Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
|
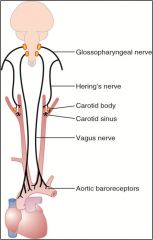
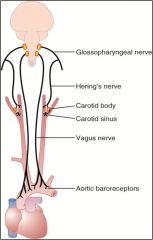
where are baroreceptors located?
|
carotid sinus (via carotid bodies)
wall of aortic arch |
|
|
How is vasomotor tone maintained?
|
Tonic stimulation of 1-2 AP's per second; if tonic contraction is not maintained there is a 50% drop in bp
|
|
|
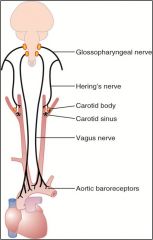
Where do you monitor flow to the head and body?
|
Head = carotid bodies/sinus
Body = aortic arch |
|
|
How are signals transmitted from the carotid sinus?
|
Herings nerve to the glossopharyngeal nerve to the nucleus tractus solitarius of the medulla
|
|
|
How are baroreceptor signals transmitted from the arch of the aorta?
|
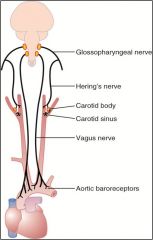
Vagus into the nucleus tractus solitarius
|
|
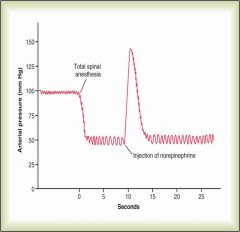
Most sensitive range for carotid sinus baroreceptors?
|
60-180 mmHg
The reflex is most sensitive at 100 mmHg (as pressure increases # of impulses from carotid sinus increase which = inhibition of vasoconstrictor center and activation of the vagal center to the heart) |
|
|
Which vascular control mechanism is the fastest?
|

Baroreceptors; act within a couple of seconds
|
|
|
Which mechanism is effective control between 60 mmHg - 180 mmHg
|

Baroreceptors
|
|
|
Why don't quick vascular control repsonses (baro/chemoreceptors) respond for long term?
|

Receptors reset according to the new pressure established
Baro/Chemo get blood w highest 02 and lowest C02 |
|
|
Which response is faster; baroreceptors or chemoreceptors?
|

Baroreceptors
|
|
|
Describe the ischemic response
|

Cerebral iscemia > increased C02 > VMC activated > increased symp activity > increased arterial pressure
|
|
|
What is the direct affect of aldoesterone related to blood pressure?
|
Stimulates the retention of sodium by the kidney (increases action of the sodium/potassium pump)
|
|
|
Best definition of shock
|
Inadequate perfusion of tissue (which can be caused by a ton of stuff obv)
|
|
|
During shock does a pt often go acidodic or alkalotic?
|
Acidotic;
Pts with a large base deficit (15 mmol) = mortality of 70% |
|
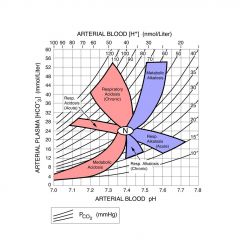
Acute Respiratory Alkalosis
|
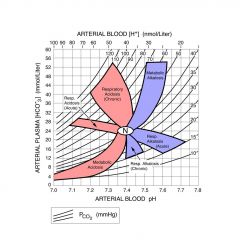
PC02 decreased, pH increased, HC03 depressed
H20 + C02 <- (carbonic anhydrase) -> H + HC03 |
|
|
Metabolic Acidosis
|
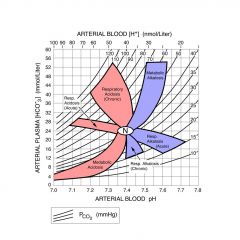
Accumultation of lactic acid because tissues are not being perfused adequately and later due to renal failure
|
|
|
Anion Gap
|
Degree of acidity experienced during metabolic acidosis
Na - Cl + HC03 Increased anion gap = decrease in bicarb levels |
|
|
Third Spacing of Fluid
|
Movement of fluid out of cardiovascular system into the tissues/other spaces
Third spacing occurs when too much fluid moves from the intravascular space (blood vessels) into the interstitial or "third" space - the nonfunctional area between cells Often happens in shock due to increased capillary permeability |
|
|
Hemorrhagic Shock
|
Loss of substantial blood volume for period of time; if rapidly returned wont produce shock
Exanguination does not equal shock; pt can die from exanguination but not be in shock; must be inadequate tissue perfusion Wigger's Model: Decreased bp to approximately 50 mmHg for several hours |
|
|
Cardiogenic Shock
|
Loss of cardiac function (pericardial, myocardial or valvular dysfunction)
|
|
|
Distributive Shock
|
Septic Shock;
can be induced experimentally by injection of endotoxin or lipopolysaccharide iv or injection of live bacteria |
|
|
L/P ratio = conc of protein in lymph/plasma
|
If capillaries are totally permeability and unable to retain protein in circulation L/P ratio = 1
As LP ratio drops it means there is a lower conc of protein in lymphatic fluid compared to plasma |
|
|
How does cortisol affect blood pressure?
|
Helps NE promote vasoconstriction
|
|
|
Renin
|
Released from kidneys; produces A1 from angiotensinogen; A1 (ACE) -> AII which is a potent vasoconstrictor
|
|
|
In the early stages of shock would there be respiratory alkalosis or acidosis?
|
A short lived respiratory alkalosis due to hyperventilation; however this is short and will become acidosis as lactate acid builds up from peripheral tissues
|
|
|
Pulmonary Shock Response
|
ARDS due to WBC release inflammatory mediators
|
|
|
Renal Shock Response
|
Acute renal failure due to decreased blood flow (so don't give antibiotics that use renal metabolism/nephrotoxicity)
Dopamine has been suggested to stimulate the cardiovascular system due to its sparing of renal blood flow |
|
|
Metabolic Shock Response
|
Build up of lactic acid due to decreased tissue perfusion; glucose levels in the plasma can be either elevated or depresed; often an increase in protein catabolism that results in a negative nitrogen balance
|
|
|
Inflammatory Response in Shock
|
Prostaglandins, TXA2, leukotrienes
Oxygen radicals from AA pathway is activated during shock |
|
|
Tx hemorrhagic shock
|
Fluids at a rapid rate to restore hemodynamic function (2-3 liters in 10 min)
If Hg conc falls below 10g/dL, blood should be given. this should be matched but if not use type 0 |
|
|
Tx cardiogenic shock
|
Pulmonary capillary wedge pressure; indicates how well heart is pumping blood; can put in a Swan-Ganz catheter to measure this
can give dopamine, NE, or dobutamine to increase PCWP Lasix can help reduce fluid loads (diuretics) |
|
|
Tx septic shock
|
Fluid tx to maintain pulmonary capillary wedge pressure at 15 mmHg
Oxygen support/ventilation drugs to increase cardiac output Antibiotics to control infection In severe wound infection debridement or drainage may be required |
|
|
Steroids have been used as a treatment for shock in patients. This was because
|
Steroids helped to reduce the movement of fluid into the interstitial space; stabilize capillary membranes
|
|
|
You are treating a 21 year old male patient who was admitted to the hospital 1 hour ago for treatment of injuries sustained in a motor vehicle accident. He lost a large volume of blood. The accident apparently occurs several hours before the paramedics were called. Once the monitors are in place, you find that he has an increased heart rate, increased cardiac output, and increased respiratory rate. These data suggest that the
|
Patient may be in the hyperdynamic phase of shock and will soon exhibit depressed cardiovascular parameters if treatment is unsuccessful.
|
|
|
A patient is in the early stages of shock. He is hyperventilating. This can result in
A. Metabolic alkalosis B. Metabolic acidosis C. Respiratory alkalosis D. Respiratory acidosis E. Mixed respiratory and metabolic acidosis |
Respiratory alkalosis
|
|
|
A patient is in the advanced stages of shock. All treatments have failed to produce an improvement in his condition. He will most likely be in
A. Metabolic alkalosis B. Metabolic acidosis C. Respiratory alkalosis D. Respiratory acidosis E. Mixed respiratory and metabolic acidosis |
Metabolic acidosis due to buildup of lactic acid
|