Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
220 Cards in this Set
- Front
- Back
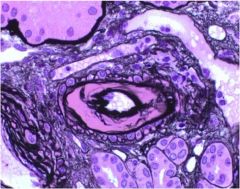
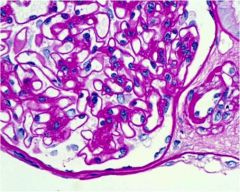
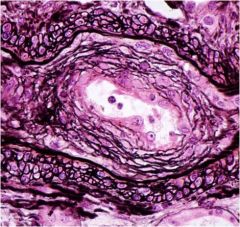
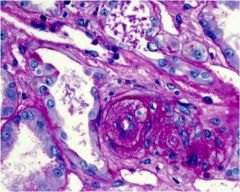
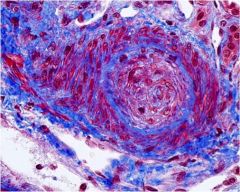
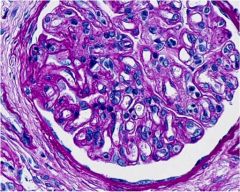
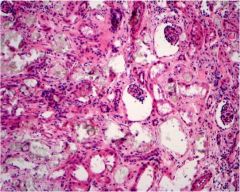
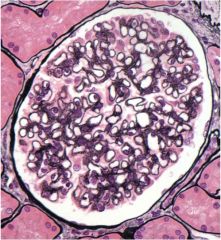
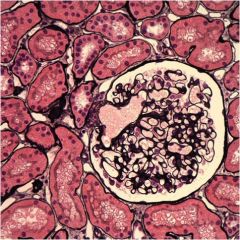
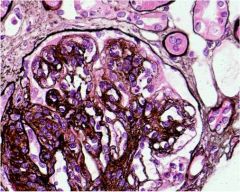
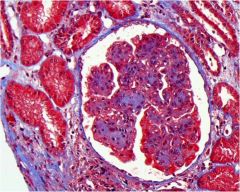
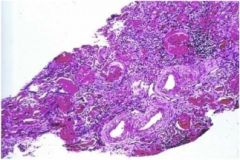
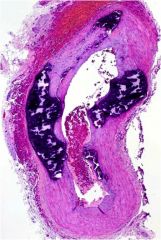
What is underlying chronic condition is most likely responsible for the pathology seen on this silver stain?
|
"Benign" hypertension. This is hyaline arteriolosclerosis. Note the thickening of the arteriole wall.
|
|
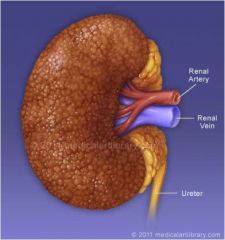
This patient has hypertension. What is the name of this pathology?
|
Benign nephrosclerosis.
|
|

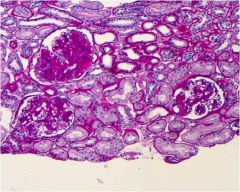
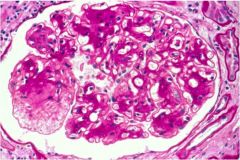
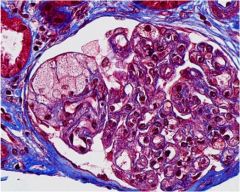
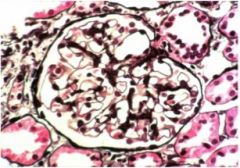
Acute or chronic glomerulosclerosis?
|
Chronic - hence the sclerosis (scarring)!
|
|
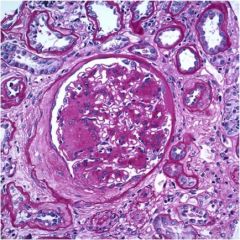
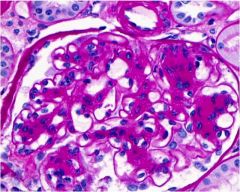
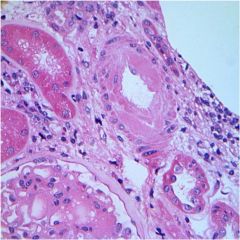
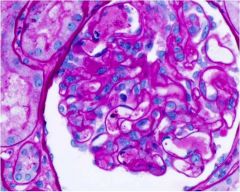
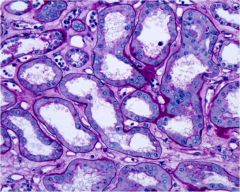
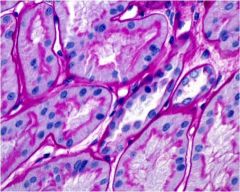
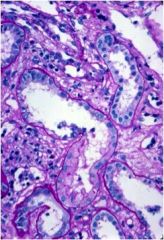
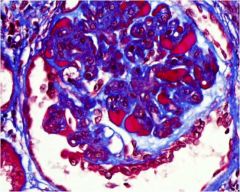
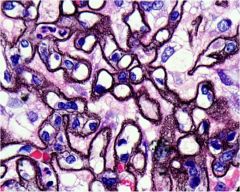
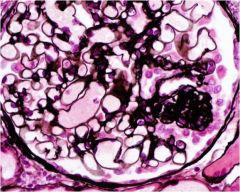
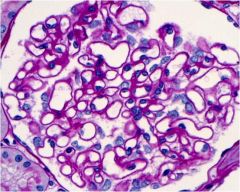
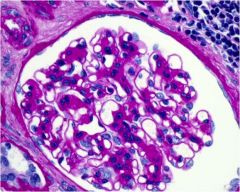
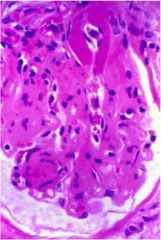
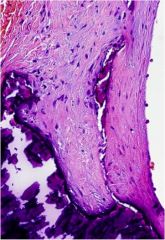
What features of diabetic nephropathy can be seen on this slide?
|
Mesangial expansion, basement membrane thickening
|
|
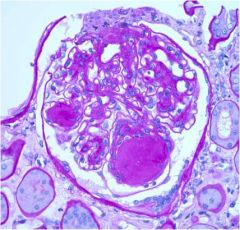
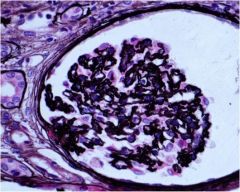
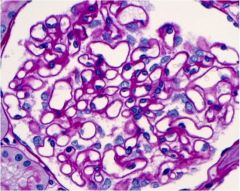
Aside from mesangial expansion, what diabetic nephropathy histopath is visible in this image?
|
Capsular drop (on the right edge of Bowman's capsule)
|
|
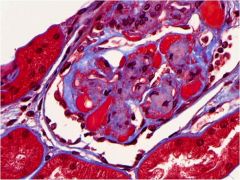
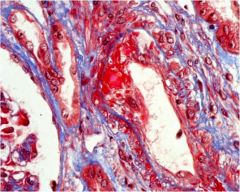
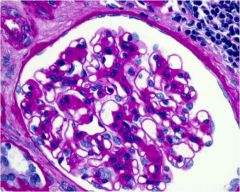
This patient has diabetic nephropathy. What process is shown by the bright red areas?
|
Hyalinosis (insudate of plasma proteins out of the capillaries)
|
|
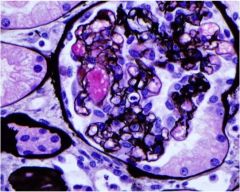
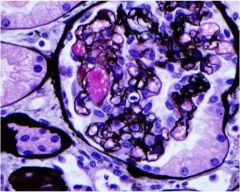
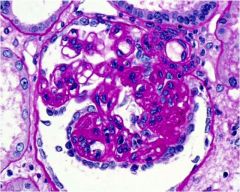
What are these?
|
Kimmelstiel-Wilson lesions, diabetic nephropathy
|
|
What part of the glomerulus is thickened in this patient?
|
The mesangium and the GBM. This patient has diabetic nephropathy.
|
|
What chronic condition does this patient most likely have?
|
Diabetic nephropathy causing mesangial expansion
|
|
In addition to mesangial expansion, what other diabetes-related lesion is seen on this image? (Hint: look at the arteriole)
|
hyaline arteriosclerosis
|
|
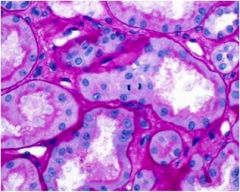
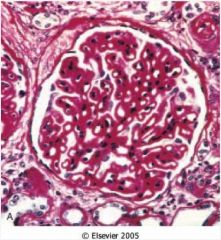
Is this kidney normal?
|
NO. The basement membranes are thickened due to diabetic nephropathy.
|
|
What has happened to this mesangium, in addition to expansion?
|
mesangiolysis due to diabetic nephropathy
|
|
What has happened here?
|
Diabetic nephropathy (mesangial expansion)
|
|
This patient has malignant hypertension. What has happened?
|
fibrinoid necrosis
|
|
This is hyaline arteriosclerosis. In the absence of other pathology, what is the most likely underlying condition?
|
"Benign" hypertension.
|
|
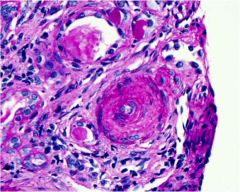
Does this patient have benign or malignant hypertension?
|
Malignant. This is hyperplastic arteriosclerosis with "onion skinning."
|
|
Does this patient have benign or malignant hypertension?
|
Malignant - hyperplastic arteriosclerosis - "onion skinning"
|
|
What is the cause of this hyperplastic arteriosclerosis?
|
Malignant hypertension.
|
|
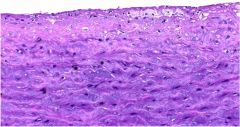
Is this kidney normal?
|
Yes.
|
|
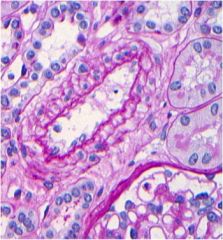
Is this normal kidney stained with PAS or H&E?
|
PAS
|
|
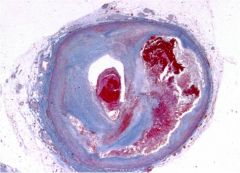
This is a renal artery. What is the diagnosis, and how does it occur?
|
Renal artery stenosis, occurs via fibromuscular dysplasia OR atherosclerosis
|
|
What type of cell has hypertrophied in this case of malignant hypertension?
|
smooth muscle hypertrophy
|
|
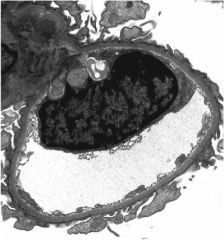
What pathology is seen in this slide of thrombotic microangiopathy?
|
capillary aneurysm filled with foamy macrophages
|
|
What substance fills these capillaries?
|
Fibrin. This is thrombotic microangiopathy.
|
|
What has happened in this case of thrombotic microangiopathy?
|
ischemic wrinkling
|
|
What has happened to the basement membrane in this case of thrombotic microangiopathy?
|
splitting
|
|
What has happened to the endothelium in this case of thrombotic micronangiopathy?
|
swelling, vacuolation
|
|
What is going on with this kidney?
|
Fibrin clot from thrombotic microangiopathy
|
|
What is going on with this kidney?
|
Fibrin clot from thrombotic microangiopathy
|
|
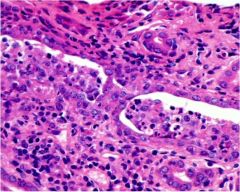
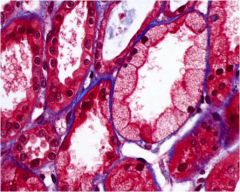
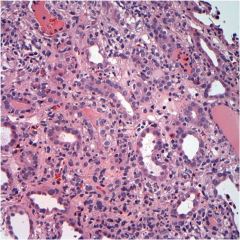
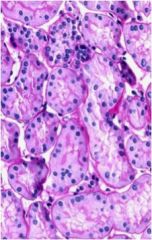
This patient has neutrophils in the lumen of her renal tubules. What illness does she have?
|
acute pyelonephritis
|
|
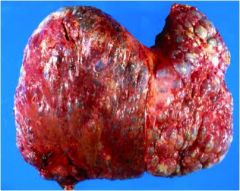
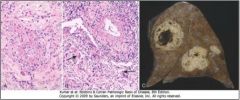
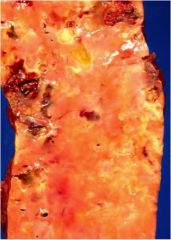
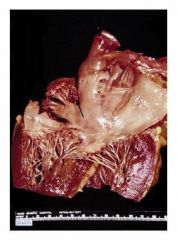
What might kill this patient suddenly?
|
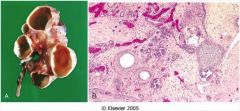
This patient has ADPKD. This is his liver. He is most likely to die suddenly of a ruptured Berry aneurysm in the circle of Willis. (Hepatic or renal failure would kill him slowly.)
|
|
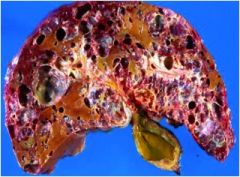
What disease does this patient probably have?
|
autosomal dominant polycystic kidney disease (ADPKD)
|
|

Diagnosis?
|
autosomal dominant polycystic kidney disease (ADPKD)
|
|
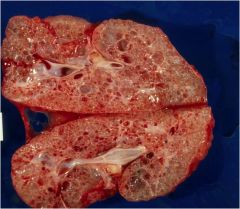
This kidney was removed from a neonate before emergency renal transplantation. Diagnosis?
|
ARPKD
|
|
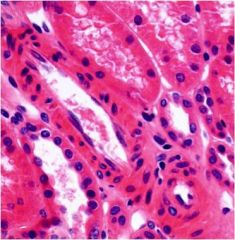
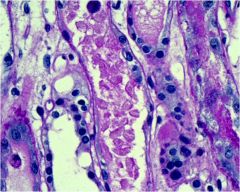
What has happened to these tubules?
|
Acute tubular necrosis. Note they are edematous and dilated. The epithelium is flattened, and the renal tubular cells have lost their brush border.
|
|
Find the mitosis in the image. If this patient has acute renal failure and will probably recover, what disease does he have?
|
acute tubular necrosis
|
|
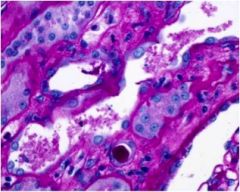
What is in the renal tubular lumens of this patient with acute tubular necrosis?
|
necrotic material (sloughed renal tubular epithelial cells)
|
|
This patient has acute tubular necrosis. What type of crystals has most likely formed?
|
oxalate crystals
|
|
These are oxalate crystals. If this patient was recently exposed to contrast, what is the most likely diagnosis?
|
acute tubular necrosis
|
|
What substance fills the tubules of this patient with acute tubular necrosis?
|
sloughed renal tubular epithelial cells
|
|
What process can be seen in this acute tubular necrosis specimen?
|
vacuolization of renal tubular epithelial cells
|
|
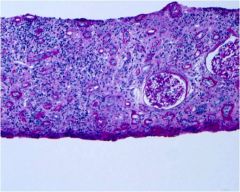
This patient has interstitial nephritis. Is it acute or chronic?
|
chronic
|
|
What is the most common cause of abdominal mass in the newborn (seen here). Is it malignant or premalignant?
|
Cystic renal dysplasia, usually caused by downstream obstruction. NOT malignant or premalignant.
|
|

What has happened to this patient who has been on dialysis for 5 years?
|
dialysis-associated renal cysts
|
|
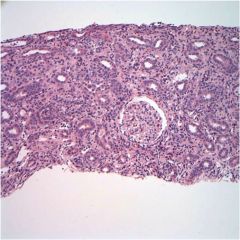
This patient has interstitial nephritis. What is the most common cause?
|
Idiosyncratic reaction to antibiotics (synthetic penicillins, sulfonamides, rifampin). Can also be caused by thiazide diuretics and possibly NSAIDs.
|
|

What is the cause of this patient's illness?
|
Obstruction. This is hydronephrosis.
|
|
What inflammatory cell can be seen here, and what is the diagnosis?
|
Eosinophils, interstitial nephritis.
|
|
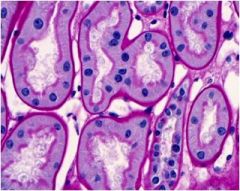
Is this kidney normal, or does the patient have ATN? How can you tell?
|
This is a normal kidney. Among other things, the brush border would most likely be destroyed in ATN.
|
|
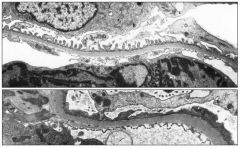
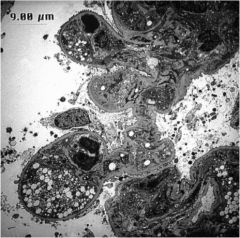
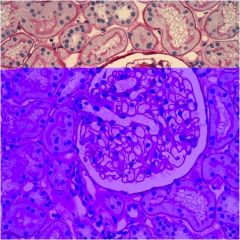
Which visceral epithelium is normal (top or bottom)?
|
Top is normal. The visceral epithelium (podocytes) are effaced on the bottom picture. They have lost the negative charge that normally keeps them apart.
|
|
Diagnosis (cardiac)?
|
congestive heart failure
|
|
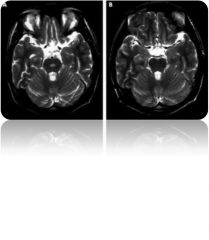
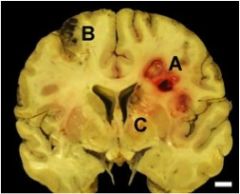
What is the cause of the syndrome seen here?
|
The image shows osmotic demyelination syndrome occurring in the pons. The cause is overly rapid correction of chronic hyponatremia causing rapid shrinkage of brain cells and leading to demyelination.
|
|
Diagnosis?
|
acute tubular necrosis
|
|

What is the significance of this cast?
|
This is a hyaline cast. There is usually no significance.
|
|
Normal kidney or acute tubular necrosis?
|
normal kidney
|
|

What is the significance of this cast?
|
This is a RBC cast implying acute postinfectious glomerulonephritis (usually post-strep).
|
|
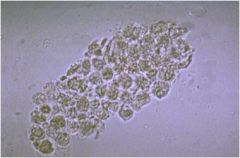
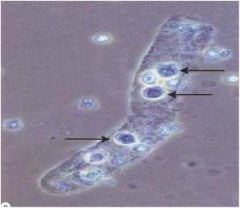
What is the most common cause of this finding in the urine?
|
This is a WBC cast. The most common cause is acute pyelonephritis. If the urine is sterile and the failure is acute, WBC casts imply acute tubulointerstitial nephritis.
|
|
These casts are found in the urine. Diagnosis?
|
Acute tubular necrosis. These are renal tubular epithelial casts.
|
|

A patient presents to the ED in acute renal failure. You perform an ultrasound to rule out this condition. Diagnosis?
|
Hydronephrosis caused by an obstruction.
|
|
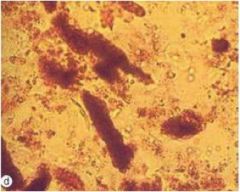
These are muddy brown casts. Diagnosis?
|
acute tubular necrosis
|
|
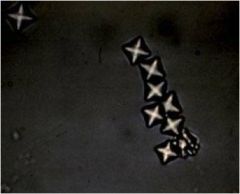
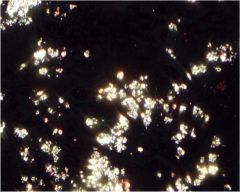
A patient with these crystals in his urine has ingested ethylene glycol. What type of crystals are these?
|
Oxalate. They can have various appearances depending on urine pH.
|
|

This patient is undergoing induction chemotherapy for acute lymphoblastic leukemia. These crystals are found in her urine. What are the crystals made of?
|
Uric acid, from tumor lysis syndrome
|
|
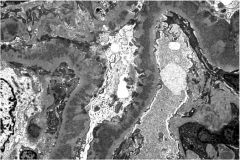
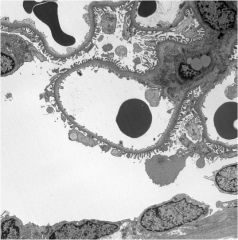
Are these deposits subepithelial or subendothelial? What are the "spikes" between them?
|
These are subepithelial deposits typical of membranous nephropathy. The "spikes" between the deposits are composed of GBM.
|
|
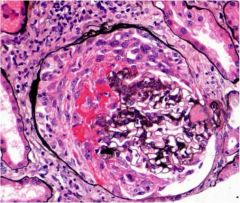
What protein fills Bowman's space in this image of crescentic glomerulopathy?
|
fibrin
|
|
What is wrong with this glomerulus?
|
It is hypercellular.
|
|
Are these deposits of IgG granular or linear?
|
granular, signifying that circulating immune complexes have deposited in the GBM
|
|
What is the red stuff in this glomerulus?
|
hyaline
|
|
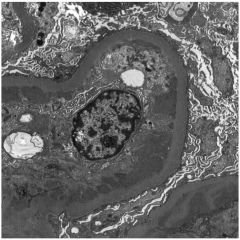
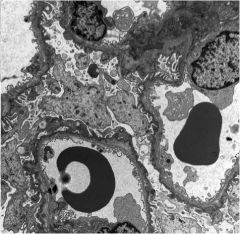
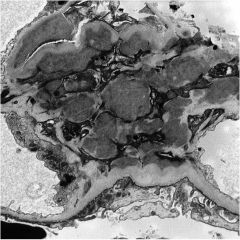
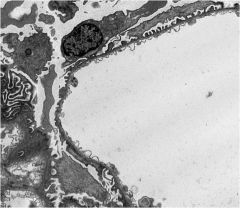
Identify the capillary lumen, Bowman's space, and the mesangium.
|
Capillary lumen = the circle in the middle (and others on the sides). The dark circle in the lumen is an RBC. You can also ID the lumen by noting the "bubbly" or "scarf-like" appearance of the endothelium (fenestrations). Bowman's space is the large space on the lower left. You can see the foot processes. The mesangium is the grey structure in the upper right, which borders both the capillary endothelium and the foot processes.
|
|
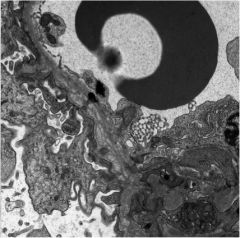
What is the squiggly dark shape in the upper left?
|
An RBC. This will help ID the capillary lumen.
|
|
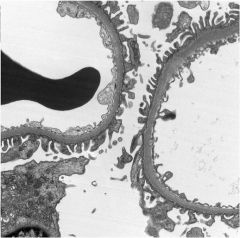
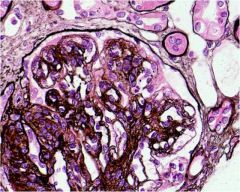
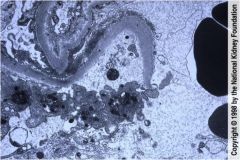
What pathology is highlighted by this silver stain?
|
GBM thickening typical of membranous nephropathy.
|
|
These thickened GBMs are typical of what renal disease?
|
membranous nephropathy
|
|
This is a glomerulus with membranous nephropathy. Are the deposits subepithelial or subendothelial?
|
Subepithelial (cannot tell from the picture)
|
|
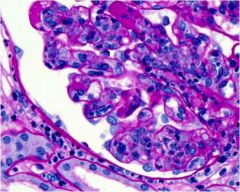
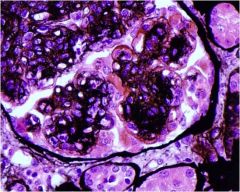
What has occurred in the glomerulus of this diabetic patient?
|
Mesangial proliferation.
|
|

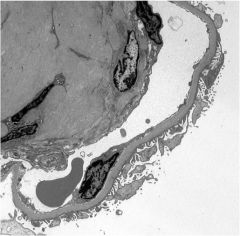
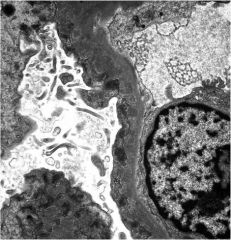
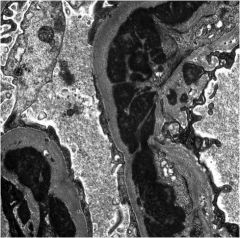
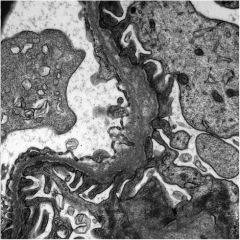
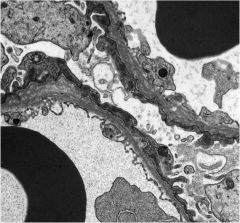
Identify the visceral epithelium (podocytes), GBM, and endothelium (capillary wall).
|
Top: podocyte. Middle: GBM. Bottom: endothelium with fenestrations.
|
|
What stain has been used on this normal glomerulus?
|
silver stain
|
|
Describe the pathology seen here.
|
No pathology, this is a normal glomerulus.
|
|
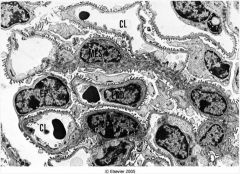
Identify a capillary lumen in this normal glomerulus.
|
Lower left, with RBC in center. Also, the space at the top labeled CL.
|
|
Does this image show focal or segmental sclerosis?
|
Segmental sclerosis (part of a glomerulus). Focal refers to part of the kidney.
|
|
Are these deposits subepithelial or subendothelial?
|
subepithelial
|
|
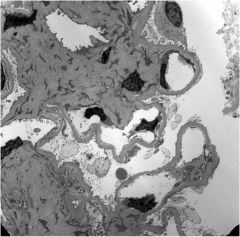
What subtle pathology is seen in this image?
|
thickened capillary loop basement membranes
|
|
What classic histopathological feature is seen here?
|
"tram tracks" (duplication of the GBM)
|
|
What is thickened in this image: the mesangium or the GBM?
|
GBM
|
|
This image shows double contours of the GBM. What is the diagnosis?
|
membranoproliferative glomerulonephritis
|
|
This patient has membranoproliferative glomerulonephritis. Are the deposits subepithelial or subendothelial?
|
subendothelial
|
|
This patient has subendothelial deposits, as seen on this EM. Diagnosis?
|
membranoproliferative glomerulonephritis
|
|
In addition to subendothelial deposits, what pathology is seen in this image of membranoproliferative glomerulonephritis?
|
lobular accentuation caused by mesangial thickening
|
|
The mesangium is thickened in this image. Does this patient have diabetic nephropathy or membranoproliferative glomerulonephritis?
|
MPGN (note lobular accentuation)
|
|
What pathologic process does this glomerulus demonstrate?
|
segmental sclerosis (not focal- that refers to some of the glomeruli, not parts of 1 glomerulus)
|
|
This is a glomerulus. Diagnosis?
|
minimal change disease (normal except for effacement of foot processes)
|
|
This GBM has a "basket weave" pattern. Diagnosis?
|
Alport syndrome
|
|
Will this patient present with nephrotic or nephritic syndrome?
|
Nephritic syndrome. The basket weave pattern in the GBM is pathognomonic for Alport syndrome, a type of hereditary nephritis.
|
|
In addition to nephritis, what might this pediatric patient present with?
|
Sensorineural hearing loss and vision problems
|
|
What gene is most likely defective in this patient?
|
"Basket weave" GBM indicates Alport syndrome. Gene = a5 subunit of type IV collagen
|
|
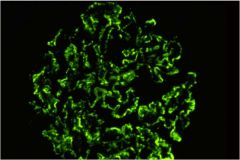
This immunofluorescence shows linear deposits. What type of antibodies form the immune complexes
|
anti-GBM
|
|
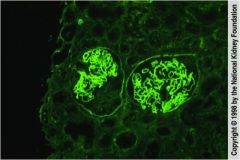
How do you know that this IgG stain detected anti-GBM antibodies?
|
Because the fluorescence is linear, indicating that the antigen is intrinsic to the GBM.
|
|
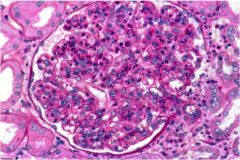
What type of inflammatory cells are seen in this image of acute proliferative glomerulonephritis, poststreptococcal type?
|
neutrophils
|
|
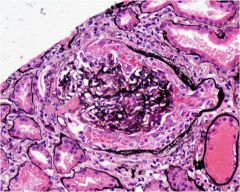
What pathologic event most likely occurred to form this crescent?
|
rupture of the capillary loop basement membrane
|
|
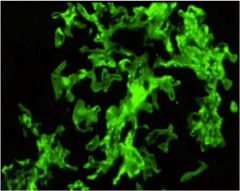
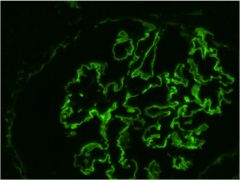
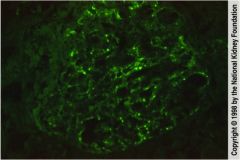
This is an immunofluorescence stain for IgA. Where are the deposits?
|
in the mesangium
|
|
Where are these glomerular deposits?
|
the mesangium (IgA nephropathy)
|
|
What can be seen in the upper left corner of this image of IgA nephropathy?
|
mesangial deposits
|
|
The mesangium has proliferated in this patient, who is NOT diabetic. Diagnosis?
|
IgA nephropathy
|
|
This patient's renal biopsy has this appearance. One week ago the patient had a sore throat. Diagnosis?
|
acute proliferative glomerulonephritis, poststreptococcal type. Note the granular appearance on IF.
|
|
This image shows the glomerular capillary basement membrane rupturing. What will form in the glomerulus?
|
crescent
|
|
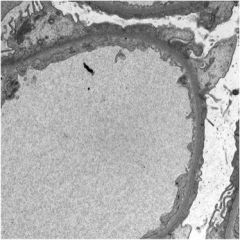
Diagnosis? (Hint: look at the GBM)
|
thin basement membrane nephropathy
|
|

What is causing this patient's renal artery stenosis?
|
fibromuscular dysplasia
|
|

What is causing this patient's renal artery stenosis?
|
atherosclerotic plaque
|
|
This is a silver stain of a glomerulus. Is it normal or not?
|
yes, normal
|
|
What common condition is the most likely cause of this patient's renal pathology?
|
hypertension. this is 'benign' nephrosclerosis
|
|

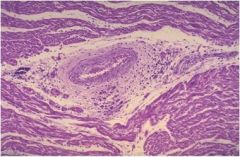
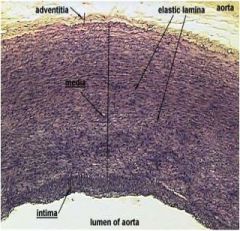
What has happened to this large artery with giant cell arteritis?
|
The intima is thickened and the elastic lamina has ruptured.
|
|
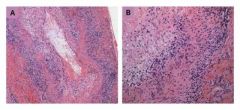
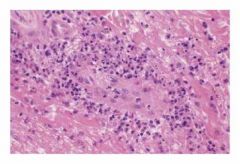
This is a large artery. Diagnosis?
|
Giant cell (temporal) arteritis. Transmural inflammation (left) with giant cells (right).
|
|
Is the entire temporal artery involved?
|
This is giant cell (temporal) arteritis. The entire temporal artery is likely NOT involved, as GCA is segmental. However, involved areas will have panarteritis (transmural).
|
|
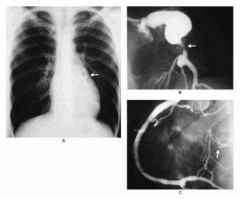
This child has a coronary artery aneurysm. Diagnosis?
|
Kawasaki disease
|
|

This patient has a medium vessel vasculitis. Diagnosis?
|
Polyarteritis nodosa.
|
|

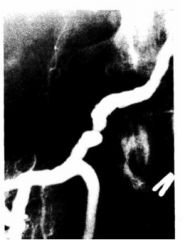
This angiogram shows the renal arteries of a patient with polyarteritis nodosa. What viral infection is associated with this illness?
|
Hepatitis B
|
|
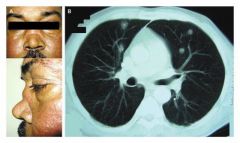
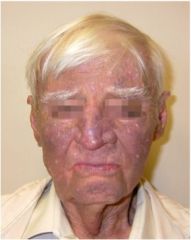
Diagnosis?
|
Wegener granulomatosis (w/ saddle nose deformity)
|
|

Will this patient have positive pANCA or cANCA?
|
cANCA most likely
|
|
How do you diagnose this disease?
|
with a tissue sample, e.g. from kidney or lung
|
|

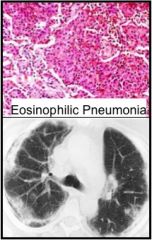
What inflammatory cell would be found on biopsy?
|
This is Churg-Strauss syndrome. You would see eosinophilic granulomas.
|
|

Diagnosis?
|
Henoch-Schonlein purpura
|
|
This patient has Henoch-Schonlein purpura. What is the median age of onset?
|
4 years
|
|
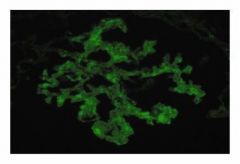
This is immunofluorescence of a glomerulus stained for IgA. Diagnosis?
|
Henoch-Schonlein purpura with mesangial IgA deposits
|
|

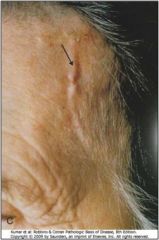
Diagnosis?
|
Coarctation of the aorta
|
|
Is this a branch retinal artery or vein occlusion? How can you tell?
|
Artery, because there's no hemorrhage
|
|

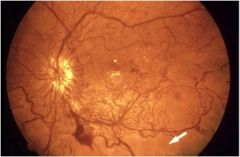
Is this a branch retinal artery or vein occlusion? How can you tell?
|
Vein, because there's hemorrhage
|
|

What is the cause of this "cherry red spot" (Block 9)?
|
There is a central retinal artery occlusion causing ischemia (edema) everywhere but the cherry red spot. This spot is supplied by collaterals.
|
|
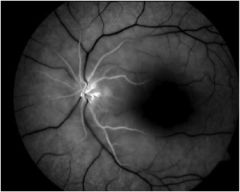
Where is the normal tissue - the black patch or the surrounding area?
|
The black patch is actually normal. This is a central retinal artery occlusion; the black area is normal and supplied by collaterals.
|
|
Central retinal artery or vein occlusion?
|
Vein, because there is hemorrhage
|
|
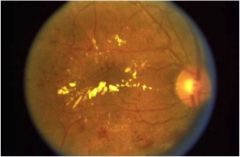
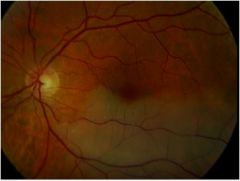
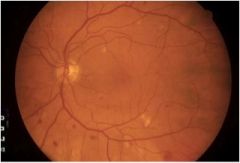
Diagnosis and finding?
|
Diabetic retinopathy with cotton wool spots
|
|
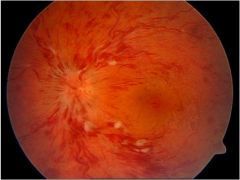
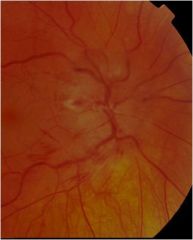
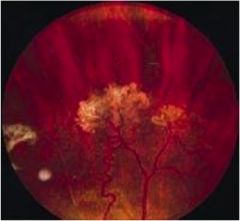
What type of diabetic retinopathy is this?
|
proliferative
|
|

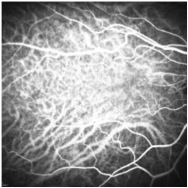
Does this angiography show the retinal or choroidal vasculature?
|
Retinal
|
|
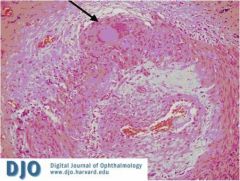
What is the arrow pointing to in this case of giant cell arteritis?
|
A giant cell!
|
|

What is the name of this finding, caused by a cholesterol embolus?
|
Hollenhorst plaque
|
|
Does this angiography highlight the choroidal or retinal vessels?
|
choroidal
|
|
What has happened to the optic nerve?
|
Ischemic optic neuropathy
|
|
Diagnosis?
|
Mild diabetic retinopathy with dot-and-blot hemorrhages.
|
|
What hematologic disorder does this patient with retinopathy have?
|
Sickle cell disease
|
|
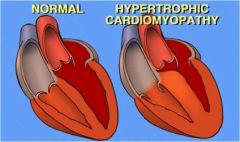
What is notable about the heart with hypertrophic cardiomyopathy?
|
Asymmetric enlargement of the ventricular septum.
|
|
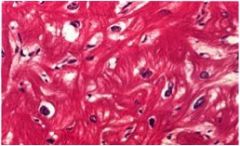
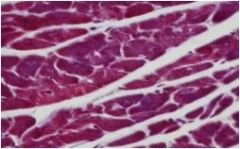
Are these cardiac myocytes normal?
|
No, they are disorganized. This is hypertrophic cardiomyopathy.
|
|
What are the two most common causes of this condition?
|
ischemic heart disease and hypertension
|
|
Are these cardiac myocytes normal or not?
|
normal
|
|
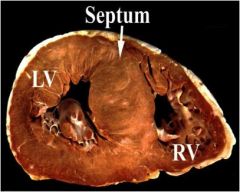
What part of this heart is asymmetrically enlarged?
|
ventricular septum
|
|
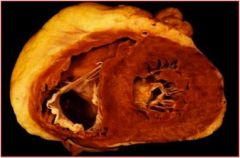
What is the most likely cause of this left ventricular rupture?
|
MI
|
|
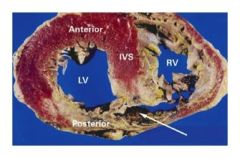
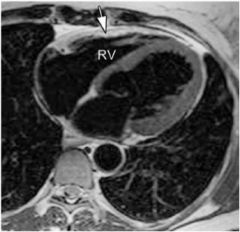
What is the arrow pointing to?
|
RV rupture, likely post-MI
|
|
Does this patient have "benign" or malignant hypertension?
|
Benign. This is hyaline arteriolosclerosis.
|
|

Does this patient have "benign" or malignant hypertension?
|
Malignant. This is hyperplastic arteriolosclerosis.
|
|
This is a blood vessel. Diagnosis?
|
Atherosclerosis.
|
|
What type of atherosclerosis is this?
|
Complicated plaque.
|
|
What type of atherosclerosis is this?
|
fatty streak
|
|

This has been stained with oil red O. What type of atherosclerosis is it?
|
fibrous plaque
|
|

This is a fibrous plaque. What are the crystal-like things?
|
Cholesterol clefts, an artifact of processing that leaves holes where cholesterol used to be
|
|

What type of atherosclerosis is this?
|
fibrous plaque
|
|
What type of arteriosclerosis is this?
|
Monkeberg's "medial" calcific stenosis ("medial" in quotation marks because it's really intima invading the media)
|
|
Is this arteriolosclerosis, Monkeberg's "medial" calcific stenosis, or atherosclerosis?
|
Monkeberg's
|
|

Patients with supraventricular arrhythmias can be taught this method...
|
carotid sinus massage
|
|
What's wrong with this heart? (Hint: patient had A-fib)
|
Thrombus in left atrial appendage
|
|
What Block 9 condition might this alleviate?
|
Valsalva maneuver can alleviate supraventricular tachycardias.
|
|
What antiarrhythmic has this patient taken?
|
amiodarone
|
|
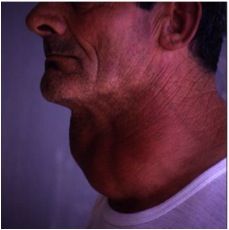
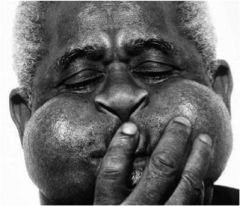
This patient has an arrhythmia. Why does he also have goiter?
|
He probably took amiodarone, which can cause hypo- or hyperthyroidism (it contains iodine!)
|
|
Diagnosis?
|
arrhythmogenic right ventricular dysplasia
|
|
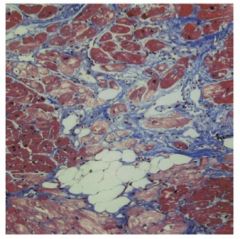
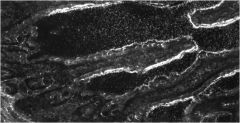
This is the right ventricle at autopsy. Diagnosis?
|
arrhythmogenic RV dysplasia
|
|
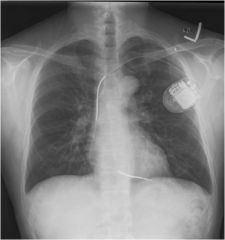
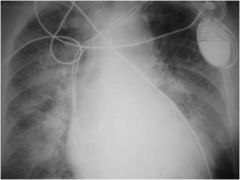
What is in this patient's chest, and why?
|
implantable cardioverter defibrillator (ICD) - most likely history of VT or VF
|
|
How long ago did this patient most likely suffer Strep throat?
|
This is acute rheumatic fever, so about 1-5 weeks ago.
|
|

This patient has aortic stenosis. What is the most likely cause?
|
Calcific aortic stenosis ("senile AS") is caused by chronic damage to the valve. This patient does not have a bicuspid valve or other condition that would predispose him to AS.
|
|

Diagnosis?
|
Aortic stenosis secondary to bicuspid aortic valve.
|
|
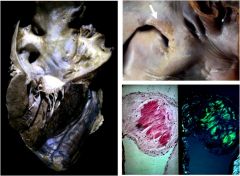
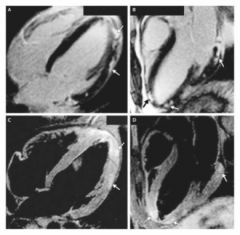
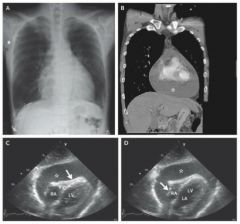
This patient has a rheumatic disease that involves the heart. Diagnosis? (Hint: look at bottom right picture)
|
cardiac amyloidosis
|
|

What type of cardiomyopathy is this? What percentage of cardiomyopathies are this type?
|
Dilated CM, 90% (10% hypertrophic).
|
|

What pathogen most likely precipitated this inflammatory reaction in the heart?
|
Group A beta-hemolytic Streptococcus pyogenes
|
|

How might this patient present?
|
This patient has hypertrophic cardiomyopathy. One common presentation is syncope on exertion.
|
|

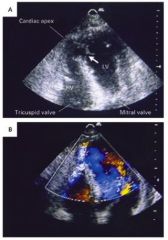
This echocardiogram of the heart shows...
|
mitral stenosis, most likely secondary to rheumatic fever
|
|

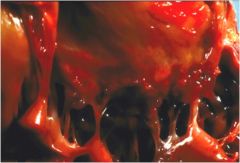
What has happened to this mitral valve?
|
myxomatous degeneration
|
|

Assuming this valve is anatomically normal, which valve is it? Why? What process has degraded it?
|
This is the mitral valve; it has only 2 leaflets (all other valves have 3 leaflets/cusps). It has been damaged by myxomatous degradation.
|
|
This is an image of the intestinal brush border. It has stained positive for a lipid-lowering drug. Which drug is it?
|
Ezetimibe acts at the intestinal brush border.
|
|
This is an image of the myocardium. What is this, and what is it pathognomonic for?
|
Aschoff nodule, acute rheumatic fever
|
|
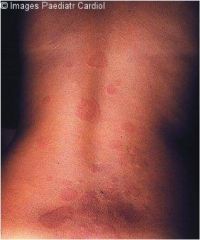
Does this patient have acute rheumatic fever or infective endocarditis?
|
Acute rheumatic fever. This is the erythema marginatum, an evanescent serpiginous rash.
|
|

Does this patient have acute rheumatic fever or infective endocarditis?
|
acute rheumatic fever; these are subcutaneous nodules
|
|

Acute rheumatic fever, or chronic damage from multiple infections?
|
Acute rheumatic fever
|
|
This patient presented with a TIA, myalgias, and splinter hemorrhages. Diagnosis? Next step?
|
Infective endocarditis. TTE followed by TEE if negative.
|
|

What are these?
|
Janeway lesions, infective endocarditis
|
|

In addition to the hands, where do Janeway lesions also commonly appear?
|
feet
|
|

What characteristic finding of infective endocarditis is the arrow indicating?
|
Osler's node
|
|
Diagnosis?
|
acute myocarditis
|
|

This is erythema migrans. Name the pathogen and the feared cardiac complication.
|
Lyme disease (Borrelia burgdorferi) can cause myocarditis.
|
|
Diagnosis?
|
Pericardial effusion.
|
|

The arrow is pointing to the space between the ___ and the ___.
|
This is the pericardial space. It is bound by the visceral pericardium (epicardium) and the parietal pericardium.
|
|

Diagnosis?
|
Massive pericardial effusion, likely chronic because if it were acute this patient would be dead!
|
|
Aortic dissections typically occur between which two layers of the aortic wall?
|
A tear in the intima leads to a build-up of blood between the intima and the media.
|
|

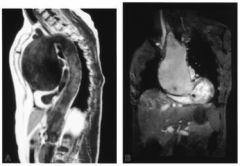
Diagnosis?
|
Aortic aneurysm - transverse aorta
|
|
Diagnosis?
|
Aortic aneurysm - aortic root
|
|

Diagnosis?
|
tetralogy of Fallot
|
|
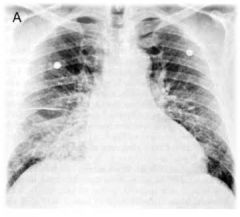
What is the cause of this patient's pulmonary edema?
|
CHF
|
|

Diagnosis?
|
COPD
|
|

This patient has pneumonia. Do you think the cause is hantavirus or Mycoplasma (atypical pneumonia)?
|
Hantavirus!
|
|

This patient recently traveled to high altitude. How high might she have traveled?
|
High altitude pulmonary edema (HAPE) can happen as low as 9000 ft. Idiosyncratic reaction.
|
|

Diagnosis?
|
hemothorax
|
|
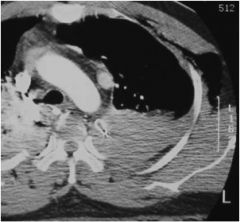
Where is the blood in this image of hemothorax?
|
pleural space
|
|

Diagnosis?
|
atypical pneumonia, likely Mycoplasma
|
|

Diagnosis?
|
pneumothorax causing atelectasis
|
|

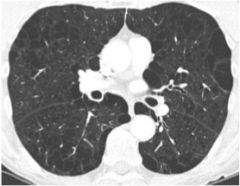
Honeycombing means...
|
pulmonary fibrosis!
|
|
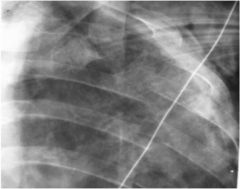
Diagnosis?
|
Multiple rib fractures
|
|
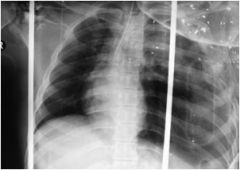
Diagnosis?
|
tension pneumothorax
|
|

What is the differential diagnosis for the anterior mediastinal mass seen on this image?
|
4 T's: thyroid (eg substernal goiter), teratoma, thymoma, terrible lymphoma
|
|

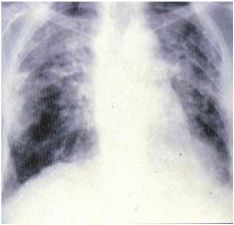
Will this patient present with obstructive or restrictive lung disease?
|
restrictive - pulmonary fibrosis
|
|
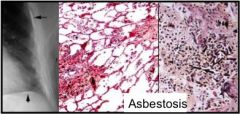
Will this patient present with obstructive or restrictive lung disease?
|
restrictive
|
|
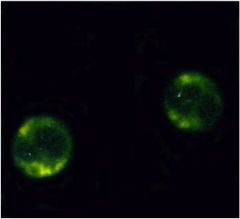
This patient has a vasculitis involving the lungs and kidneys. You stain for the antibody shown here. Diagnosis?
|
Stain shows c-ANCA (c=cytoplasmic). The diagnosis is Wegener's granulomatosis.
|
|
Obstructive or restrictive?
|
restrictive
|
|
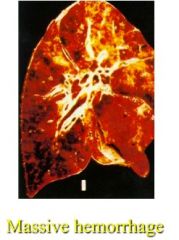
This patient, a 28-year-old man, presented with acute pulmonary hemorrhage and subclinical renal insufficiency. Most likely diagnosis?
|
Goodpasture's syndrome, aka anti-GBM
|
|
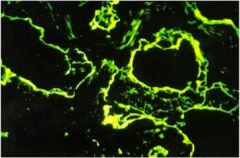
Linear IgG pulmonary renal syndrome =
|
Goodpasture's!
|
|
Farmer's lung, shown here, is one type of ____ pneumonitis that presents with restrictive lung disease.
|
hypersensitivity
|
|

Look at the line between the damaged lung and the healthy lung. Is this an anatomical division?
|
NO. This line was formed because only the damaged part was irradiated.
|
|

Can rheumatoid arthritis affect the lungs?
|
Yep. Rheumatoid nodules can form in the lungs, causing restrictive lung disease.
|
|

Diagnosis?
|
sarcoidosis (perihilar lymphadenopathy)
|
|
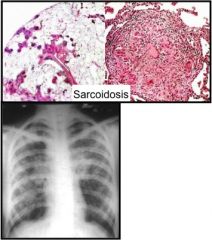
Do patients with sarcoidosis always have perihilar lymphadenopathy, as seen above?
|
No, especially not in later stages.
|
|
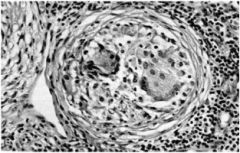
What is this, and what restrictive lung disease might look like this?
|
non-caseating granuloma suggestive of sarcoidosis
|
|

Where is this disease most common?
|
In developing countries with inadequate workers' protection laws. People get silicosis from inhaling crystalline silica dust that is produced from processing stone.
|
|

What is the cause of usual interstitial pneumonitis?
|
idiopathic
|
|
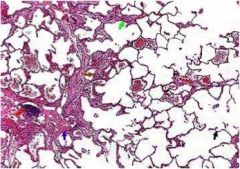
Diagnosis?
|
usual interstitial pneumonitis
|
|

This is a bronchiole. Is it normal, or does it show evidence of bronchiolitis?
|
normal
|
|

This is a bronchiole. Is it normal, or does it show evidence of bronchiolitis?
|
bronchiolitis
|
|
Diagnosis?
|
COPD
|
|

What type of lung disease will this patient have?
|
restrictive secondary to kyphoscoliosis
|
|
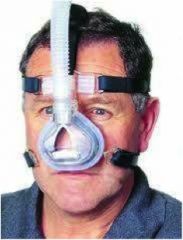
What is this guy wearing?
|
non-invasive positive pressure ventilation (NIPPV)
|