Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
96 Cards in this Set
- Front
- Back
|
Penetrating injury at left sternal border in 4th intercostal space will likely injure __________.
|
RV
|
|
|
What comprises the majority of the anterior surface of the heart?
|
RV
|
|
|
When would a stab wound likely hit the left ventricle?
|
4th intercostal space, midclavicular line after passing through bulk of lung
|
|
|
When would a stab wound likely hit the pulmonary trunk?
|
Second intercostal space, left sternal border
|
|
|
When does hypospadias arise?
Ventral or dorsal? |
Incomplete fusion of urethral (urogenital) folds
Hypospadias is ventral |
|
|
When does epispadias arise?
Ventral or dosral? |
Faulty positioning of genital tubercle-->epispadias
Dorsal |
|
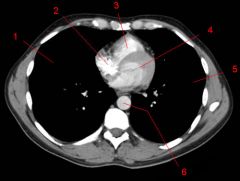
Label
|
1. Right lung
2. RA 3. RV 4. LV 5. Left lung 6. Aorta (note: space between aorta and LA (south of where 4 points) = esophagus) |
|
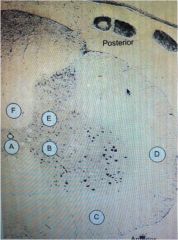
Label and describe
|
A-Ventral White Commissure; decussation, transmits pain and temp sensation; destruction (syringomyelia) results in loss of temp/pain sensation in arms/hands bilaterally.
B-Ventral horn--motor neurons responsible for voluntary motor activity; can be affected by syringomyelia, result in areflexia, flaccid paralysis, fasciculaitons, atrophy of hand mm. C- Ventral spinothalamic track--light touch, pressure sensation D- Contralateral lateral funiculus; damage would cause contralateral loss of pain and temp sensation in one segment below lesion (not bilateral loss) E- Dorsal horn--receives sensory input F-Dorsal column--contains gracile and cuneate fasciculi; proprioception, vibration, tactile sensation |
|
|
Syringomyelia affects the __________ of the spine.
|
Ventral white commissure
(pain and temperature sensation of hands/arms) Cervical region! Can also destroy MNs of ventral horns-->flaccid paralysis, atrophy of intrinsic mm |
|
|
Fragile X Syndrome:
Mutation Presentation |
Inc'd numnber of CGG repeats in Familial Mental Retardation gene (FMR-1) located on X-chromosome long arm
Presents with: -macrosomia with inc'd head circumference -Large jaw, large protruding ears, long thin face, prominent forehead -Macroorchidism (enlarged teses) -Mild-to-moderate MR, language delay, bhvrl abnlts |
|
|
Male
Tall stature Gynecomastia Small testes |
Klinefelter
|
|
|
Absolute risk reduction for drug A vs standard therapy is 4%.
If incidence of pulmonary embolism with standard therapy is 6% and there are 24 pulmonary emboli in drug A group, how many total subjects are there in the drug A group? |
ARR= Event rate (control) - Event rate (treatment)
4%=6%-Event rate (treatment) Event rate (treatment) =2% Event rate (treatment) = Events/total treatment arm subjects 2%=24/total treatment arm subjects Total treatment arm subjects = 1200 |
|
|
DiGeorge Syndrome:
Embryologic pathophys |
Maldev't of third and fourth BRANCHIAL (PHARYNGEAL) POUCHES
|
|
|
Describe schizophrenia, disorganized type.
|
Too disorganized to take care of themselves or perform activities of daily living like showering, dressing, etc.
|
|
|
Describe schizophrenia, paranoid type.
|
Prominent delusions and auditory hallucinations. Often persecutory in nature.
|
|
|
Describe schizophrenia, catatonic type.
|
Disturbance of motor fn--abnl voluntary mvmts, immobility (waxy flexibility or stupor) excessive motor activity, bizarre posturing
Mutism, echolalia (repetition of word or phrase spoken by another person), echopraxia (repetitive mimicking of another person's mvmts), extreme negativism |
|
|
Describe schizophrenia, residual type.
|
Persistence of syx like emotional blunting, eccentric bhvr, loose assocns b/t episodes of active schizophrenia.
No hallucinations, delusions, disorganized speech, or catatonia. "Burned out" schizophrenics. |
|
|
Propionic acid:
How is it made? Describe its metabolism. |
Isoleucine, valine, threonine, methionine, cholesterol., odd-chain FAs-->Propionic Acid
Propionic Acid-->methylmalonic acid via BIOTIN-DEPENDENT carboxylation Isomerization of methylmalonyl CoA-->succinyl CoA-->TCA |
|
|
Describe the metabolism of phenylalanine.
|
Phenylalanine-->Tyrosine-->Fumarate-->TCA
|
|
|
Cold agglutinins:
When are they produced? Diagnostic utility? |
Produced in response to mycoplasma pneumoniae infection
Directed against antigens that are also present on surface of human RBCs Responsible for transient anemia documented in pts w/M. pneumoniae infection Also assocd w/EBV and hematologic malignancies If place test tube of pts blood in ice (with anti-coagulant), will clump! |
|
|
Rapidly progressive dementia
Myoclonic jerks Multiple vacuoles in gray matter |
Creutzfeld-Jakob Dz
|
|
|
Creutzfeld-Jakob Disease;
Pathophys Presentation |
Prion dz:
-Prior protein present in host neurons -Long incubation period, and rapidly progressive after onset of syx -Spongiform encephalopathy--vacuoles form in cytoplasm of nphils and neurons, transform into cysts -No treatment :( Presentation: rapidly progressive dementia, myoclonic jerks, multiple vacuoles in gray matter of brain (spongiform encephalopathy) |
|
|
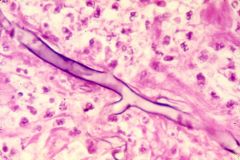
70-year old man
Bone pain Elevates serum alkaline phosphatase Haphazard cement lines of lamellar bone |
Paget's Dz:
Begins as inc'd oclast activity, followed by increase in oblast activity. Net result: inc'd bone resorption and formation of abnl bone |
|
|
Levodopa:
AEs alone AEs with carbidopa |
Alone:
CNS f/x: Anxiety, agitation because of DA Peripheral f/x: n/v (DA activates emetic center in brainstem--outside of BBB), tachyarrhythmias--extrasystoles, a fib, postural hypotn (due to peripheral conversion of levodopa to DA) With carbidopa, peripheral conversion is inhibited ; only syx seen are agitation/anxiety (which can actually be worsened bc so much of L-dopa is being converted centrally) |
|
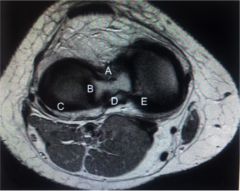
Label attachments/structures (knee)
|
A--attachment of ACL
B--attachment of lateral meniscus C--Covered by lateral meniscus D--Attachment of PCL E--Covered by medial meniscus |
|
|
Diniminished first heart sound
Apical holosytolic murmur Bibasilar lung crackles No JVD |
Holosytolic murmu-->Mitral Regurgitation
Lung crackles-->LHF |
|
|
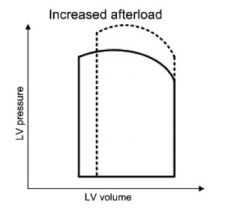
In a patient with mitral regurgitation, what would decrease the amount of blood flowing back into the LA?
How can this be achieved? |
Lower LV afterload would decrease pressure gradient driving regurgitant flow into LA. (would also increase forward stroke volume).
Achieve by arterial vasodilation |
|
|
What drug would block gastric acid secretion normally stimulated by acetylcholine, histamine, and gastrin?
|
Proton pump inhibitor!!
-prazole |
|
|
This drug blocks gastric parietal cell acetylcholine receptors.
|
Atropine
|
|
|
This drug blocks parietal cell H2 receptors.
|
Cimetidine (ranitidine, etc.)
|
|
|
Draw cardiac PV curve to show a change in afterload.
|
|
|
|
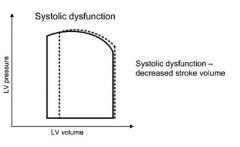
Draw a cardiac PV curve to show systolic dysfunction.
|
|
|
|
Infant
Loss of motor skills HSM Hypotonia Cherry-red macular spot Diagnosis Pathophys |
Niemann-Pick Disease
Differs from Tay-Sachs bc HSM is present; Tay-Sachs doesn't have HSM. Niemann-Pick = lipid storage disorder where lipids accumulate in spleen, liver, lung, BM, brain. Classic: Lack sphingomyelinase (degrades sphingomyelin--component of cell membrane) |
|
|
Niemann-Pick Disease:
Pathophys Presentation |
Autosomal RECESSIVE disorder char'd by deficiency of sphingomyelinase enzymes
Results in accumuln of sphingomyelin Patients present in infancy w/loss of motor skills, HSM, hypotonia, cherry red macular spot. Foamy histiocytes (accumulated sphingomyelin) Death before age 3 |
|
|
What drugs are associated with drug-induced lupus?
|
It's not HIP to have Lupus:
Hydralazine Isoniazid Procainamide |
|
|
What is cinchonism?
Side effect of what drug? |
Tinnitus, dizziness, fainting
Seen in Quinidine |
|
|
Amiodarone:
AEs |
Thyroid dz
Lung fibrosis Liver tox Blue/gray skin |
|
|
Acute acalculous cholecystitis:
What is it? Pathophys Treatment |
Acute inflammn of gallbladder in absence of gallstones
Caused by gallbladder stasis and ischemia, which cause inflammn of and injury to gallbladder wall (such as in hospitalized pts with hypotn, poor blood flow) Tx: IV broad-spectrum abx and cholecystectomy with drainage of abscess |
|
|
What is porcelain gallbladder?
Risk? |
Abdominal x-ray showing rim of Ca2+ deposits that outline the bladder
Assocd w/gallbladder carinoma |
|
|
Shrunken, fibrosed gallbladder:
Pathophys |
Chronic cholecystitis resulting form repeated mild attacks of acute cholecystitis (leads to thickening of gallbladder wall)
|
|
|
Intimal streak vs Intimal tear:
Role in aneurysm |
Major cause of aneursym (AAA specifically) is atherosclerosis
Intimal (fatty) streaks are the earliest lesion of atherosclerosis and are composed of intimal lipid-filled foam cells, which are derived from macs that have engulfed lipoproteins. These then collect in the intima through an injured, leaky endothelium. Intimal tear initiates formation of a dissecting aortic aneursym. |
|
|
rER vs sER:
Functions |
Rough ER: (ribosomes attached) snthesizes secretory, lysosomal, and integral membrane proteins
Smooth ER: steroid and phospholipid synthesis. All steroid producing cells (cells in adrenals, gonads, liver) contain well-developed SER. ACTH stimulates the cells in adrenal cortex to produce mineralocorticoids, glucocorticoids an dandrogens, all chol-derived steroid hormones. SER also involved in detox of drugs, esp in hepatocytes. |
|
|
Identify murmur.
|
Machine-like; PDA
|
|
|
Infective endocarditis after diagnosis with colon cancer:
Cause |
Bacteremia with Strep bovis (part of normal flora of colon) is assocd w/colonic cancer in ~25% of pts.
|
|
|
34-year old woman with mitral stenosis
Low-grade fevers Negative blood cultures |
Likely has suffered from acute rheumatic fever in past (which is cause of mitral stenosis), she is probably experiencing another episode of rheumatic fever
|
|
|
29 year-old male with persistent fever
Tricuspid vegetations Tricuspid regurgitation |
Right-sided endocarditis caused by S. aureus, typical of IV drug users.
|
|
|
Formula for relative risk.
|
(Dz in group A/Total group A)/(Dz in control group/Total control group)
|
|
|
Formula for odds ratio.
|
ad/bc (in 2 x 2 table)
label table as: a, b c, d |
|
|
2 year-old male
Fever Decreased oral intake Swollen gums with ulcers Enlarged, tender LAD Oral lesion demonstrates cells with intranuclear inclusions |
Herpes virus 1 infection
|
|
|
Koplik spots
|
Bluish-gray spots on buccal mucosa-->measles
|
|
|
What kind of virus is HSV?
|
Enveloped dsDNAvirus
|
|
|
Developing nation
Fulminant hepatitis in pregnant women High mortality rate |
Hep E
|
|
|
What kind of virus is hepatitis E?
|
Unenveloped single-stranded RNA virus
|
|
|
Hepatitis E:
Mechanism of spread Presentation |
Fecal-oral
Occurs in young/middle-aged adults living in developed nations. Typically self-limiting without chronic or carrier states. High mortality rate in pregnant women. |
|
|
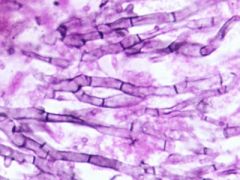
Mucor vs Aspergillus
|
Mucor and Rhizopus: broad, NON-septate angles
Aspergillia: septate, V-angles |
|
|
This organism is likely to form fungus balls.
Where? |
Aspergillus forms fungus balls in old lung cavities (as in those caused by Tb or bronchiectasis).
|
|
|
Mucor
|
|
|
Aspergillus
|
|
|
Hyponatremia
Hyperkalemia Hypoglycemia Fever Vomiting Nuchal rigidity Petechial rash |
Adrenal crisis + meningitis = Waterhouse-Friedrichsen Syndrome
|
|
|
Waterhouse-Friedrichsen Syndrome:
What is it? |
Adrenal hemorrhage (and thus insufficiency) + meningitis
|
|
|
Mental retardation
Eczema Mousy, musty body odor |
Phenylketonuria
|
|
|
Phenylketonuria:
Presentation Pathophys |
AUTOSOMAL RECESSIVE
Caused by mutation of gene encoding phenylalanine hydroxylase |
|
|
Pioglitazone:
Drug Class |
TZD
|
|
|
Thiazolidinedione:
Suffix MOA Use |
Used in DM
Improve insulin resistance by binding PPAR-gamma (involved in glucose and lipid metabolism) Causes increase in adiponectin (this is low in DMII) |
|
|
Glimepiride:
Drug Class |
Sulfonylurea
|
|
|
Sulfonylureas:
Prefix MOA Use |
Used in DM
Begin in gli- (glip, glim) Bind K-ATP chnnel on beta cells, closes them, and allows for Ca2+ channels to open |
|
|
This anti-diabetic drug binds PPAR-gamma.
|
TZDs (glitazones)
|
|
|
This anti-diabetic drug binds K-ATP channels.
|
Sulfonylureas (gli--)
|
|
|
This anti-diabetic drug binds surface tyrosine kinase-coupled receptors.
|
Insulin
|
|
|
This anti-diabetic drug binds surface adenylate cyclase-coupled receptors.
|
Glucagon like polypeptide 1 (GLP-1)
|
|
|
Glucagon like polypeptide 1 (GLP-1):
Secreted by MOA |
Secreted by intestinal L cells in response to food intake
MOA: acts through cell surface receptors coupled with adenyl cyclase G protein to induce satiety, decrease gastric emptying, and increase insulin release from beta cells (all of this decreases blood glucose) |
|
|
Volatile (inhaled) anesthetics:
Side effects |
Almost ALL increase cerebral blood flow (undesirable bc it increases intracranial pressure)
Myocardial depression Hypotension Respiratory depression Dec'd renal fn |
|
|
What is the most common cause of death in patients with TCA overdose? Why?
|
Refractory hypotension
Cardiac arrhythmias via Inhibition of Fast Sodium Channels in cardiac myocytes |
|
|
TCA anti-depressants:
MOA AEs |
MOA: Inhibit reuptake of NE and 5HT
AE: -Inhibit muscarinic receptors-->tach, mydriasis, flushing, diaphoresis, hypertherm, urinary retention -inhibit alpha-1 receptors->peripheral vasodilation--orthostatic hypotn -INHIBIT CARDIAC FAST SODIUM CHANNELS-->conduction defects, arrhythmias, hypotn -inhibit H1 receptors-->sedation |
|
|
This anti-diabetic drug requires LFTs.
|
TZD's--glitazones
HEPATOTOXICITY |
|
|
This anti-diabetic drug is contraindicated in renal failure.
|
Metformin
|
|
|
This anti-diabetic drug can aggravate CHF. How?
|
TZDs--glitazones
Cause fluid retention |
|
|
32 year-old female presents with malignant breast mass
History of osteosarcoma Family history of brain tumor, rhabdomyosarcoma |
Li-Fraumeni syndrome
|
|
|
Li-Fraumeni Syndrome:
Presentation Pathophys |
Autosomal DOMINANT predisposition to variety of cancers; sarcomas and tumors of breast, brain, and adrenal cortex are most common.
Assocd w/p53 gene mutation |
|
|
Rb gene:
Role Associated disease |
Regulates G1-S checkpoint of cell cycle
Mutation predisposes to retinoblastomas and osteosarcomas |
|
|
BRCA-1 gene mutations can result in _______.
|
Breast and ovarian cancers
|
|
|
APC gene mutations can result in ________.
|
Familial polyposis syndromes (responsible for maintaining low levels of beta-catenin, which is oncogenic, and for intracellular adhesion)
|
|
|
Progressive lower back pain not relieved by rest or position change
Urinary urgency Nocturia Frequency Hesitancy |
Prostate cancer with metastases to bone
|
|
|
NF-kappa B:
Role Disease association |
Responsible for cytokine production (NOT ANTIBODY PRODUCTION)
WHen appropriate immune response to intracellular microbes is blunted, microbes persist and induce chronic inflammation within GI tract (Crohn's) |
|
|
NOD2 Gene:
Role Disease Association |
Acts as intracellular microbial receptor that triggers NF-kappa B pathway
|
|
|
Infant with increased head circumference
Enlarged ventricles Irritability Poor feeding |
Hydrocephalus
|
|
|
Hydrocephalus:
Pathophys Presentation |
Impaired CSF outflow due to congenital abnlts
PResents with irritability, poor feeding, muscle HYPERTONICITY and HYPERREFLEXIA from upper MN damage caused by stretching of periventricular pyramidal tracts. |
|
|
QT interval:
What is it? Anti-arrhythmics that prolong it |
Remember: QT-interval = ventricular repol as ventricles prepare for next bear.
Repolarization mediated by K+ EFFLUX so class 3 antiarrhythmics (K+ blockers will prolong QT): Sotalol Amiodarone Ibutilide Dofetilide |
|

|

|
|
|
Difficulty chewing
Persistent headaches of recent onset Tenderness over temples |
Giant cell (temporal) arteritis
|
|
|
Giant cell arteritis:
Presentation Histologic features |
Jaw claudication (lameness)
HA, facial pain, vision loss Histology demonstrates granulomatous inflammation of the media |
|
|
This condition bears histologic resemblance to giant cell arteritis.
How does it differ from giant cell arteritis? |
Takayasu arteritis--may present with medial granulomas, but typically affects aortic arch. Affects women under 40.
|
|
|
Positive monospot test
|
EBV--sheep serum agglutination
|
|
|
How would HIPAA differ for a physician working with an NCAA Division I collegiate football team.
|
Trainer or team physician is allowed to communicate with coaches and protect player from further injury based on best medical judgment.
|
|
|
What processing steps must occur before mRNA can enter the cytoplasm?
|
pre-mRNA (aka hnRNA) must undergo:
-5'-capping (protects mRNA from degradation by exonucleases) -Poly A tail addition to 3' end (in cytosol, polyA tail is gradually shortened, leading to mRNA degradation) -Intron splicing |
|
|
P bodies:
Location Role |
Cytoplasm
Regulate mRNA decay |