Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
|
Negative predictive value
|
-probability of being free of a disease if the test result is negative
-NPV varies with the PRE-TEST probability of patient having disease -patient with a high probability of having a disease will have a low NPV with a negative test, but a patient with a low probability of having a disease will have a high NPV with a negative test |
|
DiGeorge syndrome
|
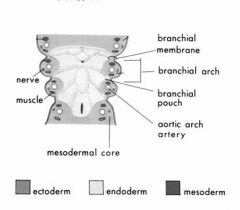
-Due to mal-development of the THIRD AND FOURTH BRANCHIAL (PHARYNGEAL) POUCHES due to deletion on chromosome 22
-clinical associations include absence of thymic shadow on neonatal x-ray, hypocalcemic tetany from absence of parathyroids, cleft palate, mandibular deformity, low-set ears, aortic arch abnormalities |
|
|
Renal angiomyolipoma
|
-renal angiomyolipoma = benign tumor composed of blood vessels, smooth muscle, and fat
-these tumors can be seen with abdominal CT scan, as density of fat is less than that of water -associated with TUBEROUS SCLEROSIS, an autosomal dominant condition -tuberous sclerosis is characterized by cortical tubers (region of brain that develops abnormally) and sub-ependymal hamartomas in the brain, with consequent seizures and mental retardation -cardiac rhabdomyomas, facial angiofibromas, and leaf-shaped patches of skin that lack pigment (ASH-LEAF PATCHES) can also occur |
|
|
C peptide
|
-C peptide is formed from pro-insulin in the pancreatic beta-cell Golgi apparatus
-within Golgi apparatus, converses cleave proinsulin into insulin, C peptide, and two pairs of basic amino acids -C peptide is packaged along with insulin in the islet cell secretory granules, and secreted in equimolar concentrations with insulin |
|
|
Transference (psych)
|
-unconscious shifting of emotions or desires associated with one person (e.g., sibling , parent, spouse) to another (physician, therapist).
-this can be positive or negative -transference reactions often arise from childhood parent-child relationships |
|
|
Acting out
|
-immature defense mechanism – unconscious wishes or impulses are expressed through actions (like temper tantrums)
|
|
|
Displacement
|
-displacement is shifting feelings or conflicts from one situation or person to another seen as safer and less distressing
-ex: a medical resident belittled by his attending on rounds who later angrily berates a medical student |
|
|
Projection
|
-projection involves attributing one's own unacceptable thoughts and feelings to another person
-ex: patient accuses therapist of having sexual interest in him when, in fact, the patient is attracted to the therapist |
|
|
Mallory-Weiss tear
|
-tear in gastric MUCOSA near the GE junction
-typically result of repetitive forceful vomiting, which can lead to metabolic alkalosis -may present with vomiting/retching, hematemesis, and epigastric pain -bleeding from submucosal arterial or venous plexus |
|
|
Boerhaave syndrome
|
-Boehaave syndrome = esophageal TRANSMURAL TEAR
-also caused by forceful coming (increased intragastric pressure) -ESOPHAGEAL AIR/FLUID LEAKS INTO MEDIASTINUM AND PLEURA -presents with vomiting/retching, chest and upper abdominal pain --> fever, dyspnea, and septic shock - |
|
|
Ethanol intoxication – metabolic effects
|

-ethanol intoxication can cause lactic acidosis, which produces a HIGH ANION GAP metabolic acidosis
|
|
|
Normal anion gap metabolic acidosis
|

-normal anion gap metabolic acidosis is usually caused by loss of bicarbonate, which can occur with PROLONGED DIARRHEA
-vs. recurrent vomiting causes metabolic alkalosis, not acidosis |
|
|
Respiratory acidosis
|
-respiratory acidosis usually seen in patients with chronic obstructive pulmonary disease (COPD) or central nervous system depression (e.g., narcotic overdose)
|
|
|
Respiratory alkalosis
|
-respiratory alkalosis occurs with hyperventilation
-seen with panic attacks, and pulmonary emboli |
|
Congenital adrenal hyperplasia
|
-21-hydroxylase deficiency is the most common form of congenital adrenal hyperplasia
-affected female infants present at birth ambiguous (virilized) genitalia -vs. male infants have normal genitalia, and present later with SALT-WASTING or precocious puberty -a high serum level of 17-hydroxyprogesterone is diagnostic |
|
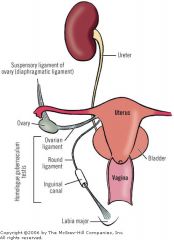
Suspensory ligament of ovary
|
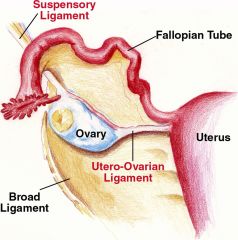
-the nerves and vessels supplying the ovary are delivered through the SUSPENSORY LIGAMENT OF THE OVARY
-so in removal of an ovarian mass, a surgeon should ligate the suspensory ligament to avoid excessive bleeding |
|
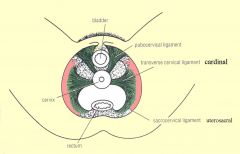
Transverse cervical ligament
|
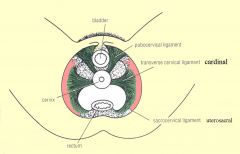
-transverse cervical ligament, aka cardnial ligament, extends from cervix and lateral fornix of vagina to lateral pelvic walls
-the uterine artery courses though the transverse cervical ligament and must be ligated during radical hysterectomy |
|
|
Meiosis of oocytes
|
-primary oocytes are completely developed in female embryos by fifth month of gestation, at which point they are ARRESTED IN PROPHASE OF MEISOSIS 1
-ovarian cycle hormones stimulate primary oocyte to resume differentiation -prior to fertilization, secondary oocytes are arrested in METAPHASE of MEIOSIS II |
|
|
Methemoglobinemia
-presentation: nitrite exposure, with anxiety, weakness, dyspnea, headache -cyanosis not corrected by oxygen supplementation |
-methemoglobinemia causes dusky discoloration to the skin (similar to cyanosis)
-since methemoglobin can't carry oxygen, a state of functional anemia is induced -blood partial pressure of O2, however, will be unchanged in this condition because oxygen's partial pressure is a measure of O2 dissolved in the plasma, and is NOT related to hemoglobin function -nitrites bind hemoglobin and keep iron in its Fe3+ form, so that it cannot carry oxygen -Hb saturation is also decreased in CO poisoning, as CO competes with O2 --but still, Po2 of blood (dissolved oxygen) would be NORMAL |
|
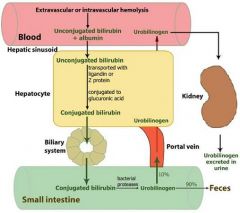
Bilirubin metabolism
|
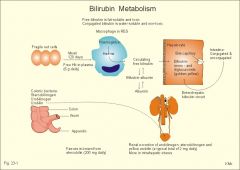
-liver takes up indirect/unconjugated bilirubin through a passive process – secretes direct/conjugated bilirubin through an ACTIVE process
-unconjugated bilirubin is virtually insoluble in water at physiologic pH – tightly complexed to serum albumin while in the circulation --so UNCONJUGATED/INDIRECT BILIRUBIN CANNOT BE EXCRETED IN URINE< EVEN WHEN BLOOD LEVELS ARE HIGH -vs. conjugated bilirubin is water-soluble, non-toxic, and only loosely bound to albumin – thus can be excreted freely in the urine |