Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
125 Cards in this Set
- Front
- Back
|
Tibial plafond fracture (Pilon)
|
Ruedi and Allgower
|
|
|
Talar Fractures
|
Sneppen (1-5)
|
|
|
CT classifcation of Calcaneal fracture
|
Sanders (1-4)
|
|
|
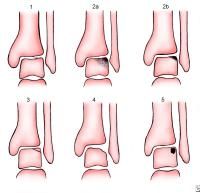
Ruedi Allgower, list stages
|
(pilon, tibial plafond fracture)
1(mild) distal tibia fx w/o displacement 2(moderate) distal tibia fx w/ displacement 3 (severe) distal tibia fx w/ displacement and comminution |
|
|
mnuemonic for describing a fracture
|
-TOE LARD LAD
-type (spiral/oblique/tran) -open/closed -extra or intra articular -length (shortened or lengthened) -angulation (transverse or sag plane) -rotation (frontal plane varus or valgus) -displacement (mild, mod or severe seperation) -location (epiphyseal, diaphyseal or metaphyseal) -anatomic alignment (good,fair,poor) -direction of fx line (medial or lateral, prox or distal, dorsal or plantar) |
|
|
nail trauma classification
|
Rosenthal
zone 1; distal to bony halanx zone 2; distal to lunula zone 3: proximal to lunula |
|
|
First MPTJ dislocation injury
|
Jahss
1. dorsal dislocation of prox phalanx w/ intersesamoid lig intact 2A. Type 1 w/ intersesamoid ligament rupture 2B. Type 2A with one sesamoid fracture 2C. Type 2B with fx of both sesamoids |
|
|
5th Metatarsal fractures
|
Stewart
1 (Jones). supraarticular fx at meta-dia junction 2. intra-articular avulsion fx at base of met 3. extra-articular avulsion of the syloid by the PB 4. intra-articular comminuted fx assoc with crush injury (base of met) 5. extra-articular avulsion fx of epiphysis in kids (SH 1) |
|
|
Jones fracture classification (met-dia 5th met fx)
|
Torg
1. acute Jones fracture 2. delayed union Jones or diaphyseal stress fracture 3. non union Jones or diaphyseal stress fracture |
|
|
AVN of 2nd met
|
Freiberg
1. non DJD, cartilage intact 2. peri articular spurs, cartilage intact 3. severe DJD, loss of cartilage 4. epiphyseal dysplasis, multiple head involvement |
|
|
Tarsometatarsal Fracture/Dislocation
|
Quenu Kuss or Hardcastle
|
|
|
Quenu and Kuss
|
-tarsaometarsal dislocation
Divergent; dislocation of lisfrancs Isolateral: partial incongruity of lisfranc joint Convergent:homolateral dislocation of lisfranc joint |
|
|
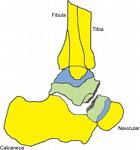
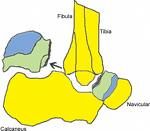
where is lisfranc ligament
|
-medial cuneiform to medial side of base of 2nd met
|
|
|
what is the lisfranc joint
|
-represents to joint between the forefoot and the midfoot
-composed of 5 tarsometatarsal joints |
|
|
Hardcastle
|
(lisfranc joint) - correlates to Quenu C-I-D
A: total incongruity of tarsomet joint B1:partial incongruity w/ MEDIAL dislocation of 1st met B2: partial incongruity w/ LATERAL dislocation of lesser mets, 1st met unaffected C1: partial divergent, 1st met is medially displaced and any combo of lesser mets are displaced laterally C2: total divergent, 1st met is medially displaced and all lesser mets are displaced laterally |
|
|
Talar Dome lesions
|
Berndt Hardy
1. compression of subchondral bone 2. partially detached osteochondral fragment 3.completely detached fragment remaining in place 4.displaced osteochondral fragment |
|
|
talar body fractures
|
Sneppen
Group 1; compression fx of talar dome (Berndt Hardy) Group 2: sagittal (type 1) or horizontal (Type 2) fracture of body Group 3: fx of posterior tubercle Group 4: fx of lateral process Group 5: crush of talar body |
|
|
talar neck fractures
|
Hawkins
1. non displaced vertical fx of talar neck 2. vertical neck fx w/ STJ dislocation 3. vertical neck fx w/ STJ and ankle dislocation (loss of all 3 blood supplies) 4.vertical neck fx w/ STJ, TN and ankle joint dislocation (loss of all 3 blood sources) |
|
|
Shepards fracture
|
posterior lateral tubercle of talus
|
|
|
Navicular fracture
|
Watson and Jones
1.navi tuber fx 2. dorsal lip fx 3A.transverse body fx, non displaced 3B. transverse body fx, displaced 4. |
|
|
Plain Film calcaneal fractures
|
Rowe
1A. medial tubercle 1B. sustentaculum tali 1C. anterior process 2A. posterior beak fx (non achilles invovlement) 2B. achilles avulsion 3. extra articular body fx 4. fx involving STJ w/o joint depression 5A. comminuted, intraarticular w/ central joint depression 5B. comminuted fx with severe joint depression |
|
|
Calcaneal fx classification that replaces Rowe 4,5 (STJ involvement)
|
Essex Lopresti
A. tongue type B. joint depression |
|
|
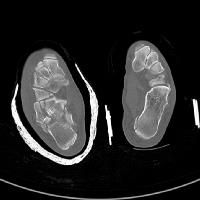
CT imaging of calcaneus
|
Sanders
1. non displaced 2. 2 part posterior facet fx 3. 3 part posterior facet fx (2 fx lines) 4. 4 part posterior facet fx |
|
|
Epiphyseal fractures
|
Salter Harris (SALTER)
1. SEPERATION of physis 2. fx from the physis up into the metaphysis (ABOVE) 3.fx up through the epiphysis 4. fx through epi,physis and metaphysis (THROUGH) 5. crush to EPIPHYSEAL plate 6. avulsion of perichondral ring (RANG's addition) |
|
|
ankle fractures
|
-danis weber or Lauge Hansen
|
|
|
Danis Weber
|
A; transverse avulsion of fibula below the syndesmosis (SAD)
B; spiral fx at the syndesmosis (SER or PAB) C; fibular fx above the syndesmosis (PER) |
|
|
SAD
|
-supination starts laterally
1. transverse avulsion of fibula at or below the ankle and/or lateral ligament rupture 2*. oblique to vertical fx of medial malleolus |
|
|
PAB
|
-pronation starts medially
1. transverse avulsion of tibia/deltoid rupture 2. rupture of AITFL and PITFL or Tillaux-Chaput or Wagstaffe 3*. short oblique of fibula (tran on lateral) |
|
|
SER
|
-supination starts laterally
1. rupture of AITFL or Tillaux-Chapet or Wagstaffe 2*. spiral oblque fx of fibula 3. PITFL or Volkman (post tibia) 4. transverse medial malleolus or deltoid rupture |
|
|
PER
|
-pronation starts medially
1. transverse fx of medial malleolus or deltoid rupture 2. tillaux-chapet or wagstaffe or rupture of AITFL and interosseous 3*. high spiral fx of fibula (Maissoneuve) 4. rupture of PITFL or Volkmans |
|
|
Hallmark of SAD
|
vertical fx of medial malleolus
-stage 2 |
|
|
Hallmark of SER
|
spiral oblique fibular fracture
-stage 2 |
|
|
Hallmark of PER
|
-Maisonneuve (high spiral oblique)
-stage 3 |
|
|
Hallmark of PAB
|
-short oblique of fibula
-stage 3 -transverse on lateral view |
|
|
if you see dislocation of the ankle joint, what stage is it
|
-end stage
|
|
|
Pilon fractures
|
Ruedi and Allgower
1. fx w/o displacement 2. fx with articualr incongruity and displacement 3. compression fx with displacement with WB segments of metaphysis |
|
|
Open Fractures
|
Gustilo and Anderson
1. wound less then 1 cm long, simple fx with little soft tissue damage 2. wound > 1 cm long, moderate soft tissue damage, moderate comminution 3. wound > 5 cm 3A. enough tissue to cover bone 3B. lack of soft tissue coverage 3C. any open fx with arterial injury that must be repaired |
|
|
how can you determine ankle diastasis on radiograph
|
-tibiofibular celar space less then 6mm on AP view
-overlap of tibia and fibula on the lateral side of 6mm or more (or 42% or greater of fibula width) -overlap of tibia and fibula of greater then 1mm on mortise view |
|
|
STJ dislocation
|
Broca
-medial STJ dislocation (MC) -lateral STJ dislocation -anterior or posterior dislocation (rare) |
|
|
basketball foot or acquired clubfoot
|
Broca- medial STJ dislocation
|
|
|
PT tendon rupture
|
Johnson and Stromm
1. peritendonitis/degeneration, mild weakness in heel rise, normal too many toes 2. elongation of tendon, weak heel rise, too many toes 3. elongation of tendon and rgid vaglus position 4. stage 3 plus lateral ankle pain and instability |
|
|
TX for Stage 1 PTTD
|
-tendon debridement and immobilization
|
|
|
Tx for stage 2 PTTD
|
-transfer of FDL for PT tendon
|
|
|
TX for Stage 3 PTTD
|
-FDL tendon transfer, TN fusion or calcaneal osteotomy
|
|
|
Tx for Stage 4 PTTD
|
-triple arthrodesis
|
|
|
peroneal tendon classification
|
Eckert and Davis
1. retinaculum and periosteum seperate from lateral malleolus 2. fibrous lip of fibula and retinauclum is torn away from fibula 3. avuslion fracture with retinaculum and fascia intact |
|
|
achilles rupture
|
Kuwada
1. partial tear of tendon 2. complete rupture, less then 3 cm gap 3. 3-6 cm gap 4. >6 cm gap |
|
|
Neuropathies and Nerve Injuries
|
Sedden and Sunderland
|
|
|
Sedden
|
Nerve injuries
-Neuropraxia; contusion but recovery is complete -Axontmesis: interruption of axon with wallerian degeneration -neurotmesis: complete severence of nerve |
|
|
Sunderland
|
nerve injuries
-1st degree: disruption of impulses w/o wallerian degeneration -2nd; disruption of axon w/wallerian degeneration distal to point of trauma -3rd; involves the axons and schwanns cells -4th: incomplete severance of nerve -5th complete severence of nerve, big gap between nerve endings |
|
|
what is the worst degree of burn
|
3rd degree: full thickness of skin and may go to bone, and are anesthetic
|
|
|
ABCDE's of trauma
|
-Airway
-Breathing -circulation -disability or neurologic status -exposure (take cloths off) |
|
|
what criteria must a spiral fracture meet to be a spiral fx
|
-fx line must be two times longer then the transverse diameter
|
|
|
which type of bone has a greater healing potential
|
-cancellous bone; has good vascularity and support structure
-metaphyseal has better healing then epi and diaphyseal bc it has more cancellous bone |
|
|
Jones Compression to reduce swelling and edema in trauma
|
-WAWAWA
-webril (undercast padding) -ACE not stretched -webril -ACE 20-30% stretch -webril -ACE 50-75% stretch |
|
|
why is there a high non union of sesamoid fractures
|
-the sesamoids are avascular
|
|
|
ilfelds disease
|
-agenesis of one or both sesamoids
|
|
|
which is the most dfficult type of MPJ dislocation to treat
|
-Jahss type 1: dorsal dislocation of prox phalanx with sesamoids and interses lig intact
-sesamoid ligaments and soft tissue are intact, so it is hard to close reduce, open reduction is necessary |
|
|
this type of MPJ dislocation (Jahss) will look like a mallet toe
|
-Jahss 2; dorsal dislocation of proximal phalnx with intersesamoid ligament rupture
|
|
|
Fleck sign
|
-small avulsion fragment in between the 1st and 2nd metatarsal bases
-pathognomonic of lisfranc;s dislocation |
|
|
what is the difference b/w delayed and non-union
|
-it is a factor of time
-non union is a fx that doesnt heel after 9 months -delayed union is a fx whose healing rate is below average -delayed unions are capable of healing, non union are not biologcally capable of healing |
|
|
list the two types of non unions
|
-avascular and hypervascular
-hypervascular (hypertrophic) are more common -avascular are inacapable of biologic reaction |
|
|
Tx of hypertrophic non union
|
-since they are capable of biologic activity bone stimulator and cast immobilization
|
|
|
Tx of atrophic (avascular) non unions
|
-these non unions are inert, so surgically clean the fracture site and bone graft is inserted with internal or external fixation
-bone stimulat can be applied with cast immobilization |
|
|
if a non union has a positive bone scan, which type of non union is it
|
-hypervascular non union
|
|
|
define malunion
|
-malalignment or malposition of fracture fragments
-so any bone that does not heal itself in anatomic position |
|
|
etiology of non-unions
|
-excessive motion at the site
-loss of blood supply -gap -infection -inc age of pt -necrosis of bone by overheating saws in sx |
|
|
Pseudoarthrosis
|
-cessation of healing with fibrous tissue remaining b/w the fracture fragments
-some pseudoarthrosis form a false joint with synovial fluid evident |
|
|
name a bone graft subsitute
|
-coralline hydroxyapatite substances from marine invertebrates
|
|
|
which is the MC fractured vertebra with calcaneal fracture
|
L1
-also do a whole body asessment with calc fx because other fx are common , so is compartment syndrome |
|
|
Mondors sign
|
-ecchymosis that extends from the heel into the arch of the foot and sometimes up the calf in calc fx
|
|
|
crucial angle of gissane
|
125-140 degrees
-angle formed by the articular surface of the calcaneus on lateral view -increases with joint depression fx |
|
|
Bohlers angle-
|
-25-40 degrees
-decreases with joint depression factors -angle formed by a line from the highest point of the anterior process of the calc to the highest part of the posterior articualr surface adn another line from the same point on the posterior articular surface and the superior part of the calc tuberosity |
|
|
2 calcaneal classifications based soley on plain films
|
-rowe
-essex lopresti -(sanders is CT) |
|
|
how can you test to see if your pt has a fx of the sustentaculum tali
|
-flex and extend the hallux, the FHL sliding under a fx tli will cause pain
|
|
|
why are fracture blisters commonly seen in calcaneus fractures
|
-they are a subcutaneous response to bleeding
-the high cancellous content of calcaneus bleeds excessively |
|
|
osteochondral talar dome lesions
|
Berndt hardy
-DIAL A PIMP -DF, Inversion: Anterior Lateral -PF, Inversion: Medial Posterior |
|
|
medial talar dome lesions
|
-no episode of trauma
-deeper and cup or triangle shaped -heal well -caused by PF, Inversion -occur in Medial posterior dome |
|
|
lateral talar dome lesions
|
-caused by trauma
-shallow and wafer shaped -heal poorly and cause degenerative changes -caused by DF, Inv -occur in ant lateral dome |
|
|
Aviators Astragalus
|
-forced DF of the foot
-Hawkins Type I : vertical fracture non displaced of the talar neck |
|
|
which Hawkins fracture (talar neck) has the highest rate of AVN
|
-Type 3 (vertical talar neck fx with displaced STJ and ankle joint)
-Type 4 (vertical talar neck fx with displaced STJ, ankle and TN joint) -all 3 blood supplies are interrupted with 3 and 4 -AVN causes intractable pain |
|
|
Hawkins sign
|
-sign of viability of the blood supply following fx of the talus
-the subchondral bone atrophy 6-8 weeks after fx is due to hyperemia of this area causing bone resorption |
|
|
Shepards fx can be confused with what ossicle
|
-os trigonum of the talus
|
|
|
what and where is the watershed area of the achilles
|
-area of avascularity
-2-6 cm proximal to the calcaneal insertion |
|
|
positive Thompson test
|
-foot does not PF when calf is squeezed
-achilles rupture |
|
|
criteria for sx correction of achilles
|
young pt or athletic pt
|
|
|
what retinaculum is important structure n maintaining the position of the peroneal tendons behind the fibula
|
-superior peroneal retinaculum
|
|
|
anterior drawer test for ankle sprains
|
-greater then 5mm from the contralateral sign is considered positive
|
|
|
inversion stress test for ankle sprains (aka talar tilt)
|
-greater then 10 degrees when compared to contralateral ankle
|
|
|
open fracture classification
|
Gustilo Anderson
|
|
|
puncture wound classification
|
Resnick
1. superficial/cutaneous 2. subcutaneous or articular w/o infecton 3A. subcutaneous or articualr w/ signs of infection 3B. bone penetration w/o infection 4. bone penetration w/osteo |
|
|
Patzakis
|
-incidence for osteomyelitis
Zone 1: toe to met head (50% chance of osteo) Zone 2: distal calc to met heads - midfoot (17% chance) Zone 3: calcaneus (33% chance of osteo) |
|
|
Berndt Hardy
|
|

|
Freiberg Stage 4
|
|

|
Freiberg Stage 2
|
|

|
Hawkins 1
|
|
|
Hawkins 2
|
|
|
Hawkins 3
|
|

|
Quenu and Kuss - convergent
Hardcastle A |
|

|
Ruedi Allgower 2
|
|

|
Ruedi Allgower 3
|
|

|
Ruedi Allgower 1
|
|

|
Ruedi Allgower 1
|
|

|
Ruedi Allgower 3
|
|
|
Sanders 3
|
|

|
Tillaux fx (ant lateral tibia)
|
|
|
two most common bacteria in puncture wounds
|
1. staph aureus
2. beta hemolytic strept |
|
|
organism in osteomyelitis
|
pseudomonas and staph
|
|
|
dog and cat bite organisms
|
pasteurella
|
|
|
human bite organism
|
eikenella
|
|
|
farm machinery organism
|
clostridium
|
|
|
how many bacteria are required to infect a wound
|
10^6/mm^3
|
|
|
what is primary wound closure
|
surgical wound closure
|
|
|
what is secondary wound closure
|
granulation tissue allows the wound to heal from the inside out
|
|
|
tertiary wound closure
|
-delayed primary closure
-the use of primary closure after the wound has been open for a period of time |
|
|
glass or wood will show up on a radiograph if it is what size?
|
greater then 5 mm
|
|
|
As far as wounds go, when do you give Tetanus Toxoid(TD) and when do you give Tetanus Immune Globulin (TIG)
|
Clean Wounds - give TD
Tetanus prone wounds - give TD and TIG |
|
|
most common compartment of the leg to have compartment syndrom
|
-anterior compartment
-deep posterior is 2nd most common |
|
|
list the 6 P's of compartment syndrome
|
-pain (hallmark of muscle and nerve ischemia)
-pain with stretch -parasthesia (numbness from nerve compression) -pulses present until very late in syndrome or is artery is crushed -pressure (tense, swollen compartment) -paresis (muscle weakness) |
|
|
what is normal compartmental pressure of the foot, when is a fasciotomy recommedned
|
0-5 mmHg
-perform a fasciotomy at 30 mmHg |
|
|
what is a better calculation for comparment pressure
|
Distolic pressure - compartment pressure
-when this difference is <30, intervention is needed |
|
|
Volksmands contractures
|
-hammertoes, clawtoes, ankle equinus and cavus caused by compartment syndrome
|
|
|
Transverse lines of park (harris lines)
|
-transverse linear bone patterns in the metaphysis
-lines result from a temporary slowdown of longitudinal growth during injury or illness -appear after trauma, when a child has been immobilized in bed from fracture, may appear after generalized illness or osteomyelitis |
|

|
Harris Park Lines
|
|
|
Physeal injury classification
|
Salter Harris
|