![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
84 Cards in this Set
- Front
- Back
|
Nabothian Cyst |
benign, simple cyst found in cervical region of uterus |
|
|
Symptoms of Nabothian Cyst |
asymptomatic unless very large |
|
|
Nabothian Cysts are more common in.... |
women who have been pregnant |
|
|
Measurement of Nabothian Cyst |
< 2cm |
|
|
Sonographic Appearance of Nabothian Cyst |

-simple -discrete -round -anechoic |
|
|
What is the most common finding on pelvic ultrasound? |
Nabothian Cyst |
|
|
Adenomyosis |
inner lining of uterus (endometrium) breaks through muscle wall of the uterus (myometrium) AKA endo migrates into myometrium |
|
|
Adenomyosis is seen in what percent of hysterectomies? |
70% (2/3) |
|
|
In Adenomyosis, the ectopic glands are typically seen how far below the endo-myometrium junction? (mmt) |
2-3mm |
|
|
2 Causes of Adenomyosis |
1. defect/absence of basement membrane at junction 2. endo migration by lymph of vascular channels |
|
|
Risk Factor of Adenomyosis |
uterine trauma (more common in mature reproductive age patients) |
|
|
Signs & Symptoms of Adenomyosis |
- uterine tenderness (dull, achy pain) - dysmenorrhea - dysfunctional menstrual bleeding (irregular) - menorrhagia (heavy bleeding for several days) - uterine enlargement |
|
|
Differential Diagnosis for Adenomyosis |
-fibroids -pelvic congestion syndrome -endometriosis -endometrial polyps -endometrial carcinoma |
|
|
Treatment for Adenomyosis (if patient doesn't want Hysterectomy) |
-GnRH inhibitors -Birth control pills -nSAIDS (steroids) -Endometrial Ablation -Uterine Artery Embolization |
|
|
The only sure Treatment of Adenomyosis is.. |
Hysterectomy |
|
|
Fibroids co-exist with Adenomyosis in what percent of cases? |
>60% |
|
|
Sonographic Appearance of Adenomyosis |
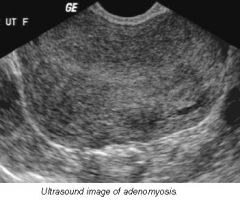
-rounded enlargement of uterus WITHOUT focal mass -abnormal heterogenous myometrium -poor definition of endomyometrial junction -Doppler: hypervascularity throughout uterus |
|
|
*Key Sonographic Finding of Adenomyosis |
Enlargement of uterus will be greater posterior to endometrium |
|
|
Sonographically, how can we differentiate Adenomyosis from Fibroids ? |
fibroids- will have focal, defined mass & peripheral vascularity adenomyosis- no focal mass & diffuse hypervascularity |
|
|
Which imaging modality is most sensitive to Adenomyosis? What are the disadvantages? |
MRI -cost -scheduling -insurance (pre-cert) |
|
|
Hystersalpingogram (HSG) & disadvantages |
radiology procedure that inserts contrast to look at uterus, fallopian tubes & surrounding area - not very specific - very uncomfortable for patients - does not always provide diagnosis |
|
|
Appearance of Focal Adenomyosis |
-poorly delineated margins -may appear as intracavitary polyp |
|
|
Diffuse Adenomyosis *most common form |
- entire uterus involved - often associated with endometrial hyperplasia & carcinoma |
|
|
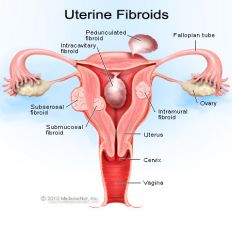
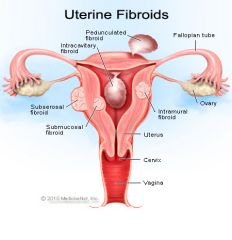
Fibroids |
benign growth of uterus |
|
|
Fibroids AKA... |
leiomyomas myomas leiomas fibromyoma |
|
|
What is the most common tumor of the uterus & female pelvis? |
Fibroid |
|
|
What is a Fibroid composed of? |
-smooth muscle -connective tissue |
|
|
Incidence of Fibroids |
20-30% women over 30 more common in African Americans |
|
|
Cause of Fibroids |
idiopathic (unknown) |
|
|
What does Estrogen do to Fibroids? |
increases! |
|
|
Why do Fibroids tend to shrink after menopause? |
lack of Estrogen |
|
|
Do we typically see 1 Fibroid, or multiple? |
multiple |
|
|
What do Fibroids cause in the Uterus? |
- enlargement - surface lobularity (bumpy) |
|
|
What feature do Fibroids have that allow them to be removed with little disruption to surrounding myometrium? |
they are encapsulated |
|
|
Signs / Symptoms of Fibroids |
- palpable pelvic mass - uterine enlargement - pelvic pain - dysfunctional uterine bleeding (DUB) |
|
|
How do Fibroids in the Endometrium affect pregnancy? |
- increased risk of miscarriage |
|
|
How do Fibroids in the Cervix or Lower Uterine Segment affect pregnancy? |
can interfere with delivery -should be closely monitored |
|
|
3 Types of Fibroids & their locations in myometrium |
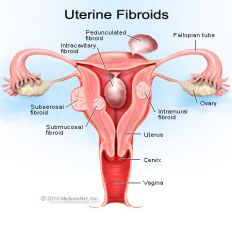
1. Submucosal - innermost 2. Intramural - center 3. Subserosal - outer |
|
|
2 Types of Subserosal Fibroids |
1. pedunculated 2. exophytic |
|
|
Submucosal Fibroid |
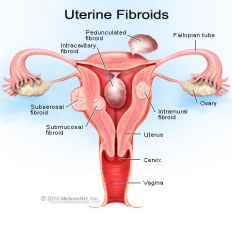
- innermost - will affect endometrium |
|
|
Which Fibroid is most likely to cause symptoms? What are they? |
Submucosal - irregular / heavy menses |
|
|
Intramural Fibroid |
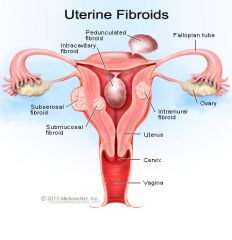
- center - do not effect endo unless large - usually will not have defined borders - usually multiple found = enlargement of uterus |
|
|
What are Intramural Fibroids sometimes defined as? |
"Heterogenous Echotexture" "Fibroid Uterus" "Diffuse Enlargement of Uterus" |
|
|
What is the most common type of Fibroid? |
Intramural |
|
|
Subserosal Fibroids |
- outer - distorts outer contour of uterus (lumpy uterus - ecophytic fibroids) - can become pedunculated |
|
|
Pedunculated Fibroid |
- grows outside of uterus with a stalk - can twist and undergo torsion |
|
|
Parasitic Leiomyoma |
exophytic fibroid in close contact with another adjacent pelvic structure and acts as a parasite on the structures blood supply - can become detached fromuterus completely |
|
|
What will happen if a parasitic fibroid outgrows their blood supply? And what are the 4 types? |
Degenerate -Hyaline -Cystic -Calcific -Red Degeneration |
|
|
Hyaline |
(Degeneration of fibroid) -fibrous tissue replaces smooth muscle cells |
|
|
Cystic |
(Degeneration of fibroid) -hyaline tissue degenerates leads to liquefaction necrosis |
|
|
Calcific |
(Degeneration of fibroid) -most often occurs after menopause |
|
|
Red Degeneration |
(Degeneration of fibroid) -acute form; results from muscle infarction (most common during pregnancy) |
|
|
What do parasitic leiomyomas look like as degeneration, calcification or growth occur? |
-heterogenous -appear hypoechoic in comparison to myometrium |
|
|
What are the two differential diagnosis of parasitic leiomyoma? |
-adnexal mass (fibroids will have shadowing that varies) -endometrial polyp (vascularity around periphery in fibroid, one single vessel in polyp) |
|
|
Sonographic appearance of parasitic leiomyoma |
-may appear as focal, hypoechoic mass -subtile changes in myometrial echotexture -focal masses: hypoechoic rim |
|
|
Complications of Parasitic Leiomyoma |
-hydronephrosis: large pelvic mass could obstruct ureters -increased incidence of miscarriages -can obstruct delivery -infertility |
|
|
Treatment of a parasitic leiomyoma |
-most commonly no treatment at all If it's causing symptoms: -hysterectomy -myomectomy (taking fibroid out) -lupron (shrinks fibroids) -uterine artery embolization (don't want hysterectomy or don't plan to get pregnant) |
|
|
What is a endometrial polys |
-localized overgrowths of endo tissue -may be peculated, broad-based or thin stalk -may see 'feeder vessel' |
|
|
Endometrial Polyps stem from? |
ENDOMETRIUM |
|
|
Leiomyomas stem from? |
MYOMETRIUM |
|
|
Signs and symptoms of Endometrial Polyps |
-asymptomatic -infertility (multiple polyps) -postmenopausal bleeding (PMB) -abdominal uterine bleeding (AUB) -incidental finding on dilation curettage (D&C) |
|
|
What does Endometrial Polyp look like on ultrasound? |

-focal thickening of endo -discrete mass: focal, round, more hyperechoic -possible feeder vessel in stalk -heterogenous as increases in size -***do not shadow -sonohysterography (SIS) determine size & location |
|
|
Endometrail Hyperplasia |
-proliferation of endometrial glandular tissue -diffuse or may not involve entire endo tissue |
|
|
What percent of endometrial hyperplasias progress into endo carcinoma? |
approx 25% |
|
|
What are some causes of endometrial hyperplasia? |
-unopposed HRT -persistent and anovulatory cycles -polycistic ovarian disease (PCOD) -obesity -estrogen producing tumors of ovary (granolas cell tumors, thecomas) |
|
|
Differential Diagnosis of endometrial hyperplasia? |
-u/s should be performed immediately after menses -D&C with thorough pathology examinations |
|
|
What does endometrial hyperplasia look like on ultrasound? |
-smooth, homogenous, echogenic -possible cystic changes Premeno: Echo complex (EC) > 14mm Postmeno on estrogen only: EC 5mm Postmeno on cycling in estrogen: 8mm in porgesterone: EC decreases |
|
|
Asherman's syndrome |
-adhesions of endometrium that develop as a result of trauma |
|
|
What is asherman's syndrome typically a result of? |
-C-section (C/S) -Dilation Curettage (D&C) -Elective abortion/Therapeutic abortion -Miscarriage (at any point) |
|
|
Asherman's syndrome can result in what? |
-infertility or recurrent pregnancy loss |
|
|
Asherman's Syndrome requires what to diagnose? |
-Sonohysterography (SIS) -HSG still gold standard at this point (x-ray) |
|
|
What is the treatment for Asherman's Syndrome? |
-remove adhesions under hysteroscope |
|
|
Uterine Sarcoma |
(MALIGNANT) -aggressive with poor prognosis -early detection increases odds of survival -difficult to differentiate from degenerating fibroid |
|
|
Why is it difficult to differentiate a sarcoma from a fibroid? |
-local invasion and distant metastasis are clues -if increases in size from baseline study |
|
|
What is the most common gynecological malignancy? |
Endometrial Carcinoma |
|
|
What are the risk factors of endometrial carcinoma? |
-obesity (50 pds over weight 2 to 3x more likely) -nulliparous (2 to 3x more likely -late menopausal (after 52 years) -pt w hx of polyps -family hx of EC -unopposed estrogen (25% develop EC) -hx of tamoxifen (if there are abnormalities prior, then 18 fold increase of EC) |
|
|
What causes decreased risks of endometrial carcinoma? |
Women on BCP for period of 12 months (safe for 10 years) -most noticeable in nulliparous pts Smoking -decreased obesity -menopause 1 to 2 years earlier |
|
|
What are some statistics of endometrial carcinoma |
-usually diagnosed in 6-7th decade (50-60 yrs) -higher in white women -higher rate of mortality in black women |
|
|
What are signs and symptoms of endometrial carcinoma |
Uterine bleeding -currently all symptomatic puts should be biopsied |
|
|
What are the treatments for endometrial carcinoma? |
-total hysterectomy -bilateral salpingo-oophorectomy -peritoneal fluid aspiration and washing -possible lymphadenectomy |
|
|
Whats the sonographic appearance of endometrial carcinoma |

-heterogenous echotexture irregular or poorly defined margins -cystic changes within endo -may see hydrometra or hematometra -enlargement of ut w lobular contour -pelvic fluid or ascites |
|
|
What will the subendometrail halo look like on ultrasound with endometrial carcinoma is present? |

If distinct- carcinoma may be localized Not distinct- nice halo but broken in one spot (greater incidence of metastatic spread) |
|
|
Ascites is an indication of what? |
-cancer somewhere in the body |
|
|
Why is a TV ultrasound most helpful in identifying endometrial carcinoma? |
-showing myometrial invasion is clear evidence -shown as thickening and irregularity of endo interface |