
|
|
|
Tetanus:
Species name Describe disease progression |
Clostridium tetani (spores! anaerobe!)
Toxin released at wound-->travels retrograde on motor neurons into spinal cord-->inhibits inhibitory interneurons and upregulates firing of primary motor neurons |
|
|
Headache
Photosensitivity Nausea, vomiting Gram-negative kidney bean-shaped cocci Diagnosis Pathophys |
Infection with N. meningitidis
Lipooligosaccharide of outer membrane is responsible for toxic effects (also associated with mortality) LOS causes sepsis by induction of systemic inflammatory response via TNF-alpha, IL-1, IL-6, IL-8 due to LOS interaction with TLR4. Beware of Waterhouse-Friderichsen (adrenal cortical hemorrhage) |
|
|
Ring-enhancing lesions in both cerebral hemispheres
AIDS patient Diagnosis Pathophys Treatment |
Toxoplasmosis
Toxoplasma gondii = obligate intracellular protozoan; cat = definitive host Can develop encephalitis with multiple necrotizing brain lesions Tx: Pyrimethamine, sulfadiazine |
|
|
What are the two most common causes of focal brain lesions in HIV-positive patients?
Etiology of both? |
1) Toxoplasmosis due to cat poop contaminated food/water
2) Primary CNS lymphoma composed of B-lymphocytes, likely secondary to EBV |
|
|
Tzanck preparation
Presence of multinucleated giant cells with some intranuclear inclusions Suggestive of HSV or VZV |
|
|
5 year-old male
Fever Vesiculoulcerative gingivostomatitis Cervical LAD Diagnosis |
Primary infection with HSV-1
|
|
|
How does primary infection with HSV-1 differ in presentation from reactivation of a latent HSV infection?
|
Primary: Fever, vesiculoulcerative gingivostomatitis, cervical LAD
Latent: If in trigeminal ganglia-->perioral blisters or "cold sores" |
|

|
Dermatomyositis
|
|
|
What is a heliotrope rash?
|
Rash on upper eyelids (think dermatomyositis)
|
|
|
Dermatomyositis:
Presentation Antibodies |
Gottron papules (flat-topped violaceous papules present over joints of fingers)
Heliotrope rash (on upper eyelids) Anti-nuclear (nonspecific) Anti-Jo1 (specific) |
|
|
Benzodiazepines:
MOA Side Effects Shortest acting Medium acting Longest acting Which are most addictive? |
Bind GABA-a receptors and enhance inhibitory effect of GABA
Can be used to treat insomnia (= hypnotics), panic/anxiety disorders (=anxiolytics), anticonvulsants (seizures assocd w/EtOH withdrawal) AE: Daytime drowsiness, ataxia (RISK OF FALLING) Shortest acting: Alprazolam (highest risk of addiction) Medium: Lorazepam Longest acting: Flurazepam (SEVERE daytime drowsiness; lower risk of addiction) |
|
|
These drugs block iodide absorption by the thyroid via competitive inhibition.
|
Perchlorate
Pertechnetate |
|
|
These drugs decease the formation of thyroid hormones by inhibiting thyroid peroxidase.
|
Methimazole
Propylthiouracil (PTU) |
|
|
This drug inhibits the synthesis and release of thyroid hormones.
|
Iodide
|
|
|
What is the action of thyroid peroxidase?
|
I- -->I0 (necessary to form thyroid hormone)
|
|
|
What cells exhibit tight junctions?
|
Apices of glandular cells
|
|
|
What cells exhibit hemidesmosomes?
|
Basal surface of keratinocytes in stratified squamous epithelium
Attaches it to basal lamina |
|
|
What cells exhibit desmosomes?
|
Stratified squamous epithelium--contributes to structural cohesiveness of tissues subject to mechanical stress
|
|
|
Equilibration of O2 in a normal patient at rest is _______-limited.
Why? When is this not true? |
Perfusion-limited, bc equilibration occurs before leaving capillary
Not true in emphysema, pulmonary fibrosis, exercise--then becomes diffusion-limited |
|
|
Lyme disease:
Early vs Late Stages (presentation) Treatment |
Early: flu-like syx, erythema migrans
(a second stage may involve AV block and Bell's palsy0 Chronic: Asymmetric large joint arthritis, encephalopathy Tx: Doxycyline OR PCN-type abx (ex: ceftriaxone) Note: Borrelia burgdorferi ~ syphilis bc it's a spirochetal infection |
|
|
MTX AEs
|
Remember: MTX works by inhibiting DHF reductase
Stomatitis (painful mouth ulcers) Hepatotoxicity (hepatitis, fibrosis, cirrhosis) Myelosuppression CONTRAINDICATED IN PREGNANCY |
|
|
Cola-colored urine
Facial edema Recent outbreak of skin infection Diagnosis |
Post-strep GN
|
|
|
What is the most important prognostic factor in poststreptococcal glomerulonephritis?
|
Age
95% of affected children, but ONLY 60% OF AFFECTED ADULTS, recover completely. |
|
|
Needle-shaped, negatively birefrignent crystals
|
Gout crystals
|
|
|
Acute pain, swelling of first metatarsophalangeal joint
Needle spirate shows needle-shaped, negatively birefringent crystals Diagnosis Treatment Treatment MOA, AEs |
Acute gouty arthritis
Tx: Colchicine MOA: Binds intracellular tubulin and prevents its polymerization into microtubules (INHIBITS MT FORMATION) in leukocytes-->reduces nphil chemotaxis in sites with uric acid crystal deposition AE: nausea, vomiting (GI mucosa affected by inhibition of tubulin polymerization) |
|
|
Mediastinal widening
Diastolic murmur over left sternal border Serum FTA-ABS positive Diagnosis Pathophys |
Aortic regurgitation + mediastinal widening = AORTIC ANEURYSM
FTA-ABS positive = syphilis Thus, must be tertiary syphilis: -Vasa vasorum endarteritis and obliteration-->inflammation and weakening of adventitia -->can extend to dilate aortic valve |
|
|
Pleural thickening with calcifications on lower lung fields and diaphragm
|
Asbestosis
localization to mid-lung zones and diaphragm = hallmark |
|
|
Nodular densities and eggshell calcifications on hilar nodes
|
Silicosis
|
|
|
Waxing and waning lymphadenopathy
|
Follicular lymphoma (it's of B cell origin BTW)
|
|
|
Under what specific histologic conditions does a tumor become invasive?
|
1) Detachment from surrounding cells via down-regulation of E-cadherins
2) Ability of detached cells to adhere to BM's through inc'd laminin and other adhesion molecules. 3) Invasion via secretion of METALLOPROTEINASES (normally involved in tissue remodeling) |
|
|
What is papilledema? What causes it?
|
Optic disc swelling due to inc'd intracranial pressure
|
|
|
Papilledema
Dry Skin Hepatosplenomegaly No intracranial mass |
Vitamin A overuse
|