![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
43 Cards in this Set
- Front
- Back
|
Average amount of urine formation a day |
Filtering 170,000mL of filtered plasma to form: 1200mL = 5 cups 'o pee pee |
|
|
Urine composition: |
95% water 5% solutes |
|
|
1/2 dissolved solids in urine consists of____________ which is from the breakdown of amino acids |
urea |
|
|
Major organic substances in pee: |
Major: creatinine, uric acid minor: hippuric aid |
|
|
major inorganic substances |
Chloride sodium potassium |
|
|
urine volume that is varied due to the secreition of ADH (give ex of disease) |
diabtetes insipidus |
|
|
Define: Oliguria anuria nocturia polyuria |
oliguria: decreased pee anuria: no more pee nocturia: pee at night polyuria: increased pee |
|
|
•Causedby a defect in the pancreatic production of insulin or a defect in the functionof insulin |
Diabetes mellitus |
|
|
What is the effect of Diabetes mellitus on blood glucose concentration? |
increases it |
|
|
polydipsia is associated with which disease |
diabetes mellitus |
|
|
the increase of glucose in the pee in diabetes mellitus has what effect on the specific gravity? |
increases it |
|
|
This disease is causedby a decrease in ADH production or a renal tubule dysfunction (inability torespond) |
Diabetes insipidus |
|
|
what is the relative specific gravity of urine from someone with: 1. diabetes mellitus: high 2. diabetes insipidus: low |
1. diabetes mellitus: high (inc glucose) 2. diabetes insipidus: low (diluted, no more ADH) |
|
|
Pee containers should be able to collect a minimum of how much pee? |
50mL |
|
|
How soon after collection should urinesbe tested? |
2 hours! if not, it must be refrigerated, put on ice or have chemical preservatives added |
|
|
PROS/CONS of refrigeration |
Pro: decreases bacterial growth Con: cancause precipitation of amorphous materials- obscures microscopic sediment |
|
|
Changes in unpreserved urine: Color: Clarity: Odor: pH: Glucose: Ketones: Bilirubin: Urobilinogen Nitrite: RBC/WBC/casts: Bacteria: |
Changes in unpreserved urine: Color: dark Clarity: dec Odor: inc pH: increased Glucose: dec Ketones: dec Bilirubin: dec Urobilinogen: dec Nitrite: inc RBC/WBC/casts: dec Bacteria: inc |
|
|
2 hour post prandial specimen is used to monitor _____________ therapy in pts with what |
insulting therapy in patients with diabetes mellitus |
|
|
•Usefulto determine the patient’s ability to metabolize a measured amount of ingestedglucose. The urine results arecorrelated with the blood glucose levels (associated with renal threshold forglucose) |
Glucose tolerancespecimens |
|
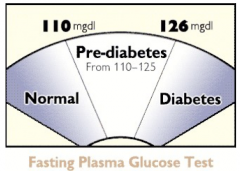
Pre-diabetes: 110-125 |
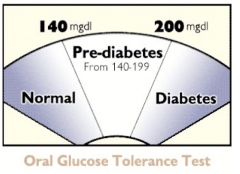
pre=diabetes: 140-199 |
|
|
Urinetemperature is take with in 4 min of collection time: |
32.5°C– 37.5°C |
|
|
Bloodpasses through the kidneys at a rate of |
•~1200ml/minor 600ml/min/kidney |
|
|
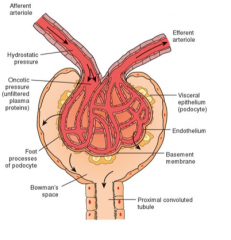
glomerulus (coil of 8 capillary lobes, non-selective filter of plasma) inside th Bowman's capsule |
|
|
Beginning of the renal tubule: |
Bowman's capsule/space |
|
|
•Re-adsorptionof essential substances occurs in the |
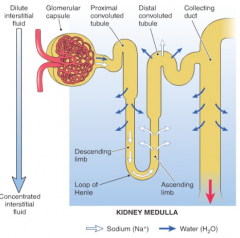
proximal convoluted tubule |
|
|
•Finaladjustment of the urinary composition occurs in the |
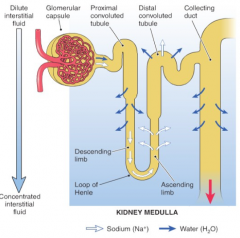
distal convoluted tubule |
|
|
place where •themajor exchanges of water and salts take place |
loop of henle |
|
|
•Nowater reabsorption in __________________ because it is impermeable to water |
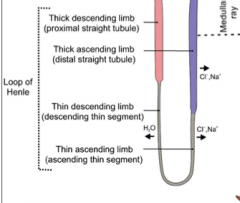
ascending loop of henle |
|
|
how big is the filter on the glomerulus |
70,000 MW very permeable to h20 |
|
|
•Threecell layers of glomerulus |
1.Capillary wall membrane = squamousepithelium•Containpores = fenestrated•Permeability 2.Basement membrane 3.Visceral epithelium•Podocytes•Filtrationslit•“Shieldof Negativity” (cations andneutral pass thru) repels anion plasma proteins |
|
|
•Maculadensasenses changes in filtrate volume and and Na+ levelsSignalsjuxtaglomerular cells to release ____________ |
renin |
|
|
•AldosteroneSecretedby leads to |
•adrenalcomplex leads to •Reabsorptionof Na+, H2O•Promotesexcretion of K+ and H+•Bloodvolume and blood pressure ↑ |
|
|
•Antidiuretichormone, ADH, VassopressinMadeby |
•Madeby hypothalamus, stored in pituitary •↑Waterretention by ↑water permeability of distal tubules•Constrictblood vessels = ↑BP |
|
|
SpecificGravity post glomerulus |
•1.010= ultrafiltrate ofplasma |
|
|
define •Passivetransport example of three things passively transported in the tubules |
Movementdue to concentration gradient or electrical potential across a membrane = gradients H2O =reabsorption everywhere but ascending loop of Henle•Urea = convoluted tubule & ascending loopof henle•Na+ = passive transport during activetransport of Cl- |
|
|
•Themaximum reabsorptionabilityfor a solute in the filtrate by the renal tubules |
•MaximalReabsorptiveCapacity (Tm) |
|
|
define •RenalThreshold |
•Theplasma concentration at which active transport stops |
|
|
Hydration= ↓ADH = ↑urine volume (less concentrated/more dilute)Dehydration= ↑ADH =↓urine volume (more concentrated/less dilute) |
Hydration= ↓ADH = ↑urine volume (less concentrated/more dilute)Dehydration= ↑ADH =↓urine volume (more concentrated/less dilute) |
|
|
Whats the diff between tubular reabsorption and tubular secretion |
Tubularreabsorption: substances removed from filtrate (urine) and returned to blood Tubular Secretion:substances move from blood (peritubular capillaries) to the tubular filtrate(urine) |
|
|
Normalblood pH |
•7.35-7.45 |
|
|
pH ofurine |
1.pH ofurine may range from 4.6 - 8.0, avg6.0 |
|
|
•Glomerularfiltration tests (3) |
•InulinClearance •CreatinineClearance •CalculatedGlomerular filtration |
|
|
•Tubularreabsorption tests (2) |
•Osmolarity •Freewater clearance |