![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
136 Cards in this Set
- Front
- Back
|
cardiac output = ? |
CO = SV x HR |
|
|
mean arterial pressure = ? (2 different ones) |
MAP = CO x total peripheral resistance (TPR) MAP = 2/3 diastolic pressure + 1/3 systolic pressure |
|
|
what is the site of highest resistance in the CV system? |
arterioles |
|
|
what type of adrenergic receptors are found in arterioles? |
alpha1 adrenergic R found in arterioles of skin, splanchnic, and renal circulations beta2 adrenergic R found in arterioles of skeletal muscle |
|
|
velocity of blood flow equation? |
v = Q / A v is velocity in cm/sec Q is the blood flow in mL/min A is the cross sectional area in cm2 so velocity is lower in capillaries (sum of all caps represents large cross sectional area) than it is in aorta (small Q), allowing time for substances to diffuse across capillary wall |
|
|
SV = ? |
SV = EDV - ESV |
|
|
pulse pressure = ? |
PP = systolic pressure - diastolic pressure |
|
|
what is pulse pressure proportional to? |
PP proportional to SV and inversely proportional to arterial compliance |
|
|
what conditions cause PP to increase (cause a wide PP)? |
hyperthyroidism aortic regurg aortic stiffening (isolated systolic HT in elderly) obstructive sleep apnoea (increased sympathetic tone) exercise (transient) |
|
|
what conditions cause PP to decrease (cause a narrow PP)? |
aortic stenosis cardiogenic shock cardiac tamponade advanced heart failure |
|
|
what is the Fick principle? |
CO = (rate of O2 consumption) / (arterial O2 content - venous O2 content) |
|
|
how does exercise affect CO? |
during exercise, CO increases initially due to increase in SV during sustained exercise, CO maintained primarily by increase in HR; if HR is too high though the diastolic filling pressure then becomes incomplete so can't fill up ventricles properly because contracting too quickly so CO would then go down, and thats why in highly elevated HR such as in Afib and v-tach you cause a decrease in CO |
|
|
what is the preload? |
pressure at the EDV, when ventricles are at their fullest right before contraction atrial pressure and end diastolic pressure are measures of preload, also roughly equal to central venous pressure |
|
|
what is afterload? |
equals MAP (which is proportional to peripheral resistance) so TPR also a measure of afterload |
|
|
what increases the preload? |
exercise increase in blood volume: from over transfusion or over hydration or pregnancy |
|
|
what drugs decrease preload? |
venodilators like nitrates (nitroglycerin) |
|
|
what drugs decrease the afterload? |
vasodilators like hydralazine |
|
|
what affects SV? |
- contractility: increased contractility increases SV and vice vers - afterload: increasing afterload, decreases SV - preload: increasing it, increases SV |
|
|
what increases contractility? |
catecholamines (acting on Beta1 adrenergic receptors which increase activity in the calcium pump of the sarcoplasmic reticulum; more calcium = higher contractility) |
|
|
what decreases contractility? |
- beta1 blockade like beta-blockers - HF - acidosis - hypoxia - hypercapnia - non-dihydropyridine CCBs (verapamil) |
|
|
how can the myocardial oxygen demand be decreased in circumstances where the heart is ischemic? |
- decrease afterload (reduce systemic BP) - decrease contractility ( beta blockers) - decrease HR (beta-blockers, non-dihydropyridine CCBs) |
|
|
what can make the SV increase for a given preload? |
increase contractility: - sympathetic stimulation thru beta1 R - giving inotropic drugs like catecholamines or digoxin - increasing intracellular calcium - decreasing extracellular sodium |
|
|
what is heart ejection fraction? |
EF = SV / EDV |
|
|
what are the phases occurring in the LV during the cardiac cycle? |
(1) isovolumetric contraction: period between mitral valve closing and aortic valve opening; period of highest O2 consumption (2) systolic ejection: period between aortic valve opening and closing (3) isovolumetric relaxation: period between aortic valve closing and mitral valve opening (4) rapid filling: period just after mitral valve opening (5) reduced filling: period just before mitral valve closing |
|
|
what happens in pressure-volume loops and cardiac cycle chart if you get an increased afterload? |
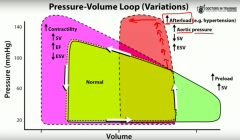
increased afterload such as in HTN means you get an in creased aortic pressure thus ventricle needs to work harder against that pressure to overcome it and enable the aortic valve to open once it does, volume decreases but so much of the contracting ability of the ventricle has been used already that you can't expel as much volume thus get decreased SV and as a result get an increase in ESV |
|
|
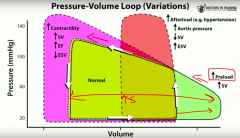
what happens in pressure-volume loops and cardiac cycle chart if you get an increase in contractility? |
increased contractility means an increased P in the ventricle as V squeezes harder afterload and preload are the same so mitral valve opens at normal time and since ventricle has increased contractility, it can eject more blood so SV is increased, EF is increased and ESV is decreased |
|
|
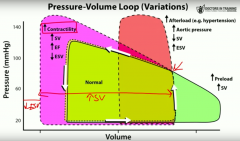
what happens in pressure-volume loops and cardiac cycle chart if you get an increase in preload? |
increase in preload means more blood in heart and most of time heart is able to eject more blood without changing the amount of pressure it is generating get an increased SV no change in ESV |
|
|
what does S1 HS correspond to? |
AV valves close loudest at mitral area |
|
|
what does S2 HS correspond to? |
closure of the pulmonary and aortic valves loudest at L upper sternal border |
|
|
what does S3 HS correspond to? what is it a/w? |
rapid ventricular filling phase in early diastole a/w increased filling pressures (mitral regurg, HF) and is more common in dilated ventricles; can be normal in children and young adults and in pregnancy |
|
|
what does S4 HS correspond to? what is it a/w? |
to "atrial kick" in late diastole best heard at apex with patient in L lateral decubitus position due to high atrial pressure and a/w ventricular noncompliance (eg hypertrophy) where LA needs to push against stiff LV wall abnormal, regardless of patient age |
|
|
what can cause an audible S3 HS? |
due to increased filling pressure - dilated CM - CHF - mitral regurgitation - L to R shunting (ASD, VSD, PDA) |
|
|
what can cause an audible S4 HS? |
- HOCM - aortic stenosis - chronic hypertension with LVH - post MI |
|
|
what does the a wave correspond to in the jugular venous pulse? |
atrial contraction absent in AFib |
|
|
what does the c wave correspond to in the jugular venous pulse? |
RV contraction closed tricuspid valve bulging into atrium |
|
|
what does the v wave correspond to in the jugular venous pulse? |
increased R atrial pressure due to filling against closed tricuspid valve |
|
|
what does the y descent correspond to in the jugular venous pulse? |
RA emptying into RV prominent in constrictive pericarditis and absent in cardiac tamponade |
|
|
where does QRS complex fall in relation to valvular dynamics? |
AV valve closure |
|
|
what is normal splitting? |
delayed closure of pulmonic valve which happens so close to closure of aortic valve that often cannot be distinguished due to decreased intrathoracic pressure brought on by inspiration --> increased VR --> increase RV filling --> increased RV stroke volume --> increased RV ejection time --> delayed closure of pulmonic valve + increased filling of RV pushes interventricular septum slightly and thus decreases LV filling space |
|
|
what is wide splitting? |
exacerbation of normal splitting a/w pulmonic stenosis or RBBB get splitting with expiration and inspiration (not just inspiration) |
|
|
what is fixed splitting? |
heard in ASD due to increased RA and RV volumes which in crease flow through pulmonic valve such that regardless of breath, pulmonic closure is greatly delayed |
|
|
what is paradoxical splitting? |
normal order of valve closure is reversed so that P2 sound occurs after delayed A2 sound heard in conditions that delay aortic valve closure, such as LBBB or aortic stenosis so on inspiration when P2 is delayed and moves closer to A2, you paradoxically eliminate the split split is thus usually heard in expiration |
|
|
when does isovolumetric contraction take place? |
during QRS complex after mitral valve closure but before aortic valve opening |
|
|
what are 4 abnormal sounds heard on auscultation of the heart which are considered benign in absence of disease signs?
|
– split S1
– split S2 on inspiration – S3 in a patient <40 – early quiet systolic murmur |
|
|
what are the diastolic murmurs?
|
mitral and tricuspid stenosis
aortic and pulmonic regurgitation |
|
|
what are the systolic murmurs?
|
AS
pulmonic stenosis mitral and tricuspid regurgitation mitral valve prolapse tricuspid prolapse VSD |
|
|
how does the valsalva manoeuvre affect murmurs?
|
makes most murmurs quieter
but increases intensity of HOCM murmur |
|
|
what are the clinical features of aortic regurgitation?
|
– best heard at the left sternal border
– heard immediately after S2 – wide pulse pressure – peripheral pulses are strong and bounding, "water–hammer" pulse – head bobbing |
|
|
what causes aortic regurgitation?
|
– aortic root dilatation (syphilis, Marfan syndrome)
– rheumatic fever – bicuspid aortic valve |
|
|
when is mitral stenosis heard? and where?
|
after a short pause following S2, with opening snap
best heard at apex of heart and in left lateral decubitus position |
|
|
what heart sounds are heard best in the left lateral decubitus position?
|
– mitral stenosis
– mitral regurgitation – L sided S3 – L sided S4 |
|
|
what causes mitral stenosis?
|
often caused by rheumatic heart disease
can result in left atrial dilation |
|
|
when is aortic stenosis heard? |
after short pause following S1 hear ejection click crescendo decrescendo murmur |
|
|
where is AS heard? and other clinical features |
heard in upper right sternal border radiates to carotids get weak, delayed peripheral pulses; can get syncope, angina, dyspnoea |
|
|
what causes aortic stenosis? |
- bicuspid aortic valve - senile / degenerative calcification - rheumatic valve disease - unicuspid aortic valve (congenital) - syphilis |
|
|
when is mitral regurg heard? where is it heard? |
immediately after S1 holosystolic murmur + high pitched and blowing hear best at apex of heart + radiates to L axilla heard best with patient in left lateral decubitus position |
|
|
what enhaces mitral regurgitation murmur? |
enhanced by increased afterload such as hand gripping, squatting |
|
|
what are the causes of mitral regurgitation? |
rheumatic heart disease endocarditis IHD left ventricular dilation mitral valve prolapse |
|
|
what causes tricuspid regurgitation? |
rheumatic fever endocarditis (in IV drug users) |
|
|
crescendo-decrescendo systolic murmur best heard in the 2nd-3rd R ICS close to sternum |
aortic stenosis |
|
|
early diastolic decrescendo murmur best heard along upper L side of sternum |
pulmonic regurgitation |
|
|
late diastolic decrescendo murmur heard best along the lower left side of sternum |
tricuspid stenosis |
|
|
pansystolic (AKA holosystolic or uniform) murmur best heard at apex and often radiates to L axilla |
mitral valve regurgitation |
|
|
late systolic murmur usually preceded by a mid systolic click |
mitral valve prolapse |
|
|
crescendo-decrescendo systolic murmur best heard in the 2nd-3rd L interspaces close to the sternum |
pulmonic stenosis |
|
|
pansystolic (AKA holosystolic or uniform) murmur best heard along the L lower sternal border and generally radiates to the R lower sternal border |
tricuspid regurgitation or VSD |
|
|
rumbling late diastolic murmur with an opening snap, heard loudest in the 5th ICS midaxillary line |
mitral stenosis |
|
|
continuous machine-line murmur (in systole and diastole) |
PDA |
|
|
high-pitched diastolic murmur a/w a widened pulse pressure |
aortic regurgitation |
|
|
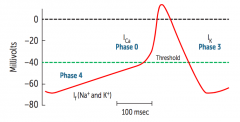
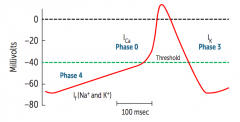
what are the phases of a myocardial AP? |
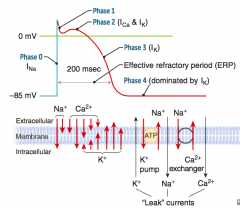
- phase O: rapid depolarization due to opening of voltage-gated Na+ channels - phase 1: initial repolarization, Na+ ch start to close and voltage-gated K+ ch begin to open - phase 2: plateau phase due to opening of gated Ca2+ ch (Ca2+ influx) which balances with K+ efflux; myocyte contraction occurs here due to Ca2+ influx triggering release of Ca2+ from sarcoplasmic reticulum - phase 3: repolarization due to opening of v-g slow K+ ch and closure of v-g Ca2+ ch - phase 4: back to baseline membrane potential, due to high K= permeability |
|
|
describe the flow of ions during a pacemaker action potential |
- phase 4: baseline membrane potential, get slow increase in Na+ conductance; slow spontaneous diastolic depolarization due to If "funny current"; If ch are responsible for a slow mixed Na+/K+ inward current, accounts for automaticity of SA and AV nodes; the slope of phase 4 determines the HR = ACh / adenosine decrease the rate of diastolic depol and decrease HR while catecholamines increase depol and HR sympathetic stimulation increase the chance that If ch are open and thus increase HR once threshold is reached: - phase 0: depolarization with opening of v-g Ca2+ ch - phase 3: repolarization back down to baseline with inactivation of Ca2+ ch and increased activation of K+ ch leading to increased K+ efflux |
|
|
what physiology accounts for the automaticity of the SA and AV node? |
the phase 4 gradual Na+ conductance |
|
|
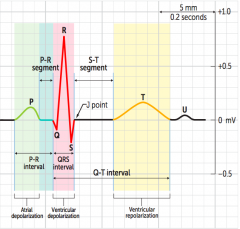
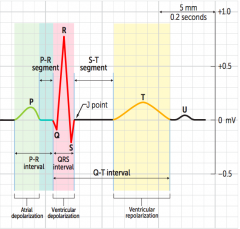
what does the p wave represent on ECG? |
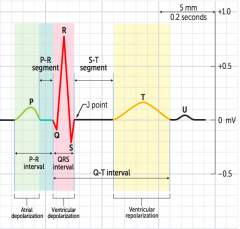
atrial depol |
|
|
what does the T wave represent on ECG? |
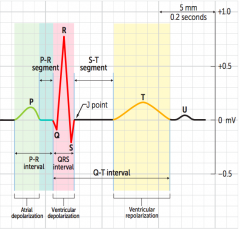
ventricular repol |
|
|
what does the QRS complex represent on ECG? |
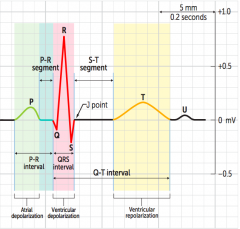
ventricular depol |
|
|
what does a T wave inversion indicate |
hypokalemia or previous MI/ischemia peaked T waves - high potassium flattened T waves - low potassium |
|
|
u wave? |
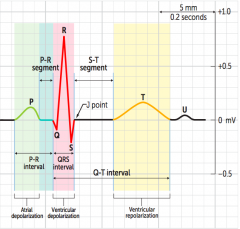
thought to be interventricular septum repol seen in hypokalemia, bradycardia |
|
|
speed of conduction in different fiber types in heart? |
purkinje > atria > ventricles > AV node |
|
|
normal duration QRS? |
<120msec |
|
|
normal PR interval? |
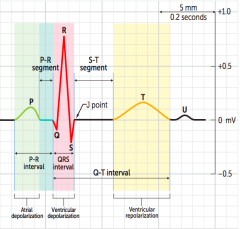
<200msec |
|
|
how does the cause of a narrow QRS complex differ from that of a wide QRS complex? |
narrow QRS complex means beat is conducted through normal pathway, going through AV node; can be a sinus beat, or an ectopic atrial beat or supraventricular tachycardia or a junctional rhythm if QRS complex is wide, depol not being normally propagated by conduction system; premature ventricular contraction, ventricular tachycardia, bundle branch block |
|
|
ECG characteristics of AFib? |
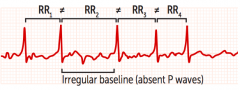
irregularly irregular no p waves |
|
|
what are the risk factors for AFib? and consequences? |
HF, hypertension, CVD / CAD (all have left atrial dilation) risk of thromboembolic events, especially stroke |
|
|
how is AFib treated? |
if less than 48hrs, synchronized cardioversion anticoagulation: heparin or enoxaparin and coumadin/warfarin, then warfarin on own rate control: digoxin, beta-blockers, CCBs rhythm control: amiodarone, sotalol, flecainide |
|
|
ECG characteristics of atrial flutter? |
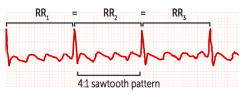
sawtooth pattern back to back atrial depol waves |
|
|
atrial flutter rx? |
same as afib definitive rx is catheter ablation |
|
|
ECG characteristics of 1st degree heart block? |
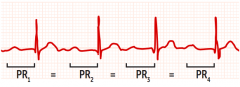
prolonged PR interval, >200msec benign and asymp no treatment required |
|
|
what bacterial infection can cause AV block? |
borrelia burgdorferi (lyme disease) |
|
|
what is Mobitz type I? ECG characteristics? |
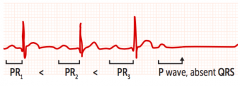
second degree heart block aka Wenckebach with progressive lengthening of PR interval until a beat is dropped, ie QRS complex absent following p wave |
|
|
what is Mobitz type II? rx? |
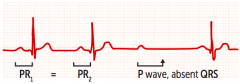
second degree heart block dropped beats not preceded by a change in length of PR interval, get absent QRS all of a sudden post p wave usu treated with pacemaker risk of progression to 3rd degree heart block |
|
|
what is a third degree heart block? ECG characteristics? other characteristics? |
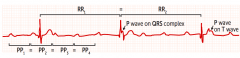
when atria and ventricles beat independently of each other p waves and QRS present but not rhythmically associated 2/3 narrow QRS and 1/3 narrow atrial rate > ventricular rate usu treated with pacemaker a/w Lyme disease |
|
|
what is Wolff-Parkinson White syndrome? characteristics on ECG? |
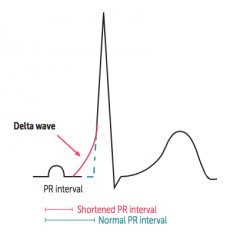
most common type of ventricular pre-excitation syndrome abnormal fast accessory conduction pathway from atria to ventricle (bundle of Kent) which bypasses rate-slowing AV node thus ventricles depol earlier characteristic delta wave with widened QRS complex and shortened PR interval |
|
|
Wolff parkinson white complication and treatment of complication? |
can result in reentry circuit leading to supraventricular tachycardia treated with procainamide (Na+ ch blocker) and amiodarone (K+ ch blocker) |
|
|
what is paroxysmal supraventricular tachycardia? HR? |
rapid heart rhythm which originates at or above AV node 2 mechanisms = reentry or automaticity usu see p waves, narrow QRS complexes (since signal from top of heart) HR >200 |
|
|
what is premature ventricular contractions? |
early occurring widened QRS complexes with bizarre morphology most often are a result of microentry at level of Purkinje fibres generating a premature complex due to a single transmission around the circuit area QRS > 4boxes or 0.16s (normal < 3boxes) usu not treated |
|
|
ventricular bigeminy and ventricular trigeminy? |
bigeminy = PVC follows each sinus beat trigeminy = 2 sinus beats followed by a PVC |
|
|
what is ventricular escape rhythm? |
when AV and SA nodes fail to generate an impulse absent p wave a/w very wide QRS complex that occurs after a pause of variable duration but always greater than normal sinus RR interval very slow rate |
|
|
junctional escape rhythm |
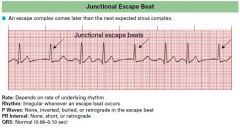
in cases of complete heart block where there is sinus node activity but failure of conduction of AV node or due to sinus bradycardia AV node takes over as pacemaker relatively slow rate get narrow QRS complexes can get inverted p waves and can be before or after QRS complexes or be hidden by it depending on where the pacemaker is in the AV junction |
|
|
what is ventricular fibrillation? |
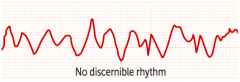
a completely erratic rhythm with no identifiable waves; fatal arrhythmia without immediate CPR and defibrillation |
|
|
what is torsades de pointes? ch on ECG? what can it progress to and what are the risk factors? |
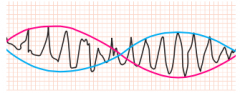
a polymorphic v-tach ch by shifting sinusoidal waveforms on ECG can progress to VFib long QT interval predisposes to torsades de pointes |
|
|
what causes torsades de pointes? |
drugs decrease K+ decreased Mg+ congenital abnormalities |
|
|
torsades de pointes Rx? |
includes magnesium sulfate |
|
|
drugs that can cause a prolonged QT? |
ABCDE + a few anti-Arrhythmics (class IA, III) anti-Biotics (macrolides) also chloroquine anti-Cychotics (haloperidol) anti-Depressants (TCAs) anti-Emetics (ondansetron) anti-HIV protease inhibitors (-navirs) methadone |
|
|
what is congenital long QT syndrome? and what are two examples of this syndrome? |
an inherited disorder of myocardial repolarization, typically due to ion channel defects Romano-ward syndrome: AD, pure cardiac phenotype (no deafness) Jervell and Lange-Nielsen syndrome: AR, sensorineural deafness |
|
|
what is Brugada syndrome? |
AD disorder, most common in asian males ECG pattern of pseudo-right bundle branch block and ST elevations in V1-V3 |
|
|
what risks are a/w Brugada syndrome? how do you prevent? |
increased risk of v-tach and SCD prevent SCD with implantable cardioverter defibrillatory |
|
|
role of ANP? |
vasodilation and decreases Na+ reabsorption at the renal collecting tubule dilates afferent renal arteriole and constricts efferent arterioles (promoting diuresis and contributing to aldosterone escape mechanism) |
|
|
ANP mechanism of action? |
acts via cGMP |
|
|
BNP clinical use? |
used for diagnosing HF (very good negative predictive value) |
|
|
what is nesiritide? |
recombinant form of BNP used in the Rx of BNP |
|
|
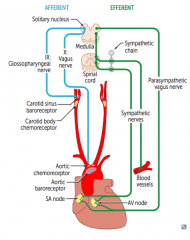
how do aortic arch receptors transmit info about BP to brain and where specifically? |
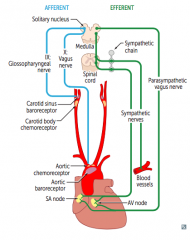
transmit via vagus nerve to solitary nucleus of medulla |
|
|
what nerve innervates the carotid sinus? |
glossopharyngeal nerve which projects to the solitary nucleus in the medulla |
|
|
outline the effects of hypotension on baroreceptors |
hypotension --> decreased arterial pressure --> decreased stretch --> decreased afferent baroreceptor firing --> increased efferent sympathetic firing and decreased efferent parasympathetic stimulation --> vasoconstriction + increased HR + increased contractility + increased BP |
|
|
what effect has a carotid massage on HR? |
carotid massage increases pressure on carotid sinus --> increased stretch --> increased afferentbaroreceptor firing --> increases AV node refractory period --> decreases HR |
|
|
what is Cushing's triad? |
hypertension bradycardia respiratory depression |
|
|
describe Cushing's reflex |
increased ICP constricts arterioles --> cerebral ischemia --> increased pCO2 and decreased pH --> central reflex sympathetic increase in perfusion pressure (HTN) --> increased stretch --> peripheral reflex baroreceptor-induced bradycardia |
|
|
what stimulates peripheral chemoreceptors? |
carotid and aortic bodies are stimulated by decrease in pO2 (<60mmHg), increase in pCO2, and decrease in pH of blood |
|
|
what stimulates central chemoreceptors? |
stimulated by changes in pH and pCO2 of brain interstitial fluid, which in turn are influenced by arterial CO2; dont directly respond to pO2 |
|
|
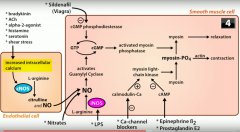
what substances stimulate cNOS? and how? |
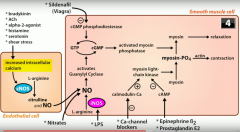
they increase intracellular calcium which stimulates cNOS and thus production of NO bradykinin shear stress ACh alpha 2 agonist histamine serotonin |
|
|
what does NO do to vessels and how? |
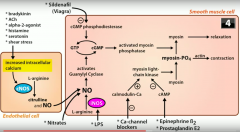
it causes vasodilation by activating guanylyl cyclase --> GTP converted to cGMP --> activates myosin phosphatase which dephosphorylates myosin and induces relaxation of smooth muscle cells |
|
|
role of nitrates? |
cause vasodilation by producing NO |
|
|
effect of sildenafil on vessels? mechanism of action? |
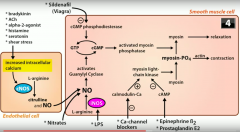
cause vasodilation MoA = inhibit cGMP phosphodiesterase |
|
|
role of cGMP phosphodiesterase in physiology of vaso-constriction/dilation? |
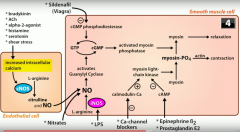
cGMP phosphodiesterase converts cGMP to GTP preventing cGMP to activate myosin phosphatase to dephosphorylate myosin and cause vasodilation thus inhibiting cGMP phosphodiesterase inhibits relaxation of vessels and induces vasoconstriction |
|
|
how do CCBs prevent vasoconstriction? |
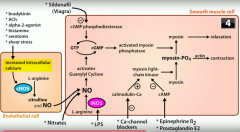
inhibit formation of calmodulin-Ca2+ complex which activates myosin light chain kinase to phosphorylate myosin --> myosin-PO4 with actin causes contraction of smooth muscle |
|
|
role of cAMP on myosin light chain kinase? |
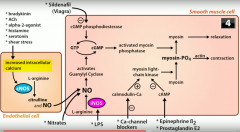
inhibits it thus preventing contraction of endothelial smooth muscle |
|
|
what stimulates cAMP to inhibit endothelial smooth muscle contraction? |
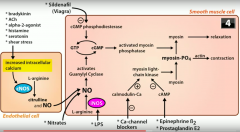
epinephrine beta2 prostaglandinE2 |
|
|
what organ receives the largest portion of systemic CO? |
liver |
|
|
what organ receives the highest amount of blood flow per gram of tissue? |
kidneys |
|
|
when does myocardial perfusion occur? |
during diastole |
|
|
what is the O2 extraction rate of the heart? what is it generally in other tissues? what is the consequence of this? |
heart extracts 80% of O2 from blood in other tissues, usu about 25% (and can go up to 75-80% in increased O2 demand) § so if heart requires more O2, can't extract that much more and hence need to increase coronary blood flow to get more O2 to tissue |
|
|
effect of hypoxia no vasculature? |
causes vasodilation except in pulmonary vasculature as hypoxia cause vasoconstriction in an effort to redirect blood to well ventilated areas / so that only well ventilated areas are perfused |
|
|
why is nitroglycerin given to angina patients? |
NO does vasodilate coronaries, but coronaries are already maximally dilated so not why we give it give nitroglycerin to induce systemic venous vasodilation which reduces preload and decreased the myocardial O2 demand |
|
|
autoregulation definition |
how blood flow to an organ remains constant over a wide range of perfusion pressures |
|
|
what factors determine autoregulation of the heart? |
local metabolites (vasodilatory) such as: adenosine, CO2, NO, decreased O2 when heart is underperfused: CO2 starts building up and cause vasodilation, NO also helps to maximise vasodilation of coronaries adenosine (part of ATP) seen as a starvation molecule so is a very potent vasodilator |
|
|
what substances act on smooth muscle myosin light chain kinase and how does this affect BP? |
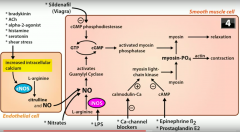
epinephrine acting at beta2 R prostaglandin E2 dihydropyridine calcium channel blockers all cause relaxation of vascular smooth muscle, leading to vasodilation --> decrease in BP |
|
|
what can cause edema or excess fluid outflow into interstitium? |
increased capillary pressure (HF) decreased plasma proteins (nephrotic syndrome, liver failure, protein malnutrition) increased capillary permeability (toxins, infections, burns) increased interstitial fluid colloid osmotic pressure (lymphatic blockage) |