Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
|
Subepithelial deposition
|
Beneath podocytes
|
|
|
Below basement membrane, above endothelial
|
Subendothelial deposition
|
|
|
Why differential location of IC?
|
Big complexes in mesangium bc cant penetrate GBM
Small complexes can reach subepithelial levels |
|
|
Glycation
|
Linking glucose to proteins; non-enzymatic glycosylation; proteins dont work properly
|
|
|
non-specific progression of renal fibrosis
|
important bc fibrosis likely proceeds the same in many different diseases
chronic exposure to insults |
|

|
mesangiolysis with loss of tight capillary loops; loss of structure/arrangement of tight capillary loops
|
|

|
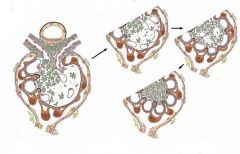
progression of mesangiolysis to ballooning
restoration towards normal architecture |
|

|
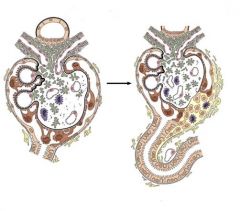
disruption of urinary space with cellular bridging
|
|
|
insudation of protein and inflammatory cells into urinary space
|
|
|
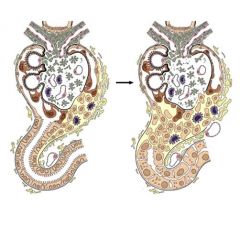
disruption of tubular architecture as well as further glomeular damage
|
|

|
complete disruption of tubular structure...if even the glomerulus
recovers it will now be unable to function |
|
|
active sediment
|
cells in cast
|
|
|
bland sediment
|
no cells/cast
|
|
|
proteinuria, bland or chronic sediment, stable or slowly creatinine
|
chronic glomerulonephritis
|
|
|
proteinuria, active sediment, progressive rapid rise in creatinine
|
rapidly progressive eglomerulonephritis
|
|
|
IgA neprhopathy
|
Women: gross hematuria
Men: microhematuria |
|
|
FARF
|
functional acute renal failure;
|
|
|
no proteinuria, bland or hyaline casts in segiment, elevated creatinine
|
functional acute renal failur
|
|
|
No proteinuria, sediment
with casts, debris, and renal tubular epithelial cells |
• acute tubular necrosis
|
|
|
No proteinuria, bland
or “chronic” sediment, stable elevated or slowly rising creatinine |
• chronic tubulo-
interstitial nephropathy |
|
|
No proteinuria, WBC’s
in urine with or without bacteria |
• infection
• acute interstitial nephritis |
|
|
differentiation between glomerular and tubular disease
|
whether or not there is protein in the urine
|
|
|
lupus demographic
|
young black females
|
|
|
what occurs in toxic insult to kidney
|
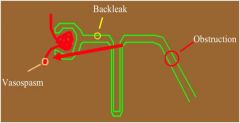
1. Vasospasm; reduces flow of blood into glomerulus
2. Backleak of filtrate into interstitium, cant form urine 3. Obstruction (due to casts of sloughed off cells) |