Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
102 Cards in this Set
- Front
- Back
|
What are extrafusal muscle fibers vs intrafusal? Name function and prevalence.
|
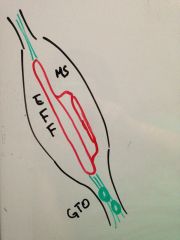
extrafusal- the contractile portion of muscle. they are the majority of the muscle fibers.
intrafusal- the muscle spindles that sit on the extrafusal fibers and detect their stretch |
|
|
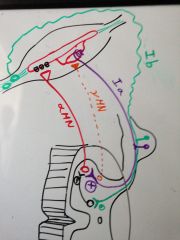
Draw the position of the extrafusal fibers, muscle spindle, and golgi tendon organs in the muscle.
|
|
|
|
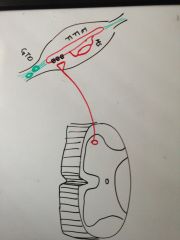
Draw where the alpha motor neurons synapse.
|
|
|
|
What receptors are present on the extrafusal fibers at this junction?
|
Nicotinic receptors for ACh.
|
|
|
How will the AP travel once the extrafusal fiber is stimulated?
|
It will travel along the entire membrane of the fiber and in through the T tubules.
|
|
|
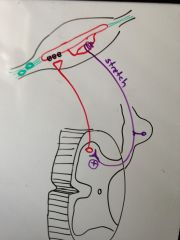
Draw how the fibers coming from the muscle spindles regulate the alpha motor neurons.
|
|
|
|
Where are the spiral muscle spindle receptors located?
|
At the very ends of the muscle spindle
|
|
|
Describe the muscle spindle reflex in words.
|
When the muscle spindles are stretched, their spiral neuron will go into the dorsal root and stimulate the alpha motor neuron to contract and "protect" the muscle.
|
|
|
What other info do muscle spindle neurons give that we will not concern ourselves with now?
|
They will send info up the spinal cord to the cerebellum about proprioception.
|
|
|
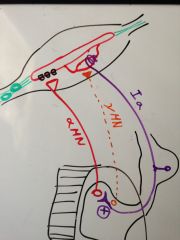
Draw in and label the neuron that controls muscle spindle contraction. Label the other two neurons as well.
|
|
|
|
How does the y-motor neuron lead to contraction of the whole muscle?
|
It contracts the muscle spindle, which stretches it and then activates the stretch reflex to stimulate the a-motor neurons.
|
|
|
What is the physiology behind muscle tone?
|
the alpha MN's are being stimulated at a sustained rate by the Ia fiber and this produces the reflexive muscle tone.
|
|
|
What OMM technique does this explain?
|
Counterstrain
|
|
|
Why is deep tendon reflex a misnomer?
|
because the thing you are stretching is the whole muscle and thus the muscle spindle, not the tendon and the golgi tendon organ.
|
|
|
What do doctors do to test the deep tendon reflexes?
|
Tap a reflex hammer lightly to the tendon to quickly and lightly stretch the muscle.
|
|
|
What do they expect to see when they stretch the muscle?
|
A reflexive contraction of the muscle.
|
|
|
What kind of reflex arc are they testing with the DTR? Name the fibers involved.
|
The muscle stretch reflex arc.
Muscle spindle--> Ia fiber --> + alpha motor neuron --> extrafusal fiber contraction |
|
|
What 5 things have you checked to be normal in a DTR?
|
1. Muscle Spindle
2. 1a fiber 3. Spinal integration 4. Alpha motor neuron 5. Neuromuscular junction |
|
|
Why do you check DTR's in different places?
|
You want to make sure that each spinal level is working.
|
|
|
When are golgi tendon organs stimulated?
|
When the tension in the muscles and tendons is so high that it threatens the integrity of the locomotor system.
|
|
|
Does the golgi tendon reflex directly inhibit the aMN?
|
No, it involved an inhibitory interneuron.
|
|
|
What is happening in ismometric contraction to the muscle and tendon length?
|
Total length stays the same, but muscle shortens and tendon lengthens.
|
|
|
What is the action of the golgi tendon reflex if I try to lift too much weight?
|
it will inhibit the muscle and drop everything to protect the muscle from tearing.
|
|
|
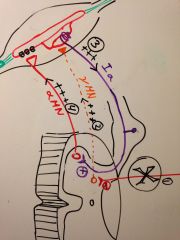
Draw in and label the fibers involved in the golgi tendon reflex?
|
|
|
|
Do upper motor neurons (UMN's) usually synapse directly on aMN's? What path do they take?
|
no, they usually go to interneurons which will inhibit the LMN's.
|
|
|
Define the parameters of a LMN lesion.
|
Any kind of disturbance from the cell body of the aMN to it's neuromuscular junction.
|
|
|
What are the two fashions in which ACh is release at the NMJ?
|
1. released when aMN is stimulated
2. basally trickling out |
|
|
What is the point of the ACh that trickles out all the time?
|
It is a trophic signal that helps to maintain muscle mass
|
|
|
What's the difference between disuse atrophy vs denervation atrophy.
|
Denervation atrophy loses basal ACh as well as AP ACh.
|
|
|
What do UMN's do to LMN's?
|
they inhibit them via interneurons (including yMNs)
|
|
|
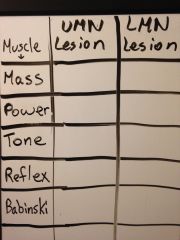
What are the signs you can use to distinguish upper vs lower motor lesions? (5)
|
1. Muscle mass
2. Muscle power 3. Muscle Tone 4. Deep Tendon Reflexes 5. Babinski's sign |
|
|
|
|
|
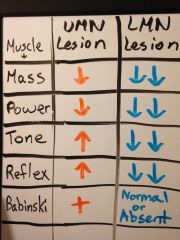
So what happens to the muscle mass if there is a LMN? Why?
|
The mass of the muscle will decrease significantly because it will have both disuse and denervation atrophy.
|
|
|
How much will it be reduced in 3 months? (%)
|
70%
|
|
|
So what happens to the muscle mass if the UMN has a lesion? Why?
|
It will only be decreased 20-30% because you still have the trophic ACh secretion and the stimulation of the stretch reflex working so you only have disuse atrophy.
|
|
|
What happens to the power of a muscle with a LMN vs UMN lesion? Why?
|
LMN lesion- power is completely lost because no ACh at all
UMN- power is slightly lost |
|
|
What is the main fiber that determines tone?
|
the yMN.
|
|
|
Is disruption of the yMN involved in a LMN lesion?
|
yes, it can be
|
|
|
So what happens to tone in a LMN lesion?
|
total loss of tone in that muscle (because of either aMN and yMN lesion).
|
|
|
Define tone.
|
muscle resistance to passive stretch
|
|
|
Explain the difference in tone between UMN lesions and LMN lesions.
|
In LMN lesion, there is complete loss of tone.
In UMN lesion, there is hypertonicity because the LMN's have escaped the inhibitory effect. |
|
|
What are the two ways in which hypertonia/rigidity is produced in a UMN lesion? (think about the two types of LMN's they affect)
|
1. yMN overfires and activates the stretch reflex
2. aMN is no longer inhibited and will fire and release basal ACh |
|
|
Draw the pathway by which hypertonia and hypereflexia happens in an upper motor lesion.
|
|
|
|
Explain the difference in tendon reflexes between UMN lesions and LMN lesions.
|
1. LMN lesion- loss of reflex because reflex arc is disruption at some point
2. UMN lesion- muscle spindle is already contracting and activating the Ia fibers. more stretch applied will cause a bigger reflex than normal. |
|
|
What is it called when a muscle has longer than normal contraction after a reflex test?
|
clonus
|
|
|
What is clonus due to?
|
it can be due to a UMN that results in basal overstimulation of aMN.
|
|
|
How do you test for Babinski's sign?
|
You draw a pen down the lateral side of the bottom of the foot and then accross the top.
|
|
|
What is the appropriate response for babies?
|
To dorsiflex the foot and effectively withdraw from the irritation.
|
|
|
What mechanism is the baby's babinski reflex due to? Why are they different?
|
local motor reflex in the lumbar spinal cord because their upper motor neurons are not completely myelinated yet.
|
|
|
What will the upper motor neurons do to the baby's withdrawal reflex when it is myelinated?
|
It will inhibit the withdrawal reflex.
|
|
|
Why can't babies walk until thier upper motor neurons are myelinated?
|
If they dorsiflex their feet when they hit the ground in walking, they will fall over.
|
|
|
So which kinds of pts have a positive babinski's sign?
|
Babies and people with upper motor lesions
|
|
|
How do normal people response to the foot irritation? What action does this help with?
|
They perform plantarflexion, which helps with walking
|
|
|
Is there such a thing as a negative babinski's sign?
|
No. That is just called normal plantar flexion reflex.
|
|
|
What is another name for a positive babinski's sign?
|
upgoing babinski's sign
|
|
|
What happens to the toes in a babinski reflex?
|
they fan out
|
|
|
When would I have a upgoing babinski's normally?
|
when I am asleep and my upper motor function is shut down.
|
|
|
What determines if a LMN lesion will produce a normal or absent babinski's sign?
|
Only if it is the LMN involved in the reflex will it become absent. Otherwise, it is normal.
|
|
|
If you are checking tone, what should their arms do if you let it go? Why?
|
It should drop to the side because they should be relaxed for this exam.
|
|
|
What are the three types of hypertonia?
|
1. Clasped knife
2. Lead pipe 3. Cog wheel |
|
|
What exam finding tells you is someone has spascity?
|
Clasp-knife feeling in muscle tone checking
|
|
|
What should hypertonia feel like in a clasped knife finding?
|
When you are trying to move them, it is very hard at first and then suddenly it gives.
|
|
|
What is the physiology behind why it is so hard to move initially?
|
The yMN's are overactive due to lack of UMN inhibition. The muscle spindles are contracted and any further stretch of the muscle will further exacerbate the stretch reflex.
|
|
|
What is the physiology behind why it suddenly gives?
|
The tendons accumulate a lot of tension from all the contraction and then the GTO reflex is activated to inhibit the LMN's.
|
|
|
How would a person with a UMN lesion fare in flexing and extending their arm? Which muscle is resisting in each movement?
|
It would be hard at first in both directions and then easy. In extension, it would be the bicep creating the resistance and in flexion it would be the tricep.
|
|
|
What kinds of pts get lead pipe hypertonia?
|
Pt's with parkinson's.
|
|
|
Describe what lead pipe hypertonia feels like. Why is it called this?
|
There is resistance to passive movement throughout the movement with no give point. Feels like you are bending a lead pipe.
|
|
|
Are extrapyrimidal or pyrimidal tracts damaged in Parkingson's?
|
extrapyrimidal
|
|
|
When these are damaged, do you get a lot or a little loss of LMN inhibition?
|
Only a little.
|
|
|
Why only a little?
|
Because the extrapyrimidal tracts are mostly supportive tone neurons and don't have as great of an effect on the LMN's.
|
|
|
So why is there a lead pipe effect in a extrapyrimidal UMN lesion?
|
Since there is only slight contraction from the stretch reflex, you don't put enough tension on the GTO's to stiimulate the golgi reflex.
|
|
|
Describe cogwheel rigidity.
|
It feel like a cog where there is alternating give and resistance as you passively try to move the muscle
|
|
|
What pathology would give you cogwheel rigidity?
|
When you heave lead pipe rigidity plus tremors.
|
|
|
Are the nicotinic receptors on the extrafusal fibers all over the fiber? Where are they?
|
No, they are only under the neuromuscular junction.
|
|
|
So are there many nicotinic channels on a regular muscle cell?
|
no
|
|
|
What happens to the number of any receptors when they are overstimulated?
|
They are downregulated
|
|
|
So what happens to the number and distribution of nicotinic receptors in denervation?
|
they increase drastically in number and become distributed all throughout the muscle.
|
|
|
What is this upregulation of nicotinic receptors in skeletal muscle called?
|
dennervation hypersensitivity
|
|
|
What happens when you tap on a regular muscle?
|
Nothing really
|
|
|
What happens when you tap on a muscle with tons of upregulated nicotinic receptors on it?
|
Some will open and cause mini action potentials and contractions.
|
|
|
What is this phenomenon called?
|
fasiculations
|
|
|
What type of neural lesion would produce fasiculations?
|
A chronic dennervation LMN lesion
|
|
|
What is the difference between fasiculations and fibrillations?
|
fibrillations are like fasiculations except that they can only be stimulated and detected by electromyography.
|
|
|
What is electromyography?
|
That test where they stick electrode prods into your muscle and stimulate it electrically to measure it's AP conduction.
|
|
|
Is there any fasiculation/fibrillation in UMN lesions?
|
No
|
|
|
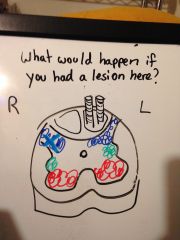
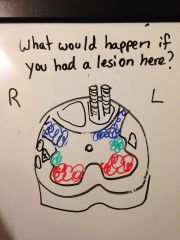
Draw a section of a spinal cord and indicate where the sensory, motor, and autonomic grey matter is.
|

|
|
|
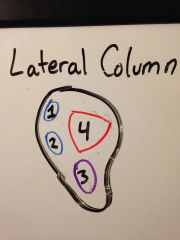
1- dorsal spinocerebellar
2- ventral spinocerebellar 3- lateral spinothalamic 4- corticospinal pyrimidal tract |
|

|
lesion at left fasiculus cuneatus -
loss of fine touch, proprioception, 2 point discrim, and vibration on the left side below the level of lesion. |
|
|
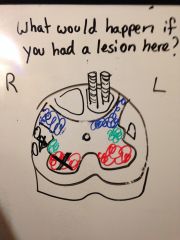
lesion at dorsal horn-
loss of all sensation on right side at that level. loss of spinoolivary input on right. loss of crude touch, pain, and temperature on that side for several levels above and below. |
|
|
What are the two questions you should ask when trying to dx a spinal cord injury?
|
What is happening at that level?
What is happening below that level? |
|
|
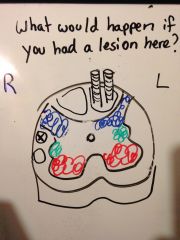
lesion at dorsal lateral tract (dorsal spinocerebellar)
right ipsilateral lower leg dystaxia |
|
|
lesion at ventral lateral tract (dorsal spinocerebellar)
left/contralateral lower leg loss of coordination |
|
|
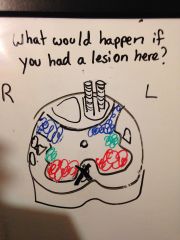
Where is the pyrimidal motor tract located in the lateral column?
|

|
|
|
loss of voluntary motor function below this level.
|
|
|
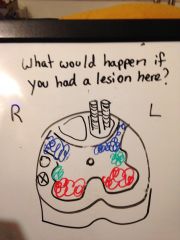
lesion of right pyrimidal column and ventral horn-
loss of right UMN function below that level and LMN function at that level |
|
|
What kind of symptoms would you see in the previous example?
|
flacidity etc at the damaged levels
spasticity etc at all the levels below. |
|
|
Where would the lesions be if you were checking a body from top to bottom and found:
1. normal reflexes 2. no reflexes 3. hyperreflexia |
at the level of no reflexes
|
|
|
lesion at right anterior column
contralateral loss of axial motor movement below that level contralateral loss of crude touch 3-4 levels below and beyond |
|
|
Which sensory systems cross anteriorly on their second order neurons? Which one is more anterior?
|
anterolateral sensory system
posterior- pain and temperature anterior- crude touch |
|
|
What does the anterior white commisure cross through?
|
The anterior column
|
|
|
What would disrupt the anterior commisure?
|
anterior dilation of the spinal cord
|
|
|
What would be the first sx if you dilated the spinal cord anteriorly at one section? Why?
|
bilaterally loss of temperature, and pain at those sections only because the anterior white commissure is the first neurons it will hit.
|