Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
Apoptosis
|

-Programmed cell death caused by the activation of capsases
-No inflammation -Intrinsic Pathway; Involved in tissue remodeling. Bcl-2 is anti-apoptotic, BAX/BAK are pro-apoptotic -Extrinsic Pathway; (1) Fas ligand/Fas receptor (2) Cytotoxic T-cell release perforin and granzyme B -Apoptotic bodies are phagocytosed |
|
|
Necrosis
|
-Cell death that is always pathologic and accompanied by inflammation
|
|
|
Types of necrosis
|
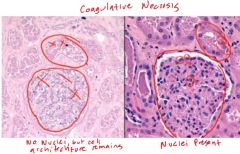
-Coagulative; infarction (except in the brain), wedge shaped. First protein denaturation then enzymatic degradation.
-Liquefactive; brain and bacterial infection. Damage due to lysosomal enzymes -Caseous; looks like cottage cheese, common in TB -Fatty; Pancreatitis, saponification -Fibroid; in vessels, malignant hypertension, stains pink -Gangrenous; Dry (ischemic coagulative) Wet (superimposed with infection). Common in limbs |
|
|
Cell Injury; Reversible
|
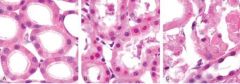
-Cellular swelling; membrane blebs (decreased ATP -> decreased Na/K pump)
-ER swelling (ribosome dissociation -> decreased protein synthesis) -Decreased oxygen -> fermentation -> lactic acid -> clumping of proteins/chromatin -Fatty change |
|
|
Cell Injury; Irreversible
|
-Nuclear breakdown (pyknosis, karyorrhexis, and karyolysis)
-Membrane damage (plasma/mitochondiral) -Lysosomal rupture |
|
|
Red vs. Pale Infarcts
|

-Red; hemmorrhagic, occurs in loose tissue with multiple blood supplies (liver, lungs)
-Pale; occurs in solid tissues with single blood supply (heart, kidney, spleen) |
|
|
Shock; Distributive (septic, neurogenic and anaphylactic)
|
-High output failure
-Decreased pulmonary capillary wedge pressure -Vasodilation (warm,dry skin) -Failure to increase BP with IV fluids |
|
|
Shock; Hypovolemic/cardiogenic
|
-Low output failure
-Decreased pulmonary capillary wedge pressure in cardiogenic, increase in hypovolemic -Vasoconstriction (cold,clammy skin) -Able to increase BP with IV fluids |
|
|
Causes of Atrophy
|
-Decreased endogenous hormones (post-menopausal ovaries)
-Increased exogenous hormones (steroid use) -Decreased innervation -Decreased blood flow -Decreased metabolic demand (prolonged hospitalization) |
|
|
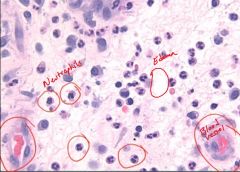
Inflammation components
|
Vascular: increased vascular permeability, vasodilation, endothelial injury
Cellular: Neutrophils leave circulation to injured tissue -> phagocytosis, degrandulaiton and inflammatory mediator release |
|
|
Acute inflammation
|
-Neutrophil mediated
-Rapid onset -Outcomes; complete resolution, abscess formation, and progression to chronic inflammation (viral infection) |
|
|
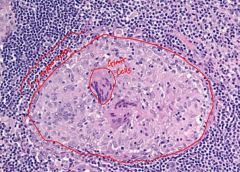
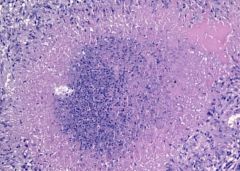
Chronic inflammation
|
-Macrophage mediated
-Characterized by destruction and repair -Blood vessel formation and fibrosis -Gramuloma formation; nodular collections of epitheloid macrophages (histiocytes) and giant cells |
|
|
Pathologic Calcifications
|
Dystrophic; when the deposition occurs locally in dying tissues (heart valves) and seen in TB, fat necrosis and infarcts/thrombi
Metastatic; the deposition of calcium salts in otherwise normal tissues (kidney, lungs and gastric mucosa); almost always a result of hypercalcemia secondary to some disturbance in calcium metabolism |
|
|
Leukocyte extravasation
|

1. Margination and rolling (E and P selectins on vessel)
2. Tight-binding (ICAM-1/VCAM-1 on vessel) 3. Diapedesis (PECAM-1 on vessel) 4. Migration (chemotactic agents - C5a, IL-8, LTB4 and bacterial products) |
|
|
Pathologic scars
|

-Hypertrophic; increased collagen synthesis, confined to the boarders of the original wound and infrequently recurs following resection
-Keloid; larger increase in collagen synthesis, extends beyond original wound, frequently recurs following resection |
|
|
Phases of wound healing
|
-Inflammatory; clots forms PMNs enter tissue, macrophages clean up
-Proliferative; deposition of granulation tissue (fibrin, myofibrin and capillaries) -Remodeling; Type III collagen replaced by Type I -> increases tensile strength of tissue |
|
|
Exudate
|
-Cellular, protein rich, specific gravity > 1.02
-Due to; lymphatic obstruction, inflammation/infection or malignancy |
|
|
Transudate
|
-Hypocellular, protein poor, specific gravity <1.012
-Due to; increased hydrostatic pressure, decreased oncotic pressure (cirrhosis) and Na+ retention |
|
|
Erythrocyte sedimentation rate
|
-Products of inflammation (fibrinogen) coat RBCs and cause aggregation -> RBCs fall at a faster rate within the test tube
|
|
|
Lipofuscin
|
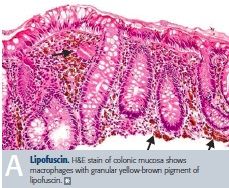
-Yellow-brown wear and tear pigment associated with normal aging.
|
|
|
Healing via secondary intention
|
-The healing of a more extensive wound such as an infarct, laceration or mechanical trauma where there is more extensive cell loss and parenchymal cells alone cannot restore normal architecture
|
|
|
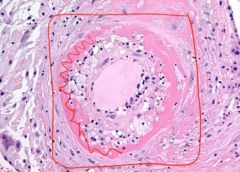
Fibrinoid Necrosis
|
|
|
|
Coagulative Necrosis - Gross
|

|
|
|
Coagulative Necrosis
|
|
|
|
Cellular swelling and fatty change
|
|
|
|
Acute Inflamation
|
|
|
|
Non-necrotizing Granuloma
|
|
|
|
Necrotizing Granuloma
|
|
|
|
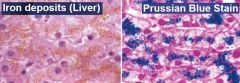
Iron Deposits
|
|