![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
I. Olfactory |
Olfactory Nostril Patency - assess nostril opening Sense of smell - able to identify scents |
Check nostril patencyTest sense of smell both sides |
|
|
II. Optic
|
-Test central visual acuity - cover one eye at a time and five feet away from eye scale-Test visual fields /peripheral vision - confrontation test ( wiggle finger from every direction from posterior to anterior) |
Visual acuity and peripheral fieldsConfrontation |
|
|
III, IV, VI. Oculomotor, Trochlear, Abducens |
-Equal Palpebral fissures-Pupil size/shape/reaction-Extra-ocular muscle function (EOM) - Six cardinal fields of gaze (diagnostic positions test)
|
Equal palpebral fissures, pupil size/reaction, EOM |
|
|
V. Trigeminal |
-Motorpalpate TMJ and masseter while clenching teeth-Attempt to open jaw Sensory cotton wisp on three areas of face - opthalmic, maxillary, mandibular- +/- corneal reflex -cotton ball cornea |
-Motorpalpate TMJ,masseter,clenching teeth -Attempt open jaw Sensory cotton wisp on three areas of face - opthalmic, maxillary, mandibular - +/- corneal reflex - cotton ball on cornea |
|
|
VII. Facial |
Motor - Facial symmetry -smile, frown, close eyes tight, lift eyebrows, show teeth, puff cheeks Sensory – taste - don’t test routinely, test only if facial injury |
-Motor Smile, frown, puff cheeks, lift eyebrows, show teeth Close eyelids against resistence -Sensory+/- tastes - lemon juice |
|
|
VIII. Acoustic |
Whisper test - two feet away with mouth covered, one ear covered, 2-syllable words Weber - tuning prong put under mastoid (intervals how long hear sound should be same) Rinne - Tuning prong put at top head ask which side coming from |
Hearing acuity Whisper Test - whisper in ear Weber test - Prong on top center of head Rinne Test - Behind ear touching |
|
|
Conductive Hearing Loss |
problem conducting sound waves anywhere along the outer ear, tympanic membrane (eardrum), or middle ear (ossicles).
may occur in with sensorineural hearing loss (mixed hearing loss) or alone. |
sound waves in outer ear, tympanic membrane, or middle ear |
|
|
Sensorineural hearing loss (SNHL)
|
type of hearing loss/deafness, the cause lies in the inner ear or sensory organ (cochlea and associated structures) or the vestibulocochlear nerve (cranial nerve VIII)or neural part.
|
inner ear, sensory organ, vestibulocochlear nerve, or neural part |
|
|
IX, X. Glossopharyngeal, V agus |
Sensory Taste posterior tongue-hard test Client says: “ahhh” – uvula midline and mobile and tonsillar pillars move medially, gag reflex intact |
Motor Uvula midline and mobileTonsillar pillares medial mobile Gag reflex |
|
|
XI. Spinal accessory |
Sternomastoid muscle and trapezius muscle – test strength |
Sternomastoid and trapezius muscle strength |
|
|
XII. Hypoglossal |
Stick out tongue and note midline, say ‘light, tight, dynamite’ and note clear distinct speech |
Clear speechstick put tongue"light tight dynamite" |
|
|
Complete neurological examination Objective Data -Mental Status |
–Arousal •Grossresponse to stimuli •Glasgow Coma Scale (GCS)(review page 698-699) –Eyeopening - 4 –Verbalresponse – 5 –Motorresponse – 6 –Awareness •Aware of orientation |
–Name,location, time–A& O x 3 -Thought process -Logical, goal directed, coherent,relevant -Appearanceand behavior -Dress, hygiene, facial expressions-Speech-Pace, articulation |
|
|
Neurological Recheck
|
•Level of consciousness –Person –Place –Time •Motorfunction •Pupillary response •Vital signs |
|
|
|
Complete neurological examination Objective Data -
Reflexes
|
-Test the superficial reflexes -Abdominal reflex -Cremastericreflex -Plantar reflex •Test the deep tendon reflexes –Technique
|
–Grading –Reinforcement –Bicepsreflex –Tricepsreflex –Brachioradialis reflex –Quadricepsreflex –Achillesreflex –Clonus |
|
|
Complete neurological examination Objective Data - Sensory System |
Posterior column tract -Vibration Position (kinesthesia) -Tactile discrimination (fine touch) -Stereognosis -Graphesthesia -Two-point discrimination -Extinction -Point location |
•Guidelines for testing
•Spinothalamic tract –Pain –Temperature –Lighttouch |
|
|
Complete neurological examination Objective Data - Motor System |
Muscles -Size -Strength -Tone -Involuntary movements Cerebellarfunction –Balance tests•Gait •Tandemwalking •Romberg’s test •Shallowknee bend |
–Coordinationand skilled movements
•Rapidalternating movements •Finger-to-fingertest •Finger-to-nosetest •Heel-to-shintest |
|
|
Test visual fields /peripheral vision |
confrontation test
-check every field by moving finger from posterior to anterior |
|
|
|
Inspection Extraocular muscle function |
-Corneal light reflex
- not pupillary response -Six cardinal fields of gaze - diagnostic positions test -cover -uncover |
|
|
|
Objective Focused Assessment Ears |
•Inspect and palpate external ear •Hearing acuity (after otoscope exam) –Size and shape -Whisper test –Skin condition -Vestibular Apparatus –Tenderness -Romberg Test•Pinnaand tragus
|
-+/-Otoscope exam •Mastoidprocess –Externalauditory meatus |
|
|
Objective Focused Assessment Eyes |
-Inspect External Ovular structures -Inspect Anterior Eyeball Structures
-External to internal -Cornea & lens -Eyebrows -Iris & Pupil -Eyelids & lashes -Pupillary light reflex |
-Eyeballs
-Direct & consensual-Conjunctiva & sclera -Accommodation & convergence-Lacrimal apparatus -PERRLA |
|
|
Objective Focused Assessment - Nose, Mouth, Throat |
•Inspect& palpate the nose -Inspect the throat –External nose -Tonsils –Nostril patency -Breath •+/-Inspect nasal cavity (not required) •Palpatesinus areas |
•Inspectmouth
–Lips –Teeth & gums –Tongue -Buccal mucosa -Palate -Uvula |
|
|
Structure and Function - Breasts |
Internal anatomy •Glandulartissue –Lobes,lobules, and alveoli -Lactiferousducts and sinuses
|
•Fibroustissue –Suspensoryligaments or Cooper’s ligaments –Run Vertical –Attach breasts to chest wall –One Sign breast cancer •Adipose tissue –Subcutaneous tissue Four Quadrants |
|
|
Structure and Function - Lymphatic |
•Axillary nodes –Central(armpit) –Pectoral(anterior) –Subscapular(posterior) –Lateral(lateraltowards arm) |
|
|
|
Subjective Data Breasts—Health History Questions |
•Breast –Pain –Lump –Discharge –Rash –Swelling -Surgery –Trauma(Lump can be caused by bruise) –History of breast disease-(Genetics play a role) •Axilla –Tenderness, lump, or swelling –Rash
|
•Axilla–Tenderness, lump, or swelling
–Rash |
|
|
Objective Data—Physical Exam - Breast Exam |
Preparation Breasts - Inspect –Position -General appearance –Draping -Skin -Nipple Equipment -Lymphatic drainage areas –Smallpillow -maneuvers to screen retraction –Pamphletor |
Axillae—Inspect and Palpate•Skin •Palpation technique •Lymphnodes
Breasts—Palpate•Position •Palpation patterns•Nipple •Bimanual palpation Male Breast Exam - Pg. 422 |
|
|
Objective Neck Assessment |
•Inspectand palpate –Symmetry •Head •Trachea •Accessoryneck muscles –ROM |
–Musclestrength
•Cranialnerve XI –Lymphnodes •Fig14.6 |
|
|
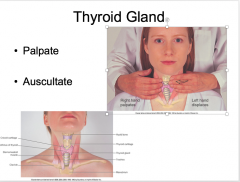
Thyroid Gland |
|
|
|
|
5 As forIntegrating Knowledge of Substance Use in Health Assessment |
-Acquire knowledge; replace erroneous assumptions -Anticipate harm that may be causedby your practices, reactions, judgements - Avoid social judgement about substance use, such as seeing a person as “bad,” deviant, or morally weak - Analyze organizational practices(e.g., clinical assessment tools) and resources -Approach patients respectfully |
- Avoid social judgement about substance use, such as seeing a person as “bad,” deviant, or morally weak- Analyze organizational practices(e.g., clinical assessment tools) and resources-Approach patients respectfully
|
|
|
Challenging the Idea of “Choice” |
-Understanding drug use as “choice”draws attention away from underlying causes and factors influencing substance use; increases likelihood of blame/stigmatization
|
-Avoid commonly held assumptionsthat people in particular ethnocultural or social groups use alcohol ordrugs more than others
|
|
|
Putting Principles Into Action |
-Learn about context and population -Be clear about why information isgathered -Do not gather information that isnot needed -Assess individuals in context |
-Start with the least intrusivequestions
-Use assessment to promote healthand reduce harm -Avoid assumptions and stereotypes |
|
|
Tweak |

|
|
|
|
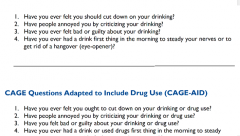
Alcohol Questions |
|
|
|
|
Alcohol Withdrawal |
Uncomplicated (peak day 2,cessation day 4 or 5) -Hand, tongue, eyelid tremor, N& V, tachycardia, HTN, headache, insomnia, irritable, depression Withdrawal delirium (1 week ofcessation) -Course tremor, tachycardia,sweating, vivid hallucinations, delusions, agitated, fever |
|
|
|
Intimate Partner Violence |
-Spousal violence/violencecommitted by current/former dating partners -Spousal abuse: physical/sexual violence,psychological violence, or financial abuse within current/former marital relationships, including same-sex spousal relationships |
-May include physical/sexualassault, verbal abuse, imprisonment, humiliation, stalking, denial of access tofinancial resources, shelter, or services-Gender is a key risk factor
|
|
|
Sexual Assault |
-Canadian CriminalCode identifies sexual assault andsexual touching as crimes -Four levels of sexual assault -Forced sexual activity withoutphysical injury |
-Sexual assault with a weapon orverbal threats-Sexual assault causing bodily harm-Aggravated sexual assault
|
|
|
Child Abuse and Neglect |
-Most provinces/territories requirethe public and health care providers to report suspected child abuse. -Child abuse and IPV often overlap. |
-Physical -Sexual -Neglect -Emotional |
|
|
Elder Abuse and Neglect |
-Physical abuse or neglect, failureto provide basic services, psychological abuse or neglect (failure to provide stimulation),financial abuse or neglect |
-Inflicted by any persons in asituation of power or trust-In home or institutions-Older women at higher risk thanolder men
|
|
|
Effects of Violence on Health |
Direct effects of physical injury -bruises, fractures, etc Chronic health problems: -Chronic pain -Neurological |
-Gastrointestinal -Gynecological •Chronicpelvic pain •Unintendedpregnancy •STIs,including HIV•Urinarytract infectionsMental health problems: -Depression -Suicidal thoughts/attempts-Symptoms of post-traumatic stressdisorder -Substance abuse
|
|
|
Health Care Providers’Responses to IPV |
-There is inconclusive evidence as to whether routine screening is effective.
-Greater detection of abuse did not necessarily lead to meaningful responses. |
-Women report negative experiences with health care providers who focus on physical consequences rather than wider effects and context of IPV.
|
|
|
Assessing for IPV
|
-All care “trauma- andviolence- informed”
-High index of suspicion for abuse -Assessing collaboratively, relational approach -Physical examination-Documentation -Women who are victims of IPV will disclose when they feel confident enough to do so. |
-The health care provider can:-Assume majority of patients have history abuse some form
-some may be currently experiencing abuse-Provide care appropriate for those histories of abuse, if hasn't been disclosed-Routinely inquire about home/worklife effects on health |
|
|
Anticipating Abuse |
-Up to 50% of all women haveexperienced some form of abuse -7% of Canadian women are currentlyin abusive relationships -More isolated = more vulnerable |
-Have a high index of suspicion whenpatients present with direct injuries, chronic pain, substance use
|
|
|
When Abuse Is Disclosed |
-Assess level of risk and develop a safety plan. -Identify personal strengths and supports. -Identify appropriate goals with the woman, in collaboration with other health care providers. -Conduct a thorough assessment. |
-Ensure objective, un biased documentation.-Take photos of injuries.-Use verbatim statements in documentation where possible.
|
|
|
HCP’s Responses to Elder Abuse andNeglect |
-Complicated -multiple health, physical, andcognitive challenges are present -Long-term abusive relationships vs.newly abused -Provincial mandatory reporting -varied and controversial |
-Canadian Centre for Elder Law(2011)
-summary of legislation for eachprovince and territory |
|
|
HCP’s Responses to Child Abuse
|
-harm related screening outweighs benefits
-High number of false positives -Reporting suspicion of child abuse mandatory -similar to IPV attention to: •Greater vulnerability of children •developmental stage of child -Neglect/emotional abuse most common |
-Parents not only possible perpetrators -Most allegations are not substantiated -Stress removal child from parents -Obligation to provide good care to parents -Nursing role child “rescuer” expense relationship with parents or child/parent relationship |
|
|
Physical Examination |
-Complete head-to-toe exam - Multiple factors can contribute to bruises in older adults -Medications and abnormal blood values -Underlying hematological disorders -Accidental bruising (one extremities) |
Children -Significant trauma -injury more severe temporary redness of skin -Suspicion when bruising in infants, bruising “atypical” places, or bruising shape of an object-Canadian Paediatric Society guidelines for head trauma, including “shaken baby syndrome” |
|
|
History - Abuse |
-Prior abuse -History of traumatic injuries -Mental health exam |
|
|
|
Documentation |
-Detailed, objective, unbiased notes -Include “exceptionallypoignant” statements that specify the perpetrator and threat -Don't sanitize language, either used by patient or quoted by patient and attributed to perpetrator |
-use the words of the child-Use of injury maps-Photographic documentation
|
|
|
Assessing for Risk of Homicide |
-In Canada, spousal homicide of women 3-4 times higher than men -Danger assessment -Map abuse on a calendar |
-Note overall score•More‘yes’ than ‘no’?-Follow-up
|
|
|
Subjective Data: Health History Male Genitourinary System |
-Frequency, urgency, and nocturia -Dysuria -Hesitancy and straining -Urine colour -Past genitourinary history -Penis: pain, lesion, discharge -Scrotum: self-care behaviours, lump-Sexual activity and contraceptiveuse-Sexually transmitted infectioncontact |
Preparation: -Position -Apprehension regarding exam Equipment needed -Gloves -Occasionally need (Equipment for specimen collection)
Penis—Inspect and palpate -Skin ( no lesions) -Glans (Palpate, any discharge) -Urethral meatus -Pubic hair -Urethral discharge |
|
|
Objective Data: Physical Exam Male Genitourinary System |
Scrotum—Inspect and palpate -Skin – no skin breakdown -Testis- Epididymis -Spermatic cord-Any mass•Notecharacteristics•Transillumination |
•Check for hernia—Inspect andpalpate–Patient standing and straining down–Palpation technique•Inguinal lymph nodes—Palpate–Horizontal chain along groin andvertical chain along upper inner thigh
|
|
|
Self-Care: TesticularSelf-Examination |
-Teach testicular self-examinationfor testicular cancer; early detection and cure rate of almost 100% -Signs: lump, pain, heaviness, ordull ache -Risk factors: |
-Age15 to 49-Delayeddescent of testicles-Familyhistory -Abnormaldevelopment of testicle- T = Timing; S = Shower; E =Examination
|
|
|
Subjective Data: Health History Questions Female Genitourinary System |
-Menstrual history -Obstetrical history -Menopause -Self-care behaviours -Urinary symptoms -Vaginal discharge -Past history - Sexual activity -Contraceptive use -STI risk reduction -Sexually transmitted infection(STI) contact |
|
|
|
Objective Data: Physical Exam Female Genitourinary System |
Preparation -Lithotomy position and draping
-Measures to enhance comfort duringexam -Mirror pelvic examination Equipment -Gloves -Goose-necked lamp with a stronglight -Graves speculum -Pederson speculum |
-Large cotton-tipped applicators(rectal swabs)-Materials for cytological study -Lubricant -External genitalia—Inspection-Skin colour -Hair distribution-Labia majora -Any lesions-Labia minora -Urethral opening-Vaginal opening-Perineum -Anus |